Lower Eyelid Blepharoplasty
Stephen W. Perkins
Jess Prischmann
Lower eyelid blepharoplasty is one of the most common and technically challenging procedures in facial plastic surgery. Unlike upper eyelid blepharoplasty, surgery on the lower eyelid has a lower threshold for error and a higher potential for complications. Most blepharoplasty surgeons will encounter unexpected postoperative outcomes. Because of this, an intimate understanding of anatomy, methodical evaluation of patients, obsessional intraoperative treatment of tissue planes, and prompt recognition of complications are required for success in this detail-driven and rewarding procedure.
LOWER EYELID ANATOMY
The upper and lower eyelids contain analogous structures. Knowledge of upper eyelid anatomy begets understanding of its lower counterpart.
The eyelids are divided into lamellae. The anterior lamella is composed of skin and the orbicularis oculi muscle. While the skin of the eyelid is the thinnest in the body, the thickness of the orbicularis is variable. The posterior lamella is composed of the tarsal plates, capsulopalpebral fascia, and palpebral conjunctiva. The capsulopalpebral fascia is part of the lower eyelid retractor and is an extension of the inferior rectus muscle. The middle lamella refers to the orbital septum (Fig. 187.1).
The lower eyelid is critical in creating a natural “almond” shape to the palpebral fissure. It is most commonly angled slightly upward, with the lateral canthus being 2 mm higher than the medial canthus. Variations exist, as the palpebral fissure can be angled downward or neutral. The lower eyelid margin should rest at the inferior limbus of the iris. Maintaining these topographical relationships is important in blepharoplasty.
The lower eyelid has three described fat pads: medial, central, and lateral. The inferior oblique muscle separates the medial and central fat pads. The central and lateral fat pads are separated by the arcuate expansion of Lockwood ligament. The medial fat pad is most commonly transposed to efface the “tear trough deformity” (as described below).
The inferior oblique muscle can be vulnerable to injury during lower lid blepharoplasty. It originates from the orbital floor lateral to the nasolacrimal canal. It takes a posterolateral course, passes inferior to the inferior rectus muscle, and inserts on the globe. Injury to the inferior oblique can result in a range of disability, from transient diplopia to permanent strabismus. This complication can largely be avoided by only transecting fat that protrudes anterior to the orbital septum (1).
The blood supply to the lower eyelid is through rich anastomoses between the internal and external carotid artery systems. The major arteries include the dorsal nasal, angular, infraorbital, transverse facial, zygomaticofacial, and medial palpebral. From a surgical perspective, the plane between the orbital septum and orbicularis is relatively avascular. However, meticulous hemostasis is required when dissection proceeds anteroinferiorly (as performed in fat transposition) or posteriorly (as performed during routine access to fat pockets).
The sensation to the lower eyelid is from branches of the infraorbital nerve, a terminal branch of the maxillary division of the trigeminal nerve. The motor innervation is through the oculomotor and facial nerves.
IMPORTANT TERMINOLOGY
Knowledge of a few basic terms is required for effective communication with regard to lower eyelid blepharoplasty.
Orbital fat pseudoherniation or palpebral bags: Bulging of orbital fat that is seen in conjunction with a weakened orbital septum and/or relaxation of Lockwood ligament. Visible pseudoherniation of orbital fat disrupts the normally smooth transition between the eyelid and cheek subunits and creates an “aged” or “tired” appearance.
It is considered to be the most common indication for lower eyelid blepharoplasty (Fig. 187.2).
It is considered to be the most common indication for lower eyelid blepharoplasty (Fig. 187.2).
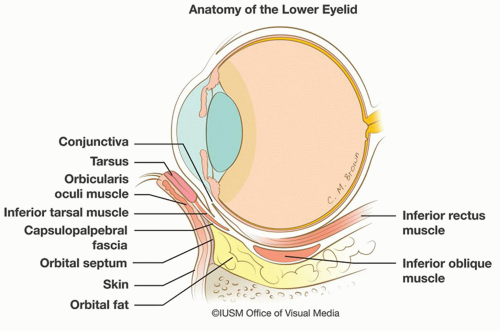 Figure 187.1 Anatomy of the lower eyelid. |
Dermatochalasis: Excess skin of the eyelid (Fig. 187.3). Dermatochalasis should not be confused with “blepharochalasis,” which is a rare inflammatory disorder of the eyelids characterized by recurrent edema.
Orbicularis hypertrophy: Increased thickness of the preseptal or preorbital portions of the orbicularis oculi muscle (Fig. 187.4). This sign is often mistaken for orbital fat pseudoherniation.
Scleral show: The measurement of white (sclera) show between the inferior limbus of the iris and the margin of the lower eyelid when the head is in the Frankfort horizontal plane (Fig. 187.5).
Negative vector: Seen when the anteriormost point of the cornea projects beyond the inferior orbital rim. Most commonly recognized on profile view (Fig. 187.6).
Lower eyelid laxity: Horizontal excess of the lower eyelid that occurs as the result of aging. Clinically determined by the snap and/or distraction tests (Fig. 187.7).
 Figure 187.2 Orbital fat pseudoherniation, considered the most common indication for lower eyelid blepharoplasty. |
Ectropion: Outward turning of the eyelid margin away from the globe (Fig. 187.8).
Entropion: Inward turning of the eyelid margin toward the globe.
Tear trough deformity: The soft tissue surface depression seen along the medial inferior orbital rim, often accentuated by orbital fat pseudoherniation (2) (Fig. 187.9).
Double convexity deformity: The contour deformity that results from descent of the suborbicularis oculi fat pat below the arcus marginalis and weakening/bowing of the orbital septum above the arcus. Most commonly seen on three-quarters or profile view. This deformity is considered an indication for fat repositioning in lower eyelid blepharoplasty or midface lift (3) (Fig. 187.10).
Festoons: Redundant folds of lax skin and orbicularis muscle that hang in a hammock-like fashion from canthus to canthus (4) (Fig. 187.11).
Malar mounds or bags: The soft tissue convexity seen between the orbicularis retaining ligament and the zygomaticocutaneous ligament. As aging occurs, the “fixed”
nature of the ligaments causes a visible disruption in the contour between the eyelid and cheek (Fig. 187.12).
nature of the ligaments causes a visible disruption in the contour between the eyelid and cheek (Fig. 187.12).
 Figure 187.3 Lower eyelid dermatochalasis. |
 Figure 187.4 Orbicularis hypertrophy of the lower eyelid. Note the thickness of the orbicularis without pseudoherniation of orbital fat. |
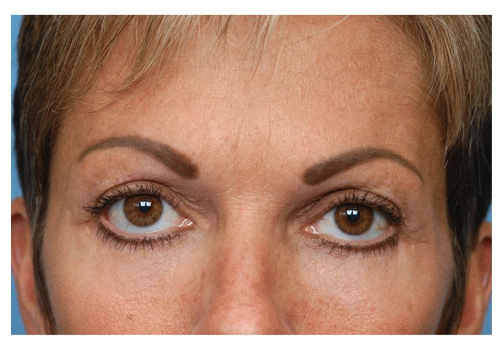 Figure 187.5 Scleral show. Note that the lid margin rests below the lower limbus of the iris. |
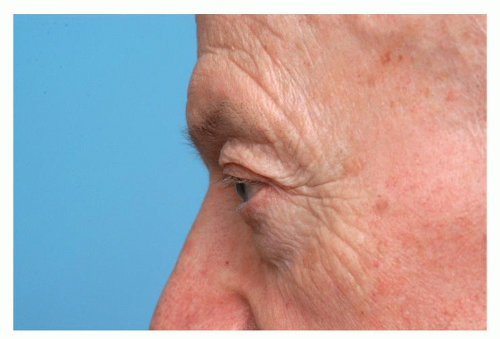 Figure 187.6 Negative vector orbit. Note that the anteriormost projecting point of the cornea projects beyond the inferior orbital rim. |
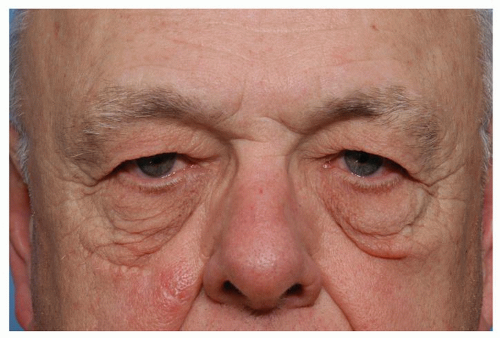 Figure 187.7 Lower eyelid laxity. Blepharoplasty in patients with this finding necessitates lid-supporting adjunctive procedures. |
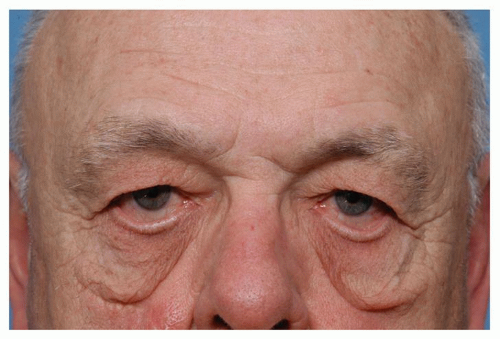 Figure 187.8 Ectropion. Note the outward turning of the lid margin away from the globe. Blepharoplasty in patients with this finding necessitates lid-supporting adjunctive procedures. |
 Figure 187.9 “Tear trough” deformity. |
 Figure 187.10 “Double convexity” deformity. Note the contour deformity that results from bowing of the orbital septum above the arcus marginalis and descent of the suborbicularis oculi fat pad below the arcus. |
PATIENT SELECTION AND EXAMINATION
The ideal lower eyelid blepharoplasty patient is healthy, has reasonable expectations, and presents with findings easily correctable with a surgical procedure. In order to determine appropriate candidacy, the surgeon must be prepared to look for and elicit for pertinent signs and symptoms.
An evaluation should always begin with an assessment of the patient’s motives and expectations. Lower lid blepharoplasty can correct orbital fat pseudoherniation, excess skin and muscle, mild festooning, and tear trough deformities. However, if the patient’s main concerns include abnormal skin pigmentation, fine rhytids, or large malar bags, the surgeon must explain that a blepharoplasty is not the appropriate procedure (5) (Fig. 187.13A and B).
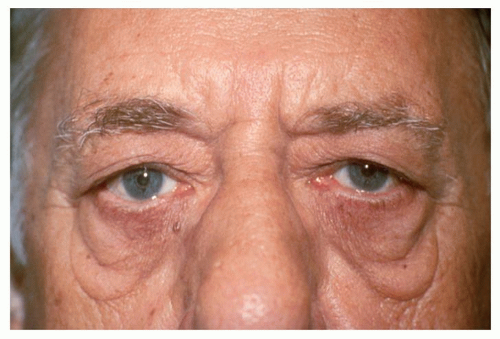 Figure 187.11 Lower eyelid festoons. |
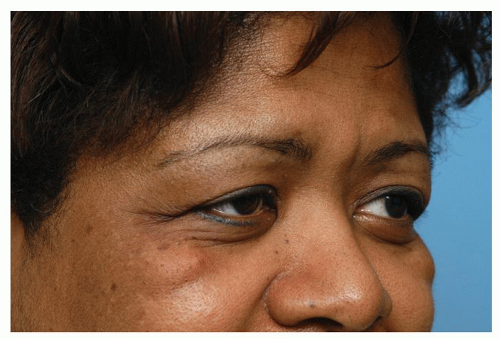 Figure 187.12 Malar mounds. This finding is not easily correctable with standard blepharoplasty approaches. |
When discussing medical history, the surgeon should ask about thyroid eye disease, poorly controlled hypertension, anticoagulant use, blepharitis, facial nerve dysfunction, history of keloid scars or herpes zoster ophthalmicus, and visual field problems (5). Particular attention should be paid to a history of dry eye symptoms or regular use of lubricating drops. The surgeon should inquire about dry eye symptoms in several ways, as some patients may only report “allergic”-type symptoms or watering without emotional stimulation (Fig. 187.14). All patients, and particularly those with symptoms, should be informed that blepharoplasty can cause or exacerbate dry eye symptoms. The surgeon should be aware that a subclinical dry eye condition can worsen to a keratoconjunctivitis sicca with the mechanical alteration that occurs following cosmetic eyelid surgery (6).
A thorough physical examination is critical to selecting the correct procedure and avoiding postoperative complications. The surgeon should look for the following: orbital fat pseudoherniation, orbicularis hypertrophy, dermatochalasis, tear trough deformity, lid laxity, scleral show, negative vector, festooning, malar bags, midface ptosis, and fine rhytids.
Orbital fat pseudoherniation and dermatochalasis are the most common reasons patients seek lower eyelid blepharoplasty. In most cases, fat pseudoherniation is obvious on inspection. This finding can be confirmed by gentle pressure on the globe and examining the patient in upward gaze. Orbicularis hypertrophy can be differentiated from fat pseudoherniation by having the patient smile or squint. While fat pseudoherniation can be treated with either a transconjunctival or transcutaneous approach, skin or muscle excess can only be treated with an incision through the anterior lamella.
The contour of the lower lid should be closely examined. The surgeon should assess for a “tear trough deformity.” If a surface depression is noted along the inferomedial aspect of the orbital rim, a fat transposition to efface the “tear trough” should be performed (see procedure section).
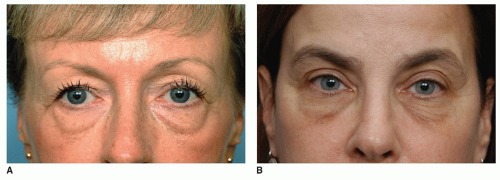 Figure 187.13 A: Excellent candidate for blepharoplasty. This patient has obvious pseudoherniation of orbital fat, tear trough deformity, and some excess skin and muscle. B: Poor candidate for blepharoplasty. This patient has hyperpigmentation and fine rhytids of the lower eyelid. |
Examination for lid laxity deserves special attention. Failure to note this common sign is a missed opportunity for the surgeon and can result in patient dissatisfaction and an increased risk of postoperative complications. Lower eyelid laxity is evaluated by two common clinical tests: the snap test and distraction test. The snap test assesses canthal stability and orbicularis and tarsal strength (7). The test is performed by gently pulling the lower lid toward the orbital rim and releasing. Obvious scleral show or slow return to the resting position (greater than 1 second) indicates poor lid support. The distraction test is performed by grasping the lower lid and pulling it away from the globe. Distraction of the eyelid greater than 10 mm indicates poor lid support. If the distraction or snap tests are positive, failure to adequately support the lid can lead to ectropion, epiphora, or exposure keratitis (7) (Fig. 187.15A and B).
The position of globe relative to the eyelid and maxilla should also be examined. Assessing for scleral show and negative vector can change the surgical plan and prevent postoperative lid malposition. In a normal-vector orbit, the cornea rests in a vertical plane with the inferior orbital rim. When a negative vector is present, the cornea lies in plane anterior to the inferior orbital rim. In patients with negative vector orbits, transcutaneous approaches with shortening of the anterior lamella can result in significant postoperative lid malposition. If scleral show or negative vector is noted preoperatively, the surgeon can plan procedures to support the lower lid, such as intraoperative canthopexy (see below) or postoperative lid taping. Patients with negative vector orbits should also have conservative fat removal, as they are more prone to developing a “hollowed” appearance.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


