24
Macular Edema Associated with Vascular Occlusion
Jawad Ahmad Qureshi  Sharon Fekrat
Sharon Fekrat  Daniel Finkelstein
Daniel Finkelstein
Occlusion within retinal veins may occur in the central retinal vein, producing a central retinal vein occlusion (CRVO), or in a branch retinal vein, producing a branch retinal vein occlusion (BRVO) or a hemiretinal vein occlusion (HRVO). Approximately 2 in 1,000 persons aged 40 years or older developed a retinal vein occlusion over a 4-year period in a population-based study performed in Israel (1). In persons aged 65 years or older, this increased to 5 per 1,000 individuals.
The likelihood of some of the ocular consequences of venous occlusive disease, such as decreased visual acuity from perfused macular edema in eyes with BRVO, vitreous hemorrhage, and neovascular glaucoma, may be decreased by early diagnosis and laser treatment (2–5).
BRANCH RETINAL VEIN OCCLUSION
Occlusion of a retinal venous branch typically occurs in the seventh decade of life (6) and develops because the blood flow in the affected retinal venous branch is slowed or interrupted. It usually occurs where a retinal artery crosses a retinal vein, the retinal arteriovenous intersection (7–9). Rarely, a BRVO may occur at a site other than an arteriovenous crossing in eyes with ocular inflammatory disease.
An increased risk of developing a BRVO was noted in persons with histories of cardiovascular disease, systemic hypertension, glaucoma, increased body mass index at 20 years of age, or higher serum levels of a2-globulin in the Eye Disease Case-Control Study (10). In this study, those persons with higher serum high-density lipoprotein cholesterol levels and greater levels of alcohol consumption had a decreased risk of BRVO; diabetes mellitus was not a strong independent risk factor for BRVO (10). Other studies have suggested an increased risk of BRVO in eyes with shorter axial lengths (11–14).
Clinical Features
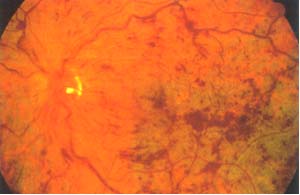
An acute BRVO is one that has been present for less than 6 months and displays characteristic ophthalmoscopic findings. In the affected distribution, variable amounts of superficial and deep retinal hemorrhage, retinal edema, venous tortuosity and dilation, and cotton-wool spots may coexist in a segmental pattern (Fig. 24-1). The presence of cotton-wool spots in the involved area, however, does not necessarily imply that the vein occlusion is ischemic. In the acute phase, the diagnosis of a BRVO is usually straightforward, unless the affected segment is either small or well perfused, with complete recovery of function. If another retinal vascular disease, such as diabetic retinopathy, coexists, or if there are several BRVOs in one eye, the diagnosis may not be so obvious.
A BRVO may lead to compromise of visual acuity or may be asymptomatic, depending on the location of the occluded segment. If the visual acuity is affected, it may be attributed to involvement of the macula with hemorrhage, edema, or ischemia. If the venous blockage is peripheral to those veins draining the macula, the macula may not be involved, and visual acuity may be unaffected. Nasal BRVOs seem less common, but this may be a result, in part, of the asymptomatic location of these occlusions (15). The superotemporal venous branch is involved more frequently (63%); the inferotemporal branch is affected in almost all other cases (15). The apex of the segmentally distributed intraretinal hemorrhage usually marks the approximate location of the arteriovenous intersection at which the occlusion occurred (Fig. 24-1). With some exceptions, the closer the BRVO occurs to the optic disc, the greater the distribution of affected retina and the more serious the sequelae (15, 16). If the BRVO occurs at the optic disc, two quadrants of the retina may be involved, whereas if the occlusion is peripheral to the disc, one quadrant or less may be affected.
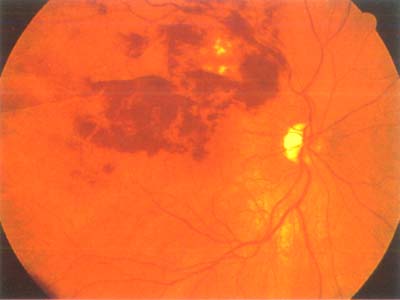
Figure 24-1. An acute branch retinal vein occlusion is characterized ophthalmoscopically by a segmental distribution of varying amounts of intraretinal hemorrhage and segmental venous dilatation and tortuosity.
A BRVO may be categorized as chronic 6 months or more after its onset. The diagnosis may be more challenging ophthalmoscopically in these eyes, because the intraretinal hemorrhage may have been mostly reabsorbed. Ophthalmoscopically, retinal capillary abnormalities, such as capillary dilation, capillary nonperfusion, microaneurysms, and collateral vessel formation, may be noted in the involved distribution. In these cases, fluorescein angiography may facilitate the diagnosis by better delineating the segmental retinal capillary abnormalities. If the occlusion is deemed ischemic, sclerosis and sheathing of the retinal vasculature in the distribution of the occlusion may also be identified.
Perfusion Status
If the ophthalmoscopic diagnosis of BRVO has been determined, it is useful to determine whether the BRVO is perfused (nonischemic) or nonperfused (ischemic), using high-quality fluorescein angiography (2). If less than five disc areas in diameter of retinal capillary nonperfusion is present in the affected distribution on fluorescein angiography, the occlusion is classified as perfused or nonischemic. If five or more disc areas in diameter of nonperfusion are present on angiography, the occlusion is classified as nonperfused or ischemic. Of eyes with a BRVO affecting one quadrant of the retina or more, about half are ischemic.
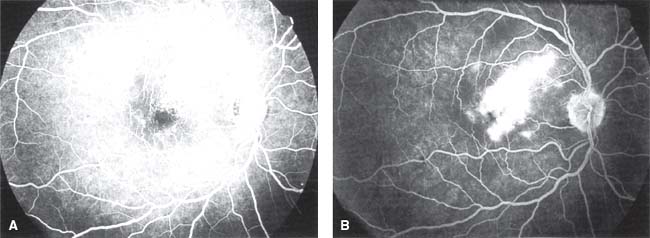
Figure 24-2. Perfused macular edema in an eye with branch retinal vein occlusion. A: The transit phase of the fluorescein angiogram shows an intact parafoveal retinal capillary network. B: Late accumulation of fluorescein dye parafoveally and in the foveal center is present.
Identification of retinal capillary nonperfusion may not be feasible on fluorescein angiography in those eyes with moderate to marked amounts of intraretinal hemorrhage, because the hemorrhage may block the fluorescein outline of the parafoveal vascular network as well as patches of retinal capillary nonperfusion. As a result, fluorescein angiography cannot be utilized diagnostically until the hemorrhage resorbs sufficiently to allow the observation of underlying capillary architecture. The hemorrhage may take up to 1 year to clear in some eyes.
Macular Edema
Macular edema may be categorized angiographically in eyes with a BRVO as perfused (nonischemic), nonperfused (ischemic), or mixed (perfused and nonperfused) (5, 17). Rarely, the macular edema may not be characterizable into one of these three classes, because it may have developed in association with a distant BRVO. After sufficient resorption of the intraretinal hemorrhage, careful evaluation of the parafoveal vascular architecture with ophthalmoscopy and high-quality fluorescein angiography is necessary to identify the type of macular edema (17). Optical coherence tomography has also become increasingly useful in evaluating, characterizing, and following macular edema.
If fluorescein angiography demonstrates an intact parafoveal retinal capillary network during the transit phase of the angiogram (Fig. 24-2A) followed by the late accumulation of fluorescein dye both parafoveally and in the foveal center (Fig. 24-2B), the macular edema is classified as perfused.
If fluorescein angiography demonstrates an irregular parafoveal vascular network with para- and perifoveal areas of retinal capillary nonperfusion (Fig. 24-3) followed by the absence of any late accumulation of fluorescein dye in the foveal center, the macular edema is classified as nonperfused.
If fluorescein angiography demonstrates parafoveal retinal capillary dilation and leakage admixed with areas of capillary nonperfusion, the macular edema is classified as mixed (17). In the late phase of the angiogram in these eyes, fluorescein dye accumulates in the foveal center. In eyes with mixed edema, however, it is not possible to discern how much of the foveal cystoid edema may be attributed to perfused edema and how much may be attributed to nonperfused edema. Spontaneous resolution of the nonperfused portion of the macular edema within 6 to 12 months may permit reassessment.
Distant macular edema may develop in an eye with a peripheral BRVO, in which the occluded venous branch is peripheral to the macular area. Fluorescein angiography may demonstrate leakage. The pathophysiology of the macular edema in these eyes has not been elucidated.
Optic-disc and Retinal Neovascularization
Approximately 40% of eyes with an ischemic BRVO develop retinal or disc neovascularization. If laser photocoagulation is not performed, approximately 60% of those that have neovascularization develop vitreous hemorrhages (2). Neovascularization of the optic disc and retina (Fig. 24-4A) may develop in eyes with an ischemic BRVO, usually within the first 6 to 12 months after onset but possible at any time within the first 3 years. Retinal neovascularization almost always occurs within the involved segment; however, rarely, it may develop outside the affected area, usually at an arteriovenous crossing.

Figure 24-3. Nonperfused macular edema is present if fluorescein angiography demonstrates an irregular parafoveal vascular network with para- and perifoveal areas of retinal capillary nonperfusion and no late accumulation of fluorescein dye in the foveal center.
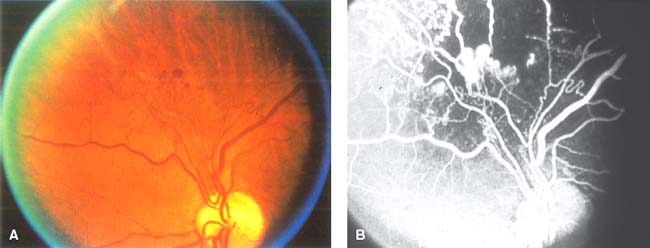
Figure 24-4. A: Retinal neovascularization may be difficult to differentiate from collateral channels in eyes with vein occlusion. B: Fluorescein angiography may help distinguish whether the abnormal vessels are true neovascularization or collateral vessels, because fluorescein leakage is more prominent from the neovascularization than from collateral vessels.
Ophthalmoscopically, disc and retinal neovascularization may be mistaken for collateral vessels. Collateral vessels may develop on the disc or within the retina along the horizontal raphe or around the site of occlusion (Fig. 24-4B). These venule-to-venule channels bypass the occluded vein and appear as dilated, and occasionally tortuous, vessels. Fluorescein angiography may help to distinguish whether these vessels are collateral or represent true neovascularization, because the fluorescein leakage is much greater from neovascularization than from collateral vessels.
Iris Neovascularization
Iris neovascularization and neovascular glaucoma are infrequent sequelae in eyes with BRVO. The coexistence of diabetes mellitus, with or without retinopathy, may increase the likelihood of developing iris neovascularization.
Pathogenesis and Histopathology
Although branch venous occlusive disease has been attributed primarily to arterial insufficiency (18), in animal studies, common manifestations of BRVO, including retinal capillary nonperfusion and secondary retinal arteriolar changes, can be duplicated by the experimental occlusion of a retinal vein alone (19, 20). In human eyes, the blocked venous branch is almost always localized to a nearby arteriovenous crossing (8). Histopathologic examination of the involved branch retinal vein has demonstrated a thrombus as the cause of the venous occlusion at the arteriovenous intersection (21); despite this, the pathogenesis of thrombus formation remains unclear. In a histopathologic study, a fresh or recanalized thrombus was present at the site of venous occlusion in each of nine eyes with BRVO (21); thus the primary event was thought to be intravenous thrombosis with secondary arterial and capillary manifestations and ultimately neovascular proliferation. Thrombus formation was not observed in any of the corresponding retinal arterioles, even though all but one of the corresponding arterioles had moderate to severe sclerosis.
Because branch venous occlusive disease almost always occurs at arteriovenous intersections (7&x2013;9, 22, 23), associated arterial disease may be in part a cause of the occlusion. Retinal arterioles cross anterior to retinal veins at approximately 55% to 70% of all arteriovenous crossings in normal eyes (7–9). The artery was located anterior to the vein at the obstructed site in 99% of 106 eyes with BRVO (8). Histopathologically, the retinal artery and vein share a common adventitial sheath at the crossing site, and the lumen of the vein may be compressed up to 33% at the site in some cases (21, 22). Atherosclerosis may contribute to increased rigidity of the crossing artery and contraction of the common adventitia, resulting in turbulent venous blood flow, endothelial cell injury, and thrombotic venous occlusion.
In an animal model, certain histopathologic sequelae develop after the complete occlusion of a branch retinal vein (19, 20, 24). Within 1 to 6 hours following the occlusion, there is a suspected elevation in intravascular pressure, resulting in capillary leakage and retinal edema. Within 6 hours to 1 week following the obstruction, necrosis of the vascular endothelium leads to exposure of the basement membrane with thrombus development. Complete microvascular stasis results, followed by the development of retinal hemorrhages. Within 1 to 5 weeks following the occlusion, irreversible capillary closure has developed, with the invasion of proliferating glial cells into the ghost vessels.
Treatment and Clinical Course
Medical Intervention
Systemic anticoagulation has not been demonstrated to prevent or alter the clinical outcome of the venous occlusion. Because the administration of anticoagulants may result in systemic bleeding complications, and because anticoagulants may promote the development of intraretinal hemorrhage acutely, anticoagulant therapy currently is not recommended. Other agents, such as troxerutin, and ticlopidine, have been suggested as potential treatments by reducing blood viscosity and improving retinal microcirculation. Studies on the use of troxerutin and ticlopidine have shown a trend toward improving visual acuity in eyes with BRVO, but the evidence to support these treatments is limited at this time (25, 26).
Laser Photocoagulation
Some basic knowledge of laser treatment techniques is essential in treating these eyes; a meticulous approach helps decrease the likelihood of developing complications. Laser photocoagulation should not be done over substantial intraretinal hemorrhage, because the energy of the laser is absorbed by the hemorrhage and may damage the nerve fiber layer, producing preretinal fibrosis. If intraretinal edema is present, higher laser powers may be necessary for adequate uptake.
The Collaborative Branch Vein Occlusion Study (BVOS) (2, 5), supported by the National Eye Institute, was a multicenter, randomized clinical trial constructed to answer three questions about the management of complications of BRVO:
1. Does grid argon laser photocoagulation improve visual acuity in eyes with visual acuity of 20/40 because of perfused macular edema (5)?
2. Does peripheral scatter argon laser photocoagulation prevent the development of neovascularization (2)?
3. Does segmental peripheral scatter argon laser photocoagulation prevent vitreous hemorrhage in eyes with neovascularization (2)?
Macular Edema
The BVOS was designed to determine if grid argon laser photocoagulation can improve the visual acuity in eyes with an acuity of 20/40 or worse resulting from macular edema from BRVO of 3 to 18 months’ duration (5). The BVOS data demonstrate that grid photocoagulation may improve the visual acuity in treated eyes. The timing of laser treatment of perfused macular edema, after the onset of a BRVO, did not affect the visual acuity. Early photocoagulation did not appear to be more beneficial. In a different nonrandomized study of 161 treated eyes with macular edema, those eyes treated 12 months or longer after the onset of the BRVO improved less than those treated within the first year (27).
Clinical information must be collected prior to treating macular edema with laser (5, 17). First, the visual acuity in the eye with the BRVO should be documented. In the BVOS, treated eyes had a corrected visual acuity better than 20/40. Second, high-quality fluorescein angiography must be feasible to demonstrate foveal dye accumulation and an absence of moderate to marked para- and perifoveal capillary nonperfusion. Hemorrhage may interfere with determination of visual acuity, angiographic interpretation, and subsequent laser treatment. Third, fluorescein-proven perfused macular edema involving the foveal center must be documented to be the cause of visual loss. Blood should not be in the foveal center, because subsequent clearing of this blood may lead to some spontaneous improvement in visual acuity. Fourth, one must be confident that the macular edema is not resorbing spontaneously. Untreated foveal macular edema of less than 12 months’ duration can improve during the first 6 to 12 months after the onset of a BRVO; approximately one third of patients may improve two or more Snellen lines of visual acuity without treatment (5). Individuals who are hypertensive or have had decreased visual acuity for greater than 1 year from macular edema, however, are less likely to regain vision spontaneously. For the nonperfused and mixed forms of macular edema, a small study suggested that the spontaneous rate of improvement was much greater, approximately 90% (17). If some capillary nonperfusion is present along the edge of the foveal avascular zone, the acuity may be more likely to improve; if larger areas of capillary nonperfusion exist at the border of the foveal avascular zone, the acuity often does not improve.
Argon laser photocoagulation was placed in a “grid” pattern within the area of vascular leakage on fluorescein angiography (Fig. 24-5) in the BVOS (5). The treatment could extend from the edge of the foveal avascular zone to the major vascular arcade. Suggested treatment parameters include a spot size of 50 to 100 mm in diameter, a 0.1-second duration, and a power setting sufficient to produce a light to medium white burn. Grid laser photocoagulation is not performed to directly and immediately close the leaking and dilated capillary vasculature; instead, laser absorption occurs at the level of the retinal pigment epithelium. Although it is not understood how the laser treatment may act in lessening edema if laser absorption occurs at this level, experimental studies in normal primates have shown a decrease in capillary diameter if this form of therapy is used (28). Grid treatment may produce retinal thinning that permits the choroidal vasculature to provide for the inner retina; this may lead to autoregulatory constriction of the retinal vasculature in the leaking area and ultimately result in decreased macular edema (28).

Figure 24-5. In the Branch Vein Occlusion Study (5), argon laser photocoagulation was placed in a “grid” pattern within the region of leakage on fluorescein angiography. Treatment extended no closer to the fovea than the margin of the capillary free zone and no farther peripherally than the major vascular arcade.
Identifying distinct landmarks may help avoid accidental laser photocoagulation of the fovea (5, 17, 29). If sufficient landmarks cannot be identified, then the treatment may be started far away from the foveal avascular zone. At the 3-month follow-up visit, fluorescein angiography outlines the previous area of grid laser photocoagulation and defines the amount of additional treatment needed. If macular edema with foveal involvement is still present, another treatment session may bring the grid treatment pattern closer to the edge of the foveal avascular zone. This staged method may be less risky and as effective as a single treatment in some cases (29).
A follow-up evaluation is recommended approximately 3 months following treatment (5). If macular edema persists ophthalmoscopically and the acuity has not improved, fluorescein angiography is suggested. If residual fluorescein leakage is observed, another session of laser photocoagulation may be necessary. In the BVOS at 3 years, treated eyes were more likely to have visual improvement, a final visual acuity of 20/40 or better, and an average visual acuity better than that of untreated eyes (5). Sixty-three percent of treated eyes improved two or more lines compared with 36% of untreated eyes at 3 years. The mean visual acuity improvement in treated eyes, however, was only one more Snellen line than in untreated eyes. Because approximately 10% of individuals with BRVO have a second venous occlusion in the same or fellow eye, the acuity gain from treatable macular edema may be important (5, 29).
Neovascularization
The BVOS sought to determine if segmental peripheral scatter argon laser photocoagulation could prevent the development of neovascularization in eyes with ischemic BRVO (2), and whether, if neovascularization develops in untreated eyes with nonperfused branch vein occlusion, segmental peripheral scatter laser photocoagulation could prevent a vitreous hemorrhage (2).
Data from the BVOS demonstrated that prophylactic scatter laser photocoagulation can decrease the likelihood of subsequent neovascularization, and, if neovascularization is already present, scatter laser photocoagulation can lessen subsequent vitreous hemorrhage (2). Treatment should cover the entire area of ischemic retina, except within two disc diameters of the fovea, and consist of medium-intensity 200- to 500-mm argon laser burns spaced one burn width apart.
Neovascularization develops in approximately 40% of untreated eyes with ischemic BRVO (2). Disc or retinal neovascularization may develop any time within the initial 3 years following a BRVO but usually appears during the first 6 to 12 months. The incidence of neovascularization may be decreased to approximately 20% if peripheral scatter laser photocoagulation is administered (2). If routine photocoagulation were applied to all eyes with nonperfused BRVO before the development of neovascular proliferation, however, the 60% that would never develop neovascularization would receive unnecessary scatter laser photocoagulation. As a result, prophylactic laser treatment in these eyes has not been advocated.
Of the 40% of untreated eyes with nonperfused BRVO that do develop neovascularization, approximately 60% develop a vitreous hemorrhage (2). If neovascularization is definitely present, as documented by fluorescein angiography in the BVOS, peripheral scatter laser photocoagulation can decrease the likelihood of vitreous hemorrhage to 30% (2).
The BVOS did not determine whether ischemic eyes should receive prophylactic photocoagulation or be observed and photocoagulated only if neovascularization should develop. Analysis of the available data suggests that there may be no benefit to treating prior to the development of neovascularization (2). If fluorescein angiography demonstrates that the BRVO is ischemic, then an examination every 4 months to look for neovascularization is suggested. If neovascularization is noted, then scatter photocoagulation is recommended to the ischemic region. Data from the BVOS suggest that laser photocoagulation following the development of neovascularization is just as effective in preventing vitreous hemorrhage as is photocoagulation prior to the development of neovascularization (2).
Vitreous Hemorrhage
A vitreous hemorrhage in eyes with BRVO usually develops either from disc or retinal neovascularization, with or without prior scatter laser photocoagulation, or from the breakthrough of retinal hemorrhage through the internal limiting membrane into the vitreous cavity. B-scan ultrasonography may be useful to rule out a traction retinal detachment and other intraocular causes of bleeding. The long-term sequelae of visual loss from vitreous hemorrhage in BRVO have not been investigated, but in some individuals, vitreous hemorrhage from neovascularization results in prolonged visual loss. In other eyes, however, the hemorrhage resolves spontaneously without resulting in permanent visual impairment.
Retinal or disc neovascularization should be excluded if a vitreous hemorrhage is present in eyes with BRVO, whether or not previous scatter laser photocoagulation has been administered. If ophthalmoscopy is not feasible because of a dense hemorrhage, fluorescein angiography or angioscopy may permit visualization of neovascularization. If a neovascular source cannot be identified, it is possible that the hemorrhage resulted from the breakthrough of retinal hemorrhage; however, this is less likely. If the vitreous hemorrhage does not clear spontaneously over time, a pars plana vitrectomy with endolaser photocoagulation is recommended, especially in eyes that have not had previous scatter laser photocoagulation.
Vitrectomy (with and without Sheathotomy)
Evidence exists suggesting that vitreomacular attachment alone may contribute to the development of macular edema in BRVO (30). Kurimoto and coworkers found that vitrectomy with separation of the posterior hyaloid resulted in decreased macular edema. Six of the seven eyes had improved visual acuity at 3 months follow up (31). Saika and coworkers reported similar results (32). Increased oxygenation of the macula, removal of vitreous traction, and tamponade of the macula by intraocular gas are possible explanations for the clinical improvements seen in these studies.
As discussed previously, the blocked venous branch in a BRVO is almost always localized to nearby arteriovenous crossing (8). It has been suggested that removal of the compressive factors affecting the vein by sectioning the adventitial sheath (sheathotomy) may be an effective treatment for BRVO (33). Osterloh and Charles reported significant visual improvement in the first report of sheathotomy (20/200 to 20/25≶ over 8 months) (34). Opermcak and Bruce reported equal or improved visual acuity in 12 of 15 patients undergoing sheathotomy. All of the patients in this study had marked resolution of edema and intraretinal hemorrhages (35). Mason and coworkers compared sheathotomy to control groups in which patients were treated with laser or no treatment. Of the 20 eyes that underwent surgical intervention, 75% percent achieved a halving of their visual angle compared with only 40% of control patients (36). In contrast, Cahill and colleagues reported 27 cases of BRVO treated with sheathotomy without a statistically significant improvement in postoperative median visual acuity (37). No randomized, controlled study evaluating the benefits of sheathotomy has been published. This procedure has been largely abandoned.
Intraocular Corticosteroids
Recently, intraocular injection of steroids has been added as an option for the treatment of macular edema. Although the exact mechanism of macular edema development from BRVO has not been elucidated, breakdown of the blood-retinal barrier is thought to play a role. A corticosteroid suspension, triamcinolone acetonide, has been shown experimentally to reduce breakdown of the blood-retinal barrier when injected intravitreally (38). A human pharmacokinetics study of nonvitrectomized eyes found a single 4 mg injection of triamcinolone to have a mean elimination half-life of 18.6 days with measurable concentrations expected to last approximately 3 months (39). The administration of intravitreal corticosteroids to treat macular edema has gained popularity due to the potential of minimizing side effects while allowing higher drug concentrations to the eye. A number of studies have reported improvements in visual acuity and macular edema by optical coherence tomography and clinically (40–48). The results appear to be transitory, requiring reinjection to maintain improvement (41&x2013;45, 48). Side effects of intravitreal corticosteroids include increased intraocular pressure, cataract formation in phakic patients, vitreous hemorrhage, sterile and infectious endophthalmitis, and retinal detachment (40,44–47,49–50).
The Standard Care vs. Corticosteroid for Retinal Vein Occlusion (SCORE) Study is a multicenter, randomized, Phase III trial sponsored by the National Eye Institute currently underway to assess the efficacy and safety of standard of care versus intravitreal triamcinolone injection for treatment of macular edema associated with CRVO and BRVO. The study has recruited 1260 patients randomized to standard care, laser treatment, intravitreal triamcinolone (IVTA) 4 mg, or IVTA 1 mg. (51). Two multicenter phase III trials evaluating the safety and efficacy of an intravitreal implant of dexamethasone (Posurdex, Allergan Inc.) for the treatment of macular edema from retinal vein occlusion are also currently recruiting patients.
ANTI-VEGF Intravitreal Therapy
Anti-VEGF (vascular endothelial) therapies such as pegaptanib sodium (Macugen; Eyetech Pharmaceuticals and Pfizer), ranibizumab and bevacizumab (Lucentis and Avastin, respectively; Genentech) may play a role in treating macular edema related to RVO and preventing neovascular complications. Further study is underway with these agents in BRVO.
CENTRAL RETINAL VEIN OCCLUSION
CRVO is a common cause of visual loss in individuals 50 years of age and older (52). In young individuals, CRVO has been termed as “papillophlebitis” and considered a different disease entity, with an assumed inflammatory cause (53). There is little basis, however, on which to differentiate these eyes from those in older individuals with CRVO, except for the younger age of these patients.
In the Eye Disease Case-Control Study (54), relationships between certain risk factors, including glaucoma, systemic hypertension, and diabetes mellitus, and the development of CRVO were suggested. Others report that increased plasma viscosity and increased hematocrit also may contribute to the development of venous occlusive disease (55).
Clinical Features
A collection of ophthalmoscopic manifestations characterizes eyes with CRVO, rarely creating a diagnostic dilemma, and includes varying quantities of superficial and deep intraretinal hemorrhage emanating from the optic disc into the peripheral fundus in all four quadrants, optic nerve-head congestion, and a tortuous and dilated retinal venous tree. A mild or chronic CRVO, however, may create diagnostic confusion. In eyes with scattered, blot-shaped, intraretinal hemorrhage, predominantly in the peripheral retina, atherosclerotic carotid artery disease should be sought as the underlying cause. In an eye with carotid insufficiency and decreased arterial perfusion, gentle digital pressure on the globe may produce pulsations of the central retinal artery. If simultaneous bilateral intraretinal hemorrhage is observed, even if asymmetric, an underlying systemic hyperviscosity disorder must be considered.
In eyes with CRVO, the clinical course varies (3, 4, 56, 57). In eyes with mild disease, the ophthalmoscopic characteristics may resolve within several months, with subtle or no sequelae. In moderate cases, some hemorrhage may persist, with retinal vascular abnormalities and macular edema. In eyes with ischemic CRVO, however, complications may develop, such as iris or angle neovascularization with neovascular glaucoma, vitreous hemorrhage, and optic-disc or retinal neovascularization, among others.
The Central Vein Occlusion Study (CVOS) collected and tabulated data to determine the visual prognosis of eyes with CRVO (4). The best corrected visual acuity, on presentation, may be a predictor of the final visual outcome. For example, if the initial visual acuity is 20/40 or better, the acuity in the affected eye is likely to remain good. If the visual acuity is 20/50 to 20/200, however, the visual prognosis varies; the acuity may improve (20%), may not change (approximately 50%), or may worsen. If the initial visual acuity is worse than 20/200, the visual prognosis is poor (80% remain the same or deteriorate), and the CRVO is usually ischemic.

Figure 24-6. A: In eyes with perfused central retinal vein occlusion, a few small, scattered retinal hemorrhages and mildly dilated and tortuous retinal veins may be present. B: Fluorescein angiography in an eye with a perfused central retinal vein occlusion demonstrates less than 10 disc areas of capillary nonperfusion. Blocked fluorescence from the scattered hemorrhage and, in some cases, a prolonged venous transit time may be present.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


