49
Macular Choroidal Melanoma
Jerry A. Shields  Carol L. Shields
Carol L. Shields
Uveal melanoma is the most common primary intraocular malignant tumor among Caucasians. The epidemiology, clinical features, diagnostic approaches, management, and prognosis of uveal melanoma have been discussed in detail in recent textbooks (1, 2). Choroidal melanomas that occur in the macular area present unique therapeutic considerations, because their treatment sometimes can cause considerable visual loss. This chapter reviews the diagnosis and management of melanomas that arise in the macular area, a region that we define as an area about 6 mm in diameter with the foveola as its center. Because recent publications (1, 2) have described this tumor in great detail, this chapter briefly reviews the diagnosis and management of macular choroidal melanoma.
CLINICAL FEATURES
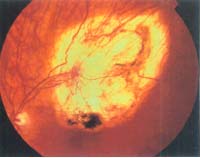
Macular choroidal melanoma can assume a variety of clinical features (1, 2). It usually presents as a sessile or dome-shaped pigmented mass located deep to the sensory retina (Fig. 49-1). If located in the macular area, it is more likely to have surface orange pigment at the level of the overlying retinal pigment epithelium. A secondary retinal detachment frequently accounts for visual impairment. Occasionally, a macular choroidal melanoma can be partly or entirely nonpigmented. With continued growth, the tumor can rupture Bruch’s membrane and assume a mushroom shape. If the tumor is amelanotic, blood vessels in the mass are visible ophthalmoscopically. In some instances, larger macular choroidal melanoma can cause total retinal detachment, cataract, congestive glaucoma, and extraocular extension. Such tumors are generally larger and carry a worse prognosis.
DIAGNOSTIC APPROACHES
In most instances, the diagnosis of macular choroidal melanoma can be made by recognition of its classic features using indirect ophthalmoscopy. The diagnosis can be supported or confirmed, however, by the judicious use of ancillary studies such as fluorescein angiography, ultrasonography, or, in more difficult cases, fine-needle biopsy (3). In cases that are atypical ophthalmoscopically, these ancillary studies assume a more vital role in diagnosis. These techniques are discussed in detail in the literature (1, 2) and are only summarized here.
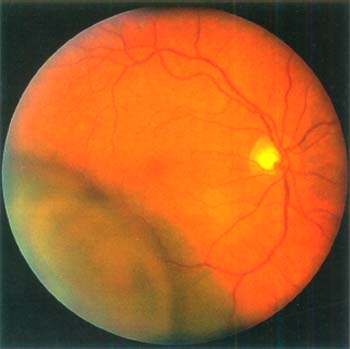
Figure 49-1. Pigmented choroidal melanoma encroaching on the foveal area.
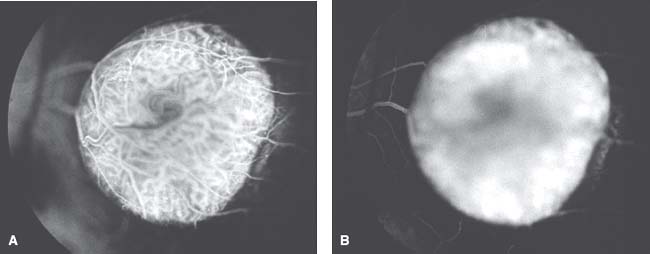
Figure 49-2. Fluorescein angiography of an elevated macular melanoma. A: Venous phase showing filling of the tumor vessels and the overlying retinal vessels (“double circulation”). B: Late angiogram showing diffuse hyperfluorescence of the mass.
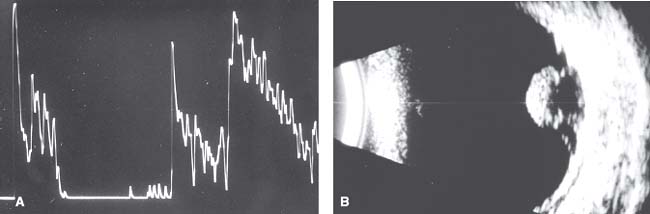
Figure 49-3. Ultrasonography of macular choroidal melanoma. A: a-Scan showing medium to low decreasing amplitude pattern. B: b-Scan showing pedunculated mass with basal acoustic hollowness and choroidal excavation.
On fluorescein angiography, a typical choroidal melanoma shows mottled hyperfluorescence in the vascular filling phases and diffuse late staining of the mass and its overlying subretinal fluid. A larger melanoma, particularly one that has broken through Bruch’s membrane, shows more clearly the characteristic double circulation in which both the retinal vessels and the choroidal vessels in the tumor are evident (1, 2) (Fig. 49-2).
On A-scan ultrasonography, choroidal melanoma typically shows medium to low internal reflectivity; on B-scan, it shows a choroidal mass pattern with acoustic hollowness and choroidal excavation (Fig. 49-3). Ultrasonography can delineate small nodules of extraocular extension of the tumor. It is particularly helpful in eyes with opaque media. Computed tomography and magnetic resonance imaging can be used to visualize uveal melanoma and to completely delineate larger areas of orbital extension (1, 2).
Fine-needle aspiration biopsy can be used diagnose choroidal melanoma in difficult cases that defy clinical diagnosis using less invasive measures (1–3). The most commonly employed technique is a trans–pars plana, transvitreal approach using a 25-gauge needle.
MANAGEMENT
There are several methods for management of macular melanoma (1, 2). The selected management should depend on factors such as the size, location, and activity of the melanoma, as well as the status of the opposite eye and the age, general health, and psychological status of the patient. Each patient should undergo a detailed ophthalmic evaluation, and the size and extent of the tumor should be carefully documented. The known risk factors for growth and metastasis should be considered (4), and the patient then should be counseled thoroughly as to the therapeutic options (5).
The details of the therapeutic methods are described elsewhere (1–3). Small lesions in which the diagnosis is questionable can be followed with serial fundus photographs and ultrasonography to document growth before undergoing definitive treatment.
Some small and medium-sized melanomas can be managed with techniques of laser photocoagulation. Laser can be used primarily for lesions less than 3 mm in thickness that have documented growth or other significant risk factors for growth and metastasis (6). Photocoagulation is used less often today because transpupillary thermotherapy in the infrared range using a diode laser delivery system has shown some promising preliminary results.
Transpupillary thermotherapy recently has replaced laser photocoagulation at some centers for treatment of selected small and medium-sized melanomas (7, 8). It involves heating the tumor using light in the infrared range by way of a modified diode laser delivery system. It gives the best results in cases of small choroidal melanomas in which growth is detected at an early stage (Fig. 49-4), but it has been used successfully for tumors up to 4 mm in thickness (1, 2).
Techniques of radiotherapy using radioactive plaque (9) or charged particles (10, 11) can be used for many medium-sized or large macular choroidal melanomas in which there is a reasonable chance of preserving some useful vision. Plaque radiotherapy is currently the most commonly employed method for treating uveal melanoma. Extensive experience with plaque brachytherapy has suggested that it offers reasonably good tumor control, can often preserve useful vision (12) (Fig. 49-5), and offers as good a systemic prognosis as enucleation. Plaque radiotherapy requires close cooperation among the ocular oncologist, radiation oncologist, and radiation physicists. It is now recognized that plaque radiotherapy can be employed to treat large melanomas, macular melanomas, ciliary-body melanomas, and extraocular extensions of melanomas (1, 2, 13, 14). Similar results have been obtained with charged-particle irradiation, but anterior-segment complications such as cataract and neovascular glaucoma seem to be worse if charged-particle treatment is employed. Although results are sometimes surprisingly good (12), radiation retinopathy can be expected in most cases of macular melanoma treated by any form of irradiation (13, 15) (Fig. 49-6).
A melanoma located in the ciliary body and peripheral choroid can be managed by local removal of the tumor using a method of partial lamellar sclerouvectomy (1, 2, 16). It is a difficult procedure that requires considerable skill and experience, but the results are often very gratifying. It is only rarely used for tumors that encroach on the macular area.
Enucleation appears to be the best treatment for larger macular tumors in which there is little hope for salvaging useful vision or tumors that surround or invade the optic nerve (1, 2). It is most often employed in younger patients with large melanomas in whom there is no hope for useful vision.
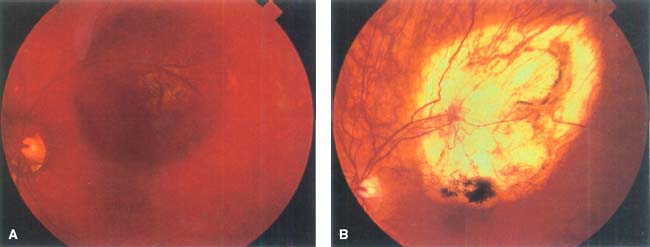
Figure 49-4. Transpupillary thermotherapy of macular choroidal melanoma located just superior to the foveola. A: Pretreatment appearance. The pigmented mass was 2.5 mm in thickness. B: Posttreatment appearance showing complete destruction of the mass.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


