28

Macular Hole
Borja Corcostegui  Lorena Patricia Pimentel
Lorena Patricia Pimentel
INTRODUCTION
A macular hole is a full thickness defect of retinal tissue involving the anatomic fovea and the foveola of the eye. Macular holes were first described in 1869 by Knapp and later by Noyes in young patients mainly in relation to trauma (1, 2). Recent studies have shown that the vast majority occur as an age-related primary idiopathic condition with a female predominance in the seventh decade of life.
They may also occur in association with cystoid macular edema in the setting of inflammation, retinal vascular disease (diabetic retinopathy, vascular occlusion, hypertensive retinopathy) highly myopic eyes, macular pucker, retinal detachment, and in less frequency with lightning strike (3, 4).
PATHOGENESIS
There are three basic historical theories regarding the etiology of macular holes:
Traumatic Theory: In the first reported cases, trauma was estimated to account for as many as 50% of cases.
Cystoid Degeneration Theory: In the first histopathologic descriptions of macular holes, Coats in 1907 noted cystic retinal changes adjacent to the macular hole and thought that these changes could be caused by trauma as well as other mechanisms. In cases where there was not an immediate hole formation, trauma was believed to cause reactive vasoconstriction followed by vasodilatation, thus leading to cystic degeneration of the central macula and full thickness macular hole formation by coalescence of the cysts (5). Cystoid degeneration of the macula with secondary macular hole formation has been uncommonly described in association with a variety of conditions that include Coat’s disease, retinal vascular occlusions, severe hypertension, syphilis, solar maculopathy, arc welding maculopathy, electrocution, and vitreous traction (6).
Vascular Theory: Coats and Kuhnt believed that aging-related changes of the retinal vasculature (also characterized as ocular angiospasm) led to cystoid degeneration and subsequent macular hole formation.
Other theories:
Vitreous Theory: In 1912, Zeeman described the histopathology of the premacular vitreous condensation adjacent to foveal cystoid degeneration. Later on, as noted by Aaberg, Lister described anteroposterior fibrous vitreous traction bands, which were believed to cause macular distortion that led to tractional macular detachment, cystoid macular degeneration, and subsequently, macular hole formation (7). Based on these observations, the vitreous theory proposed that both forms of vitreous actions—preretinal condensation and contracting vitreous bands—were involved in the pathogenesis of macular holes. Around 1960, different studies began to highlight the relationship of the vitreous and the macula in eyes with macular holes. Worst described the premacular vitreous bursa as a vitreous pocket anterior to the macula and attached to it. This bursa, despite the fluid in the prefoveal interface, could exert anteroposterior traction from the margins. However, the problem with all these observations was that although the presence of a firm vitreofoveal adhesion was known, an obvious anteroposterior vitreous traction band was rarely observed.
Other investigators emphasized that the process of vitreous separation from the macula was the critical event in the pathogenesis of a macular hole. For example, Reese et al. proposed that vitreous separation from the fovea could cause avulsion of the fovea, resulting in a lamellar or full thickness macular hole (8). Because of the preponderance of women with macular hole, McDonnell et al. speculated that systemic estrogen fluctuations might promote destabilization and liquefaction of the vitreous, resulting eventually in vitreous separation with formation of a macular hole (9, 10).
Involutional Macular Thinning: Morgan and Schatz incorporated vitreous, vascular, and cystic degeneration theories and proposed that initially, choroidal vascular changes would take place and then lead to altered submacular choroidal vascular perfusion and cystic degeneration of the retina. This would cause a progressive involutional macular thinning that, in addition to vitreous traction generated from attached posterior vitreous, would cause macular hole formation (11).
Muller Cell “Cone”: In 1999, Gass emphasized the importance of the foveal Muller cell “cone,” originally described by Yamada and Hogan et al. in histological studies of the normal human foveola. These studies showed that the foveola is composed of an inverted cone of Muller glia with a truncated apex up to the external limiting membrane (ELM). Radially oriented inner cone segments that radiate toward the beginning of the outer nuclear layer of cone nuclei are located between the apex and the ELM. The base of the cone formed the umbo and extended into the clivus in the perifoveolar region (12). Gass suggested that the Muller cell cone has three important roles in the formation of a macular hole:
 Glia contain concentrated superficial xanthophyll, which migrates centrifugally during the formation of a full thickness macular hole and may be seen as a yellow spot or a yellow ring. This hypothesis is supported by the presence of xantophyll in the operculum.
Glia contain concentrated superficial xanthophyll, which migrates centrifugally during the formation of a full thickness macular hole and may be seen as a yellow spot or a yellow ring. This hypothesis is supported by the presence of xantophyll in the operculum.
 The Muller cone provides structural support for the radiating inner cone segments at the foveola and its disruption may lead to damage and atrophy of the cone cells located in this area.
The Muller cone provides structural support for the radiating inner cone segments at the foveola and its disruption may lead to damage and atrophy of the cone cells located in this area.
 Muller cells within the cone invade the prefoveolar vitreous cortex and initiate cellular remodeling and contraction. This, results in tangential traction on the foveola, centrifugal migration of photoreceptors and xantophyll, causing further disruption of the Muller cone and eventually umbo dehiscence (12).
Muller cells within the cone invade the prefoveolar vitreous cortex and initiate cellular remodeling and contraction. This, results in tangential traction on the foveola, centrifugal migration of photoreceptors and xantophyll, causing further disruption of the Muller cone and eventually umbo dehiscence (12).
Hydration Theory: Tornambe in 2003, on the basis of optical coherence tomography (OCT) 3 images and a simple model, proposed the Hydration theory. In this theory, susceptible eyes have a firm point of adherence between the posterior hyaloid face and the central macula. Stages 1A and 1B holes are explained by this foveal traction that lifts the fovea, distorting the foveal depression and displacing deeper yellow pigment. If the posterior hyaloid traction tears the inner foveal retina, OCT 3 suggests that vitreous fluid soaks into the layers of the macula initially creating a cavity in the inner retina, and then dissecting deeper, laterally accumulating in the outer plexiform layer. As the swelling increases, the hole enlarges. Because the internal limiting membrane (ILM) at its junction with the inner retina is a more rigid structure than the deeper retinal tissue, this complex (ILM/inner retina) retracts and elevates as the swelling increases. If the posterior hyaloid separates from the macula (stage 4), it may pull a tag of inner retinal tissue (ILM/nerve fiber layer/Muller cell/inner nuclear cells) (13).
CLINICAL STAGING
In 1988, Gass and then Johnson and Gass (14, 15) developed a classification scheme for idiopathic macular holes and their precursor lesions (Fig. 28-1).
Stage 1 (Foveolar Detachment). It is also known as “impending hole.” Patients usually note metamorphopsia and blurred vision, although visual acuity at this stage is reasonably good (20/20–20/60) (14–16). These symptoms may be unnoticed in the first eye involved but are the rule not the exception if the fellow eye becomes affected. There is a progressive loss of foveal depression in the absence of posterior vitreous detachment or vitreofoveal separation, associated with the appearance of an enhanced lipofucsin-colored yellow spot of approximately 100 to 150 μm at the fovea (stage 1A). The foveal retina then elevates to the level of the surrounding perifoveal retina, elongating the foveal retina around the umbo and creating a small yellow ring of 200 to 300 μm in diameter (stage 1B). Fine radiating striae surrounding the central area can be demonstrated and are best observed with retroillumination (17). Fluorescein angiography may be normal or may show fluorescence in the normally dark fovea that fades in later phases and is consistent with a window defect. The OCT scan may show a perifoveal separation of the posterior hyaloid with focal vitreous attachment to the fovea, a foveal detachment or an intraretinal space termed as pseudocyst. There is no evidence of a full thickness retinal defect. Johnson and Gass (14, 15) and Kokame (16) observed that 66% of stage 1 macular holes progressed to stage 2, while Akiba et al. and Guyer et al. reported that 37% and 10.5% of stage 1 holes progressed to stage 2, respectively (18, 19).
Stage 2 (Early Full Thickness Macular Hole). Further traction results in the formation of a small, full thickness macular hole that can be seen centrally within the yellow ring or eccentrically at the margin of the ring. The eccentric location is typical in the majority of cases (80%–90%) and it extends in a “can opener” fashion to form a crescentic hole that progresses to a horseshoe shaped hole, and eventually, to a round hole with a fully detached operculum. The visual symptoms become more severe as metamorphopsia increases and visual acuity deteriorates to a level of 20/40 to 20/100 (5, 6). The vitreous has the same appearance as that in stage 1. As the hole enlarges, the yellow ring often turns gray as the retina surrounding the hole begins to detach from the underlying retinal pigment epithelium (RPE), creating an annular neurosensory retinal detachment. Fluorescein angiography may have a more intense central fluorescence, but it is not reliable in differentiating the two stages. The OCT scan shows a small full thickness retinal defect or a rupture of the roof of the pseudocyst. Approximately, 67% of stage 2 holes progress to stage 3 as noted by Hikichi et al. (20). Kim et al. reported a 55% progression rate to stage 3 for centric stage 2 holes, and 100% for eccentric (can opener) holes, with an overall 74% progression rate of all stage 2 holes to either stage 3 or 4 (21). There are some eyes with “stage 2-like” holes that appear to have small retinal defects that remain stable for years without progression. These eyes probably do not have a true full thickness defect but rather, a lamellar macular hole that can be demonstrated with an OCT scan (14). Clinical differentiation between these two entities is not easy but it is important to decide if surgical intervention is needed. For this reason, surgery for very small or questionable full thickness macular holes should be deferred until progression can be demonstrated clinically.
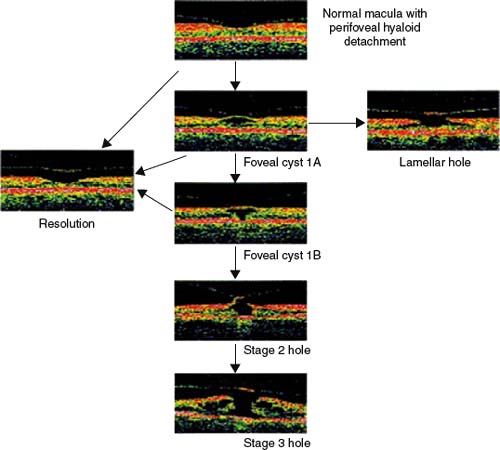
Figure 28-1. Staging of macular hole.

Figure 28-2. Left eye of a 64-year-old female patient with an initial visual acuity of 20/200 and a stage 3 macular hole with yellowish deposits at the level of retinal pigment epithelium.
Stage 3 (Fully Developed Full Thickness Macular Hole without Posterior Vitreous Detachment).
Stage 4 (Fully Developed Full Thickness Macular Hole with Posterior Vitreous Detachment).
The visual acuity drops between 20/80 and 20/200. In stage 3, vitreofoveal separation occurs at the macula and is usually only detected because of the presence of the operculum suspended on it, lying a short distance anterior to retinal plane. In stage 4, 20% to 40% of patients present evidence of posterior vitreous separation, such as partial or complete remnants of Weiss’ ring and 50% to 70% of patients present a retinal operculum that can be seen freely floating on the posterior hyaloid face (Figs. 28-2 to 28-5). In these two stages, a full thickness retinal defect of 300 to 1500 μm in diameter associated with a surrounding neurosensory retinal detachment can be easily detected clinically, although the full extent of the detachment might be underestimated, since there is often a much larger area of shallow detachment surrounding the retina around the retinal hole. Discrete white deposits, which represent nodular proliferations of RPE cells, may appear on the surface of the RPE at the base of the hole or under the surrounding retinal detachment in approximately 50% of the patients (7). In long standing cases, a pigmented demarcation line at the level of RPE may be seen surrounding the cuff of fluid along with cystic changes. Fluorescein angiography demonstrates a window defect with early fluorescence in the area of neurosensory retinal defect followed by gradual fading of the fluorescence. OCT scan shows a full thickness retinal defect with a sharp edge that changes over time to become a rounded edge and that is associated with an adjacent neurosensory retinal detachment. Intraretinal edema and epiretinal membranes may also be observed.
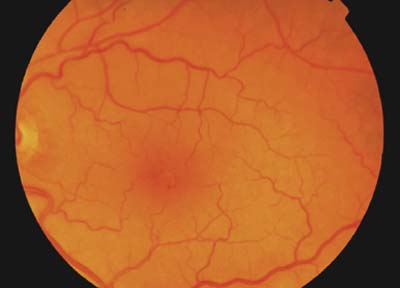
Figure 28-3. Optical coherence tomography scan shows retinal edema at the margins of the macular hole and the operculum lying in the posterior hyaloid face, which is detached.
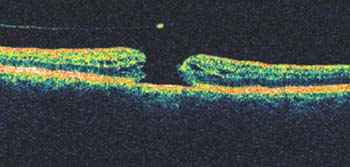
Figure 28-4. Fundus color photograph shows closure of the macular hole and some retinal pigment epithelium disturbances at the foveal area with two pinpoint hemorrhages at inferotemporal margin of the fovea. Final visual acuity improved to 20/60.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


