Low Vision: Introduction
In every subspecialty of ophthalmology, the patient with impaired vision represents a challenge in management. Whether reduced vision is temporary or permanent, it is the consequence of an eye disorder and, as such, is the responsibility of the ophthalmologist and optometrist. If the outcome of optimal medical and surgical intervention is diminished functional vision, the patient needs vision rehabilitation (also see Chapter 25). No person with low vision should have to search far and wide for low-vision care. Some level of care should be integrated into every ophthalmic practice, whether it is on-site or referral to a low-vision center.
Low-vision patients typically have impaired visual performance, that is, visual acuity not correctable with conventional glasses or contact lenses. They may have cloudy vision, constricted fields, or large scotomas. There may be additional functional complaints: glare sensitivity, abnormal color perception, or diminished contrast. Some patients have diplopia. A frequent complaint is confusion from overlapping but dissimilar images from each eye.
The term “low vision” covers a wide range. A person in the early stages of an eye disease may have near-normal vision. Others may have moderate to severe loss. All low-vision patients have some degree of useful vision even though the loss may be profound. They should not be considered “blind” unless they no longer have useful visual clues. Performance varies with each individual.
In the United States, over 6 million persons are visually impaired but not classified as legally blind.1 Over 75% of patients seeking treatment are age 65 or older. Age-related macular degeneration accounts for an increasing number of cases. Other common causes of low vision are glaucoma, diabetic retinopathy, cataract, optic atrophy, corneal disease, cerebral damage resulting in hemianopia, degenerative myopia, and retinitis pigmentosa. Approximately 9% of the low-vision population is pediatric, resulting from congenital eye disorders or trauma. (See Chapter 20 for discussion of the worldwide prevalence and causes of visual impairment.)
Effective low-vision intervention starts as soon as the patient experiences difficulty performing ordinary tasks. A treatment plan should consider the level of function, realistic goals for intervention, and the varieties of devices that could be helpful. Patients must face the fact that impaired vision is usually progressive. The sooner they adapt to low-vision devices, the sooner they can adjust to the new techniques of using their vision. Low-vision evaluation should never be delayed unless the person is in an active phase of medical or surgical treatment.
Visual performance can be improved by the use of optical and non-optical devices. The general term for corrective devices is “low-vision aids.” In this chapter, the emphasis will be on assessment techniques, descriptions of useful devices, and a discussion of some of the functional aspects of common eye diseases.
Management of the Patient with Low Vision
Comprehensive management includes (1) history of onset of the eye condition and the effect of the loss of vision on daily life; (2) examination for best corrected acuity, visual fields, contrast sensitivity, color perception (and glare sensitivity if it pertains to the patient’s symptoms); (3) evaluation of near vision and reading skills; (4) selection and prescription (or lending) of aids that accomplish task objectives; (5) instruction in correct use and application of devices; and (6) follow-up to reinforce new patterns.
Specific features of the onset, treatments given, and current medications should be verified. Patients’ responses indicate their understanding of their condition. Unrealistic or unreasonable attitudes need to be documented. Does the person understand the limitations of what can be achieved with low-vision rehabilitation? It is helpful to refer to a list of common daily activities the patient may not be able to perform efficiently (Table 24–1). From this list, it is possible to arrive at realistic treatment objectives for that person.
| Activity | Optical Aids | Non-Optical Aids |
|---|---|---|
| Shopping | Hand magnifier | Lighting, color cues |
| Fixing a snack | Spectacle magnifier | Color cues, consistent storage plan |
| Eating out | Hand magnifier | Flashlight, portable lamp |
| Identifying money | Spectacle, spectacle-mounted or hand magnifier | Arrange wallet in compartments, fold banknotes of different denominations differently |
| Reading print | Spectacle, spectacle-mounted, dome, hand, or stand magnifier Closed-circuit television | Lighting, high-contrast print, large print, reading slit |
| Writing | Hand magnifier | Lighting, bold-tip pen, black ink |
| Dialing a telephone | Telescope Hand magnifier | Large-print dial, hand-printed directory |
| Crossing streets | Telescope | Cane, ask directions |
| Finding taxis and bus signs | Telescope | |
| Reading medication labels | Hand magnifier | Color codes, large print |
| Reading stove dials | Hand magnifier | Color codes |
| Thermostat adjustment | Hand magnifier | Enlarged-print model |
| Using a computer | Intermediate add spectacles | High-contrast color, large-print program |
| Reading signs | Spectacle or spectacle-mounted magnifier Telescope Portable electronic magnifier | Move closer |
| Watching sporting event | Telescope | Sit in front rows |
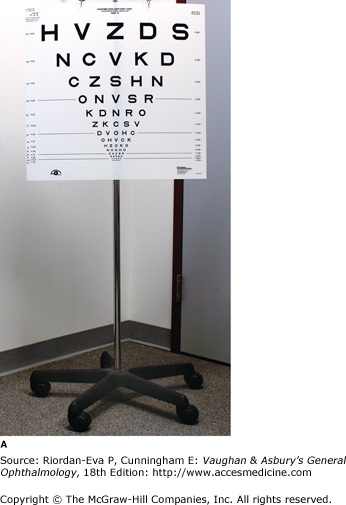
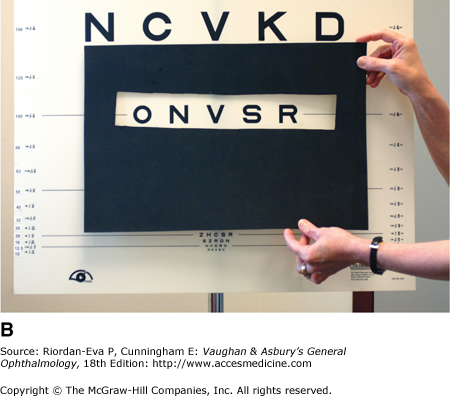
The patient should not have pupillary dilation before a low-vision evaluation. Refractive status should be confirmed to rule out a significant change, particularly after surgical intervention such as cataract or glaucoma surgery. A patient may have become myopic from a nuclear cataract or astigmatic from corneal warping after glaucoma drainage surgery. The most accurate acuity test is the Early Treatment Diabetic Retinopathy Study (ETDRS) chart (Figure 24–1), which has 14 five-letter lines of 0.1 log unit size difference with a LogMAR (logarithm of minimum angle of resolution) scale and a convenient metric or Snellen conversion. Masking of other lines may facilitate letter recognition. An integrated light box standardizes illumination. A 4-meter test distance is used when acuity is 20/20 to 20/200; a 2-meter distance for acuities less than 20/200 but 20/400 or better; and a 1-meter distance for acuities less than 20/400. The ETDRS chart makes obsolete the imprecise expression “finger counting.” Alternatively, a Snellen chart can be used, either at the conventional testing distance of 20 feet (6 m) or less (see Chapter 2).
Projector charts are not recommended for testing subnormal vision because of low contrast and insufficient letter choice at low acuities.
The dominant eye and preferred eye should be noted.
The Amsler grid is the traditional test for evaluating the central field. Although it is relatively insensitive, it can be used to advantage in low vision, particularly to identify the dominant eye. At the test distance of 33 cm, the patient should first look at the chart binocularly. (“Can you see the dot?”) Observe for eye or head turn. If the dot is seen, the patient is using either a viable macula or an eccentric viewing area. An eye turn or head tilt may confirm this. Ask the patient to report distortion or blank areas seen binocularly. Then check the grid monocularly and again ask the patient to report seeing the center fixation dot and any distortion or scotoma. If the grid is presented in this manner, the patient understands what is expected and the test can provide helpful data. For example, if a large scotoma in the dominant eye overrides the better nondominant eye, the patient probably will require occlusion of the dominant eye. If the dominant eye is the better eye, it will override the poorer nondominant eye and the patient can benefit from binocular correction.
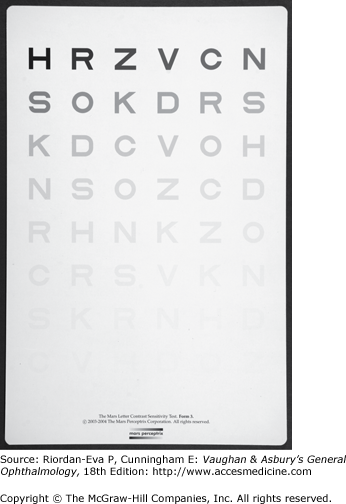
Tests of contrast express the functional level of retinal sensitivity more accurately than any other test, including acuity. Of the available tests for contrast sensitivity, the recently developed Mars test using letters arranged on three 14 × 19 charts in 8 rows of 6 letters each has been evaluated favorably (Figure 24-2).2 The contrast of each letter decreases by a constant factor of 0.04 log unit, which makes it the most sensitive of the clinical contrast tests. The test results identify the level of contrast loss: profound loss, severe loss, moderate loss, and normal adult contrast sensitivity. It is a rapid and accurate method of measuring an important visual function. Contrast sensitivity is a predictor of the retina’s response to magnification. Regardless of acuity, if contrast is subthreshold or in the severe loss category, the patient is less likely to respond to optical magnification.
Simple color identification tests are done if the patient’s complaints include difficulty with color cues.
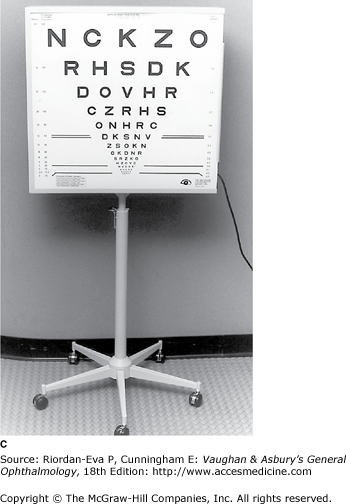
Near vision may be evaluated with a combination of single-letter tests, such as with a reduced version of the ETDRS chart, and graded text, short sentences with simple vocabulary being helpful and non-threatening (Figure 24–3). Single letters and short words are presented first to establish near acuity. Graded text is then presented to establish reading skills with the selected optical devices.
The dioptric range is selected from the outcome of acuity tests, modified by the results of the Amsler grid and contrast sensitivity tests. A rule of thumb for the starting power is to calculate the reciprocal of visual acuity—for example, an acuity of 20/160 suggests a starting lens of 8 diopters (160/20). Keep in mind that visual acuity is not a particularly sensitive measure of function. Scotomas within the reading field and the contrast sensitivity of the paramacular retina have a greater influence on ability to read magnified print through an optical lens.
After the dioptric range has been agreed upon, the three major categories of devices are presented in sequence in the selected power. Lenses in a spectacle mounting are presented and evaluated first, followed by hand-held magnifiers and, third, stand-mounted magnifiers. Telescopes and television or computer-designed devices are increasingly prescribed as the population becomes more sophisticated in the use of advanced technology.
Part of effective management of every low-vision patient is skilled instruction in using a device. Attention should be paid to daily living activities, which can be complemented by low-vision lenses but may also require referral to an agency for the visually impaired.
The patient uses the various devices under the supervision of an instructor until proficiency is achieved. During the instruction time, mechanics of the aids are reviewed, questions are answered, and goals reexamined. The patient is allowed ample time to learn correct techniques in one or more sessions, and possibly a loaner lens for home or job trial. Older patients usually need more adaptation time and reinforcement than younger or congenitally impaired persons.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


