Management of Alopecia
Raymond J. Konior
Steven Gabel
Burns, traction, infections, autoimmune disease, neoplasms, radiation exposure, psychological disorders, and chemotherapy all can cause hair loss in humans (Table 196.1). The most common type of hair loss in men and women, however, is androgenetic alopecia (AGA), also known as male pattern baldness (MPB). This form of alopecia affects scalp follicles with a genetic potential to androgen inhibition, resulting in the conversion of susceptible terminal hairs to vellus hairs. The hair follicles most likely to demonstrate AGA are in the frontotemporal and the crown regions of the scalp. Several different surgical options are available for restoring hair growth on a balding scalp. The procedure of choice for any given individual will depend on many factors. These include (a) patient’s age, (b) degree of baldness, (c) density within the donor region, (d) hair texture, (e) contrast characteristics of the hair and skin, and (f) patient expectations.
A classification system for MPB is essential for planning and comparing the results of different surgical procedures. The Norwood system, the one most often used for men, organizes MPB into seven categories, ranging from class I (minimal frontotemporal recession) to class VII (a very narrow, horseshoe-shaped band of hair in the temporal and low occipital regions) (1). For women, the Ludwig classification system divides hair loss into three grades, ranging from grade I (minimal hair loss) to grade III (severe, generalized thinning) (2). Table 196.2 lists treatment options for MPB.
MEDICAL TREATMENT OF ANDROGENETIC ALOPECIA
Attempts to medically manage MPB are nothing new. Hippocrates, in about 400 bc, prescribed several concoctions composed of animal and plant products to treat baldness.
Ideally, the medical treatment of AGA should be directed against dihydrotestosterone (DHT), the active agent involved in MPB. Finasteride (Propecia), which has been used for years to manage prostate hypertrophy, was approved by the U.S. Food and Drug Administration (FDA) for the treatment of MPB in 1997. Finasteride is a competitive and specific inhibitor of type II 5a-reductase, an intracellular enzyme that converts the androgen testosterone into DHT. Two distinct 5a-reductase isozymes are found in humans. The type II 5a-reductase isozyme is primarily found in the prostate, seminal vesicles, epididymides, and hair follicles. Finasteride has no affinity for androgen receptors but works by blocking the peripheral conversion of testosterone to DHT. Using the recommended dose of 1 mg/d, finasteride produces statistically significant increased hair counts in men with mild-to-moderate degrees of AGA. Systemic therapy that reduces or interferes with androgen levels enough to stop hair loss has the potential to reduce libido and sexual potency, making this form of treatment unacceptable to some men. Drug-related sexual adverse experiences resulting in discontinuation of therapy have been reported in 1.2% of patients on finasteride versus 0.9% of patients on placebo (3,4). Finasteride is not indicated for woman and children.
Minoxidil (Rogaine) was the first drug approved by the FDA for the medical management of MPB. This drug, which traditionally had been used to treat resistant hypertension, was noted to occasionally produce hypertrichosis as a side effect of oral therapy in adults. Minoxidil functions as a potassium channel opener and vasodilator. Currently, the dosages available are 2% and 5% formulations. In men, the 5% minoxidil solution demonstrates a significant advantage over treatment with the 2% solution (5). The mechanism by which minoxidil works to stimulate hair growth remains unclear. In addition, minoxidil does not have any known effect on the production, excretion, or interactions of human androgens. Most, if not all,
hair transplant surgeons recommend the use of minoxidil and/or finasteride to the majority of their patients (6).
hair transplant surgeons recommend the use of minoxidil and/or finasteride to the majority of their patients (6).
TABLE 196.1 ETIOLOGY OF ALOPECIA | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
SURGICAL TREATMENT OF ALOPECIA
Patient Evaluation
During the first consultation, the patient’s goal of the procedure needs to be discussed. A thorough physical evaluation will need to be performed and an explanation of the surgical options available. The physician must understand the patient’s motivations and expectations regarding hairrestoration surgery. Patients who seem emotionally labile may require a psychiatric assessment to evaluate their true motivations, but most patients requesting hair replacement do not have emotional problems; they simply would prefer not to be bald.
Several factors determine what procedure, if any, is appropriate for restoring an alopecic scalp. It is not uncommon for the patient to expect more than can be accomplished with the donor area available. The major reason for rejecting a patient is an inadequate supply of donor hair relative to the patient’s final goals.
The ideal patient is one with enough donor hair to completely fill all current or potential areas of alopecia. The younger the patient, the more conservative the physician must be in estimating the donor hair present and establishing a long-term treatment plan. An accurate assessment of the donor area is required to prevent moving follicles at risk for future alopecia into cosmetically important areas on the scalp, because any future hair loss in those transplanted follicles will result in exposed scars over the scalp. In younger patients whose final hair-loss patterns cannot be determined, the physician should try to delay hair restoration until the physician is secure with the availability of donor hair.
TABLE 196.2  TREATMENT—ANDROGENETIC ALOPECIA TREATMENT—ANDROGENETIC ALOPECIA | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
Low-density donor hair may be a contraindication to hair transplantation. Patients with fewer than 40 follicular units/cm2 tend to be poor candidates for hair transplantation, unless they are willing to accept very thin hair density from the transplantation procedures. Age is not a contraindication to hair transplantation. Older patients generally have well-established patterns of alopecia that allow a more reliable assessment of the donor area.
Hair color, skin color, and hair texture are important factors in surgical hair restoration. A sharp contrast between the hair and the skin may result in an unnaturalappearing hairline. This is especially true if transplantation is performed with grafts that contain more than one follicle unit. The best hair colors for surgical hair restoration in light-skinned patients are white, salt-and-pepper, and blond. Patients with dark skin and dark hair and those with wiry hair generally are good candidates for hair restoration. Naturally curly hair appears thicker than straight hair, thereby enhancing the results of most hair-replacement procedures.
Hairline Design
The most important goal of hair-replacement surgery is to restore aesthetic balance to the face by recreating a natural, age-appropriate frontal hairline and part (7). The surgically restored hair should be easy to maintain and should not require extraordinary hairstyles for camouflage.
The mature male hairline usually demonstrates distinct triangular regions bilaterally at the junction of the frontal and the temporal hair (Fig. 196.1). These frontotemporal triangles are formed by progressive recession of the frontal hairline superiorly and the temporal hairline posteriorly.
A natural frontal hairline is convex, with the central portion positioned slightly inferior to the frontotemporal triangle region. The most anterior portion of the hairline is placed approximately 7 to 10 cm superior to the glabella. The apex of the frontotemporal triangle marks the lateral aspect of a natural hairline. Regardless of the extent of hairline recession, the apex is designed to fall on a vertical line drawn upward from the lateral canthus of the eye. Because the temporal hairline intersects the lateral extent of the frontal hairline, advanced temporal recessions require a more posterior frontal hairline. Any attempt to fill a large frontotemporal triangle as a means of compensating for
advanced temporal recessions will result in an unnatural hairline and part. Modern follicular unit grafting techniques can be used to recreate the temporal hairline in those patients with a low-lying superior temporal fringe.
advanced temporal recessions will result in an unnatural hairline and part. Modern follicular unit grafting techniques can be used to recreate the temporal hairline in those patients with a low-lying superior temporal fringe.
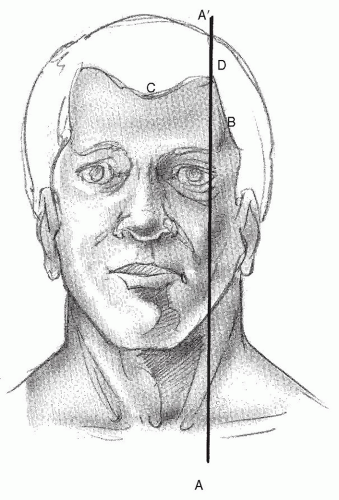 Figure 196.1 The frontotemporal triangle (BCD) is defined by the frontal and the temporal hairlines. When planning surgical restoration of the frontal hairline, the apex of the triangle is designed to fall on a vertical line (AA‘) that intersects the lateral canthus. |
FEMALE PATTERN HAIR LOSS
In hair restoration, men constitute more than 90% of the patients seeking treatment. As techniques in surgical management continue to improve and public awareness of high patient satisfaction increases, however, there are increasing numbers of women undergoing treatment for hair loss. The approach to female pattern hair loss is much different than MPB, as only 10% of women have an androgenic hair-loss pattern. Therefore, the overwhelming majority of women have hair loss for variety of other reasons, such as hormonal and autoimmune.
The workup involves recognizing the enormous psychological toll hair loss takes on a woman and using appropriate sensitivity when treating women with hair loss. Referral to an endocrinologist is usually part of the workup. Minoxidil 2% solution has been effective in treating female pattern hair loss. Increased dosages of 5% minoxidil have caused unacceptable rates of facial hypertrichosis to occur. Finasteride has not been shown to have benefit in women. Surgical hair restoration remains the only permanent treatment for hair loss in women. The same principles of adequate donor area and advanced transplantation techniques lead to better outcomes (8).
ANESTHESIA
Because most patients require multiple procedures, an adequate comfort level is essential to maintaining motivation for completion of the entire restoration process. Local anesthesia is sufficient for most hair-restoration procedures, but general anesthesia is occasionally necessary for extensive scalp reductions or flap procedures.
A preoperative sedative is commonly given before the injection of local anesthesia. Regional frontal, occipital, and temporal nerve blocks using 1% lidocaine with 1:100,000 epinephrine are performed before performing a wide-field, circumferential scalp block. This technique anesthetizes the entire hair-bearing scalp.
AUTOGRAFT HAIR TRANSPLANTATION
Okuda (9), a Japanese dermatologist, is generally regarded as the first to describe the successful use of full-thickness hair-bearing autografts for correcting alopecia of the scalp, eyebrow, and mustache areas. Hair transplantation using punch grafts was introduced in the United States in 1959 by Orentreich (10). He coined the term donor dominance to describe the fact that autografts maintain characteristics of the donor tissue when transplanted into other regions of the body. Patients followed for more than 30 years continue to demonstrate persistent hair growth following punch-graft hair transplantation (11).
Donor Hair Removal: Elliptical Strip Method
The donor site is that portion of the scalp that contains permanent hair dense enough to permit the harvesting of graft material. This area is usually found on the sides and the back of the head and is limited anteriorly by a vertical line through the external auditory canal. The superior border of the safe donor area in the midoccipital region is generally located beneath a horizontal line that intersects the superior attachment of the auricles to the scalp.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


