Lymphoma, a malignancy of lymphoid tissue characterized by the proliferation of lymphoid cells or their precursors, is the most common nonepithelial malignancy of the head and neck. Because lymphoma typically manifests as a neck mass, otolaryngologists are frequently involved in diagnosis. However, as it is a disease treated primarily by radiation and medical oncologists, the role of the otolaryngologist generally diminishes once a diagnosis is obtained. Nonetheless, as a participant of a multidisciplinary team, it is imperative for the otolaryngologist to be well versed in not only comprehensive management of the disease but also the controversies of classification and treatment. Moreover, the otolaryngologist will often be the diagnosing physician for lymphomas that present in the head and neck, and thus a high index of suspicion must be maintained, especially for lymphomas occurring at extranodal sites.
There are two main types of lymphoma: Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL). HL is typically characterized by the orderly spread of disease through contiguous groups of lymph nodes. In contrast, NHL can manifest in extranodal sites such as Waldeyer ring, salivary glands, and thyroid in addition to occurring in the nodal basins of the head and neck.
EPIDEMIOLOGY
NHL accounts for 86% of all lymphoma cases and is the fifth most common malignancy in the United States, excluding skin cancers (
1). It is primarily a disease of adults, with less than 10% of overall cases occurring in children (
2). NHL results from chromosomal translocations in B or T/natural killer (NK) cells that lead to either the inactivation of tumor suppressor genes or activation of oncogenes (
3). B-cell lymphomas compromise roughly 90% of all NHLs; the two most common histologic subtypes are follicular lymphoma and the more aggressive diffuse large B-cell lymphoma (DLBCL) (
4). Risk factors include male gender, long-term immunosuppression, exposure to radiation or pesticides, and autoimmune diseases such as systemic lupus erythematous (
5). Infections including human immunodeficiency virus (HIV), human T-cell lymphotropic virus 1 (HTLV-1), human herpesvirus-8 (HHV-8), and Epstein-Barr virus (EBV) have also been associated with the development of lymphoma (
6).
The less common HL is a highly curable disease with an estimated 5-year relative survival of 86% (
2). The incidence of HL has a bimodal distribution, with the disease primarily occurring in young adults and patients 55 years and older (
7). Much like in NHL, risk factors for the development of HL include viral exposure, immune suppression, and familial factors (
8). Although HL originally had been subdivided into four categories, the most recent World Health Organization (WHO) classification has separated the disease into the more common classical HL and the rare nodular lymphocytepredominant HL (
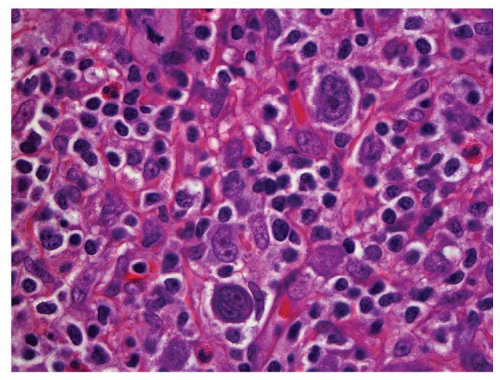
9). The diagnosis of HL is made with the identification of Reed-Sternberg cells, a binucleated or multinucleated giant cell of germinal center B-cell origin (
Fig. 128.1) (
10). HL is unique in that malignant cells compromise the minority (estimated at 0.1% to 10%) of the cellular population of the tumor (
11). Thus, obtaining ample biopsy specimen is critical for accurate diagnosis of the disease.
In 2010, the American Cancer Society estimates that 74,030 new lymphoma cases will be diagnosed and 21,530 deaths due to lymphoma will occur in the United States (
2). An analysis of the National Cancer Data Base (NCDB) revealed that the proportion of lymphoma cases among all head and neck tumors increased from 14.7% between 1985 and 1989 to 15.4% between 1990 and 1994 (
12). This increase has been postulated to be attributable to an increase in immunodeficiency secondary to both HIV and patients receiving organ transplants. Interestingly, more recent data from the NCDB suggest both an absolute and proportionate decrease (to 12.4%) in the prevalence of lymphoma from 2000 to 2004, perhaps reflecting the use
of combination antiretroviral therapy for patients with acquired immune deficiency syndrome (AIDS) (
13).
CLINICAL DIAGNOSIS AND IMAGING
The majority of lymphoma cases present with nontender lymphadenopathy of greater than 2 weeks duration, usually in the neck or supraclavicular area (
14). Systemic symptoms including fever greater than 38°C, drenching night sweats, and unintentional weight loss of greater than 10% of body weight over a period of 6 months or less are known collectively as B symptoms. B symptoms are established negative prognostic factors in both HL and NHL and predict worse treatment response and survival. Recently, B symptoms, a marker of systemic inflammation, have been established as an independent predictor of increased toxicity from chemotherapy in NHL patients (
15).
Although HL is primarily a disease confined to lymph nodes, primary extranodal involvement occurs in 25% to 40% of NHL patients at initial diagnosis (
16). Roughly a third of all primary extranodal lymphomas occur in Waldeyer ring, a circle of lymphoid tissue in the pharynx formed by the palatine and pharyngeal tonsils as well as the lymphatic follicles at the base of tongue (
17). Several European studies have shown an even higher incidence of extranodal disease in Waldeyer ring, likely related to the routine biopsy of this area in all patients with NHL (
18,
19). Lymphomas in this region compromise greater than half of all primary extranodal lymphomas of the head and neck (
20). Less commonly, primary lymphoma in the head and neck can manifest in salivary glands, the sinonasal region, the thyroid, and the larynx.
Diagnosis of lymphoma in the head and neck includes a combination of history and physical, including a full head and neck exam. Either mirror exam or flexible laryngoscopy should be performed to visualize Waldeyer ring, the larynx, and hypopharynx. Routine hematologic and biochemical profiles, renal and liver profiles, as well as imaging should be obtained as well. Cardiac assessment including clinical examination, electrocardiography (EKG), and echocardiogram should be performed for all patients greater than 65 years of age and when otherwise indicated.
Serum lactate dehydrogenase (LDH) level should be measured in all patients and is an important predictor of survival, with elevated levels indicating tissue damage, lymphoma relapse, or renewed growth. As a component of the International Prognostic Index (IPI), pretreatment LDH is used to stratify patient populations into appropriate treatment regimens (
21). β-2 microglobulin testing, which has been shown to predict response rate and duration of remission, is also routinely performed in some centers (
22). Bone marrow aspirate and biopsy, typically of the bilateral iliac crests, is also routinely performed to define the extent of disease in initial staging. Marrow involvement is found in 5% to 15% of HL patients at diagnosis and up to 30% of newly diagnosed NHL cases (
23,
24). Cerebrospinal fluid (CSF) evaluation should be performed in patients with paranasal sinus or nasopharyngeal involvement due to disease proximity to the skull base. CSF analysis should also be considered in patients with large cell lymphoma presenting with an elevated LDH and/or involvement of multiple extranodal sites (
25).
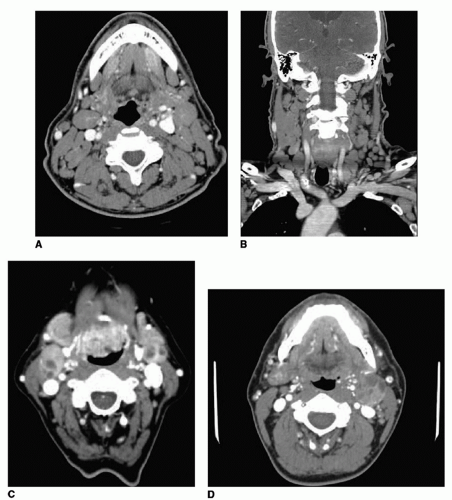
Contrast-enhanced computerized tomography (CT) of the head, neck, chest, abdomen, and pelvis is routinely performed for evaluation of both nodal and nonnodal lymphoma involvement. CT of the head and neck is also useful for the assessment of any bony involvement or destruction of the mandible, maxilla, paranasal sinuses, and skull base. Although it is difficult to distinguish HL and NHL by CT alone, lymphoma is suspected when multiple, nonenhancing, large, homogeneous lymph nodes are present, particularly in unusual nodal chains such as the retropharyngeal, occipital, and parotid nodes (
Fig. 128.2) (
26). Because nodal necrosis is present in the majority of lymph nodes involved with squamous cell carcinoma (SCC) larger than 3 cm, lymphoma is implicated with the presence of large nonnecrotic nodes (
27). Pretreatment nodal necrosis, when seen, is usually found in high-grade lymphomas (
28).
Fluorine-18-fluorodeoxyglucose positron emission tomography-computed tomography (18F-FDG-PET-CT) superimposes anatomic detail from CT images with functional imaging obtained by PET. 18F-FDG-PET-CT is a good choice as the initial imaging study in patients with FDG avid lymphomas such as HL, B-cell lymphoma, or follicular lymphoma. A pretreatment 18F-FDG-PET-CT is used in most centers for initial staging and allows for subsequent monitoring of response to treatment and assessment of recurrent or residual disease. Because it evaluates metabolic activity, 18F-FDG-PET-CT can also help differentiate malignant and nonmalignant lymph nodes in small lymph nodes that are negative by CT size criteria. Improved accuracy in staging with 18F-FDG-PET-CT may help avoid overtreatment and its associated toxicities.
Recent studies have shown upstaging of disease in up to 20% of cases using PET-CT with improved detection of
occult splenic involvement and exclusion of bone marrow involvement in aggressive B-cell NHL (
29). A meta-analysis of 20 studies including seven prospective trials on the effectiveness of PET in lymphoma staging showed an overall change-in-management rate of 30% based on imaging findings (
30).
18F-FDG-PET-CT is less useful in low-grade NHL because of low metabolic uptake in malignant nodes (
31).
STAGING
First proposed in 1971 for HL and later adapted for NHL, the Ann Arbor staging system is the most widely used criterion for determining prognosis and treatment (
Table 128.1) (
47). This system is based on the region and number of affected lymph nodes as well as the presence of extranodal sites and constitutional symptoms. The Ann Arbor staging system that was originally developed for HL is currently used to stage both HL and NHL. In 1989, the Ann Arbor system was refined with the Cotswalds modification, which takes into account the importance of bulky disease as a negative prognostic factor (
48).
The Ann Arbor system does not, however, take into account the grade and biologic behavior of a given lymphoma and has been shown to be inadequate as a sole predictor of overall survival for patients with aggressive NHL (
49). In 1993, the IPI was proposed. Based on a retrospective series of over 2,000 patients in an international multi-institutional study, this model uses age, Ann Arbor tumor stage, serum LDH, performance status, and number of extranodal disease sites to stratify patients into four risk groups (
50). Because younger patients may tolerate more aggressive therapy and thus have different outcomes, an age-adjusted index was proposed in the same study for patients younger than 60. This simplified criteria use only stage, LDH, and performance status to predict outcomes. Similar to the IPI, the Follicular Lymphoma International Prognostic Index (FLIPI) was designed as a prognostic model for patients with indolent lymphoma (
51). Factors in this index include age, stage, number of involved lymph node areas, serum hemoglobin level, and serum LDH.
These systems alone are not, however, sufficient for initiating treatment, as outcome is highly variable and dependent on tumor histology and morphology. In 1982, the Working Formulation, a now-obsolete classification of NHL tumors, subdivided lymphomas by morphology alone (
52). The REAL and later the WHO classification groups differentiated NHLs by cell lineage and unique phenotypic, molecular, and cytogenetic characteristics. The fourth edition of the WHO classification, which is the most recent update, was introduced in 2008 and classifies NHL as indolent, aggressive, and highly aggressive tumors (
9). However, it should be kept in mind that the WHO classification system is not a staging system. The Ann Arbor staging system, despite its shortcomings, remains the best mean of staging lymphomas and has been adopted by the
American Joint Committee on Cancer (AJCC) as well as Union for International Cancer Control (UICC) as the official system for classifying the extent of anatomic involvement and for staging of both HL and NHL.