Facial reconstruction is a challenging yet rewarding endeavor. Repair of facial defects requires an appreciation of variations in facial cutaneous tissue and the influence of these differences on use of potential reconstructive methods. Multiple factors help determine the optimal method of repair, including the size of the defect, the depth and location of the defect, and the strength of the underlying facial framework. Maintaining symmetry, contour, and function is essential for a successful facial reconstruction. Finally, of utmost importance is a thorough understanding of all appropriate reconstructive options.
SKIN ANATOMY
Skin variability in color, texture, thickness, and accessory components is demonstrated from one anatomic region to another, and an understanding of these variations is important for optimizing wound healing and soft tissue restoration. Skin consists of an epidermal component with appendages and a dermal component with neurovascular supply.
The epidermis consists of predominantly keratinocytes (80%) but also melanocytes, Langerhans cells, and Merkel cells (Table 173.1). The basal layer, spinous layer, granular layer, and cornified layer make up four distinct histologic layers, with the deepest layer, the basal layer, serving as the germinative layer. Melanocytes are dendritic, pigment-synthesizing cells of neural crest origin with clear cytoplasm, and they are confined to the basal layer. Melanin is produced by melanocytes, which is transported to adjacent basal and spinous layers for engulfment by the keratinocytes. Once engulfed, the melanin is arranged as a cover over the nuclei, serving as a protective barrier against ultraviolet irradiation. Langerhans cells are derived from bone marrow and serve to process and present antigens. These cells are found in the suprabasal epidermal layers, have dendritic processes, and contain Birbeck or Langerhans cell granules (1). Merkel cells are mechanoreceptors of neural crest origin and are primarily involved with touch sensation. Merkel cells are usually found in areas of high tactile sensitivity, where they aggregate to form tactile disks and Merkel cell-neurite complexes (2).
The dermal-epidermal junction is a critical structure that helps prevent dermal-epidermal separation, and alterations in the structure are found in diseases like epidermolysis bullosa (3). Keratin filaments within the basal keratinocyte condense and attach to an electron-dense plaque at the inferior portion of the cell membrane known as the hemidesmosome. Anchoring filaments in the lamina lucida connect hemidesmosomes to the lamina densa, which in turn is connected to the anchoring plaques in the dermis by anchoring fibrils.
Epidermal appendages include hair follicles, sebaceous glands, and eccrine and apocrine sweat glands. Pilosebaceous units contain hair follicles, sebaceous glands, arrector pili muscles, and sensory end organs. The pilosebaceous unit has motor and sensory functions, while also producing hair and sebum. On the nasal tip, the sebaceous component of the pilosebaceous unit is most prominent, while on hairbearing surfaces, the follicular component predominates. Complete units are absent on the soils, palms, and mucous membranes. Healing of partial-thickness wounds by secondary intention is facilitated by pilosebaceous units, since reepithelialization occurs in part from the epithelial cells that line the follicular unit. Sebaceous glands connect to the hair follicle by a squamous epithelial duct, allowing the glands to secrete sebum through the duct, along the follicle, and onto the surface of the skin. Perhaps providing a protective function, sebum acts as an emollient to the hair and skin. Eccrine sweat glands contain a secretory gland in the deep reticular dermis and a coiled intraepithelial duct that opens to the skin surface. These glands are controlled by the cholinergic system, and the duct can modify the composition of sweat secretion. Apocrine sweat glands receive adrenergic innervation and are generally found in the eyelids (Moll glands), external auditory canal (ceruminous glands), axillae, areolae, and perineum (1).
TABLE 173.1 CONTENTS OF EPIDERMIS
Keratinocytes
Melanocytes
Langerhans cells
Merkel cells
The majority of skin consists of the dermis, which contains neural and vascular networks, epidermal appendages, fibroblasts, macrophages, mast cells, and other cells (Table 173.2). The extracellular matrix consists of collagen, elastin, and amorphous substance known as the “ground substance.” Skin pliability, tensile strength, and elasticity are properties attributed to the dermal component, and the dermis is divided into the papillary (superficial) and reticular (deeper) layers. Fibroblasts produce collagen, mostly type I collagen, which is responsible for the tensile strength and elasticity of skin. Type III collagen is much less common, and is found in the papillary dermis. Matrix metalloproteinases degrade collagen, allowing new collagen to replace old fibers; however, induction of collagenases by ultraviolet radiation can lead to disorganization that is clinically manifested as skin wrinkling and photoaging. Fibroblasts also produce elastin, which is degraded by elastases, allowing a continuous regenerative process. Elastin fibers are perpendicular to skin surface in the papillary dermis and parallel in the reticular dermis. Ground substance is generated by fibroblasts and consists primarily of proteoglycans, glycosaminoglycans, and filamentous glycoproteins. Ground substance is thought to help with distribution of pressure forces (1).
An abundant vascular supply is present in the skin, facilitating nutritional support and thermo regulation for the body. At the junction of the dermis and subcutaneous fat is the deep vascular plexus, whose arterioles supply the epidermal appendages and superficial vascular plexus. The superficial plexus lies in the reticular dermis and is connected to a vascular loop system in the papillary dermis, which provides nutrients to epidermal cells via diffusion.
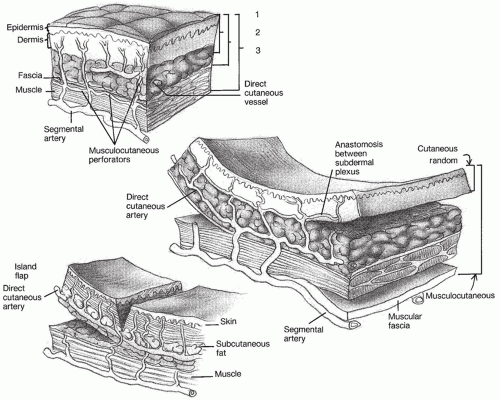
Blood vessels travel one of two ways to reach the cutaneous vascular plexus. Septocutaneous arteries travel through fascial septa, between muscular segments, parallel to the cutaneous surface. These arteries supply large areas of skin and have a pair of veins. Musculocutaneous arteries pass through muscle and are more common; however, these arteries typically supply smaller areas of cutaneous surface (Fig. 173.1) (4).
Sensory innervation includes both sensory and sympathetic nerves. Efferent nerves innervate blood vessels in the skin, and sensory nerves include dermal neural receptors known as Meissner (fine touch) and pacinian (deep pressure, vibration) corpuscles. Sensory nerves are distributed in a segmental fashion known as dermatomes.
SKIN BIOMECHANICAL PROPERTIES
The unique mechanical properties of skin influence cutaneous vascularity with tissue movement and ultimately flap survival. Skin is described as having a nonlinear stress- strain relationship, where stress represents force per unit of original cross-section and strain represents change in length divided by original length (5, 6). With initial deformation, randomly oriented collagen and elastic fibers are stretched in the direction of the force, allowing extension with little force. With continued deformation, additional collagen fibers are recruited to load carrying capacity, but resistance transitions to eventual inability of further deformation with further force. At this point, no further collagen and elastic fibers can be oriented in the direction of the force and the structural integrity is protected against additional forces (7).
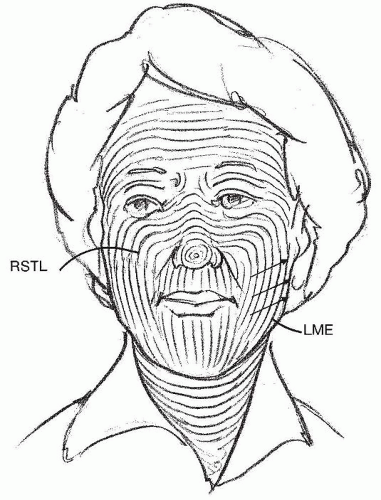
Skin is also characterized as being directional or anisotropic. The degree of skin tension is greatest parallel to the relaxed skin tension lines (RSTLs), a phenomenon that reflects interactions between collagen and elastic fibers at the cellular level. Lines of maximal extensibility (LME) run perpendicular to the RSTLs and represent lines of closure with the least tension (Fig. 173.2) (7, 8, 9).
Finally, skin is described as an elastic substance with lesser stress or force, but as a viscoelastic substance with higher stress loads. Higher stress loads cause skin to experience creep, which describes the increase in length with constant stress. Histologically, the increased length experienced is related to the displacement of interstitial fluid. Stress relaxation, although related to creep, defines the decrease in tension in skin overtime with constant tension (7). Larrabee showed that the effect of tension on flap survival is affected by flap length. Flaps with 3 cm base and 6 cm length showed necrosis, while flaps with the same base and 1.5 cm length all survived regardless of tension. Flaps with intermediate lengths were tension sensitive, with tension greater than 250 g tending to cause necrosis (10). Undermining is thought to reduce wound tension by releasing vertical attachments between the dermis and subcutaneous tissues, allowing less restricted movement.
Figure 173.1 Representation of cutaneous vascular supply. Numbered parentheses delineate vascular supply for various types of flaps: 1, random-pattern flaps; 2, axial-pattern flaps; 3, myocutaneous flaps.
SKIN PHYSIOLOGY
The vascular network within the skin facilitates regulation of body temperature and transfer of nutrients and other blood products, and the amount of blood flow is directly related to arteriolar pressure and flow (11). The precapillary sphincter controls the amount of nutritive blood flow to the skin (12), and this sphincter dilates with local hypoxemia (13). Preshunt sphincters, located deeper in the subcutaneous tissue, are regulated by the sympathetic nervous system, causing changes in blood flow that affects body temperature and systemic blood pressure (14). Vasodilatation can also occur with excessive body temperature, through local release of acetylcholine by sympathetic nerve fibers (4).
Revascularization is a complex process that is initiated after cutaneous injury or tissue transfer. Angiogenic stimuli lead to vasodilatation with increased vessel permeability. This is followed by dissolution of the basement membrane by proteases, allowing endothelial cells to migrate from the vascular wall toward the angiogenic stimulus. Nearby capillary sprouts anastomose with each other, forming loops. The blood vessels eventually differentiate to lay down basement membrane with type IV collagen, laminin, and proteoglycans. Some capillaries join preexisting vessels (inosculation), while others directly grow into the flap (neovascularization). Growth rate is about 0.2 mm/day, and regression of capillary loops occurs when the stimulus is discontinued after adequate vascular supply to the flap has been established (4). Revascularization adequate for detachment of a flap pedicle can be as early as 7 days (15), although waiting about 3 weeks is usually recommended.
Venous outflow is important, and venous occlusion can be more detrimental to tissue survival than adequate arterial supply. Venous outflow is generally through the subdermal plexus or with venous channels that accompany arteries within the flap. Cutaneous lymphatic drainage is also interrupted with tissue elevation, and increased interstitial fluid pressure can affect capillary perfusion. Severing of sympathetic nerves leads to vasoconstriction (16) through the release of norepinephrine and oxygen-free radicals (17), but the depletion of neurotransmitters within 24 to 48 hours allows improvement in blood flow (18).
Figure 173.2 Relaxed skin tension lines (RSTLs) of the face. Notice that the lines of maximal extensibility (LME) run perpendicular to the RSTLs. Placing incisions along the RSTLs will decrease wound closure tension and optimize wound healing.
Delay of cutaneous flaps is thought to improve survival of the flap at the time of eventual transfer. Some theories used to explain the benefits of delay include improved blood supply after recovery from a hyperadrenergic state that is induced by sympathetic denervation (16, 19) and permanent and irreversible dilation of the “choke” vessel through hyperplasia and hypertrophy (20). Both tobacco smoking and radiation have been shown to have a deleterious effect on flap survival, and delay of regional flaps is strongly considered in these patients (4).
DEFECT ANALYSIS AND PREPARATION
Analysis of a facial defect includes determining the depth of the wound, the color and texture of the missing skin, and the extent of involved aesthetic units and adjacent facial regions. In addition, the defect is inspected for any missing soft tissue, structural support, or lining. The thickness, texture, and mobility of remaining facial skin are assessed carefully; furthermore, any medical, social, and psychological issues pertaining to the patient should be considered. Finally, paramount to a successful reconstruction is appropriate assessment and treatment of any existing or potential functional compromise (i.e., nasal obstruction, eyelid malposition, oral incompetence) (Table 173.3).
TABLE 173.3 KEYPOINTS—FACIAL DEFECT ANALYSIS
Depth, size, and location of defect
Color, thickness, laxity of adjacent skin
Aesthetic units and landmarks
Nearby structures that cannot be distorted
Existing or potential functional compromise
Facial defects occasionally involve multiple areas of the face. When planning reconstructive options, it is helpful to demarcate the division between the primary and surrounding facial regions such that defects involving multiple facial regions are repaired with separate methods addressing each region. Adhering to this principle places eventual scars along boundary lines that separate each aesthetic region, which helps preserve the natural contours of the face.
Within each region, individual aesthetic units should be identified. Aesthetic units are based on variations in skin thickness and texture, as well as variations in contour created by the underlying facial framework (Fig. 173.3). Optimal repair of a facial defect may require repositioning of skin and soft tissue within an involved aesthetic unit, thereby allowing eventual scars to lie within zones of transitions between adjacent units. In addition, small defects may be enlarged to facilitate repair of an entire aesthetic unit by a single repair method.
Figure 173.3 Nasal aesthetic subunits.
TABLE 173.4 LADDER OF FACIAL CUTANEOUS RECONSTRUCTIVE OPTIONS
Healing by secondary intention
Primary wound closure
Skin or composite grafts
Local cutaneous flaps
Regional cutaneous flaps
Distant tissue transfer
Establishing uniform depth, while maintaining symmetry with contralateral facial structures, is equally important. Beveled tissue at the periphery of the Mohs defect is removed if flaps are planned, in order to optimize eversion of skin edges at closure. In addition, cutaneous edges of the flap and the recipient tissue are adjusted appropriately to establish uniform thickness at the line of closure. Whenever possible, the primary defect should be deepened to establish uniformity rather than thinning the flap. One exception to removing beveled edges is when skin grafts are performed. In this circumstance, beveled edges are freshened, but maintained, to provide a gradual contour transition between recipient tissue and the skin graft. Additional techniques helpful in optimizing repair include angulation of curvilinear defects, since round defects are more likely to undergo concentric scar contraction and result in trapdoor deformity. Modifying the periphery of the defect by creating more acute angles often reduces the risk of this deformity.
Facial defects are repaired using a number of options, including healing by secondary intention, primary closure, local and regional flaps, skin grafts, composite grafts, and free tissue transfer (Table 173.4). Occasionally, cartilage grafts or subcutaneous augmentation flaps are also necessary to establish appropriate support as well as contour match with the tissue surrounding the defect. Selection of the optimal reconstructive method is influenced by the size, depth, and location of the facial defect (Table 173.5).
TABLE 173.5 COMPARISON OF RECONSTRUCTIVE OPTIONS
Option
Advantages
Disadvantages
Healing by secondary intention
No further surgery required
Extended wound care. May result in depressed, hypopigmented scar. Contracture may distort adjacent structures.
Primary closure
Technically quick and straightforward
May require excision of additional normal skin if rounded defect
Usually good aesthetic outcome
Use usually limited to defects that lie along RSTLs
Cutaneous graft
Technically quick and straightforward
Donor site required
Potentially poor match in cutaneous color, texture, and contour
Longer wound care. Not always complete survival.
Local cutaneous flap
Easy wound care
May be technically challenging
Short healing period
Creates additional scars
Usually complete survival
Secondary defect may cause distortion.
Excellent color and contour match
Increased risk of bruising, swelling, trapdoor deformity
Potential for greater reconstructive challenge with failure
PATIENT PREPARATION—MEDICAL COMORBIDITIES
Systemic diseases such as diabetes, malnutrition, arteriosclerosis, hypertension, and collagen vascular disease can compromise flap vascularity and lead to necrosis and impaired wound healing. Consulting with the patient’s personal physician is important to ascertain whether the patient’s medical condition is optimized during the perioperative period.
Patients with a history of irradiation have subcutaneous scar tissue and decreased vascularity of the skin in the irradiated area. Cutaneous flaps from adjacent nonirradiated tissue are preferred, but even then, healing may be compromised leading to poor outcome. When interpolated flaps are transferred to an irradiated area, detachment of the flaps is best delayed until revascularization of the flap is certain. For suitable candidates, consideration is given to hyperbaric oxygen treatment to optimize tissue oxygenation levels prior to reconstruction.
Patients are questioned preoperatively concerning their use of tobacco and alcohol. Heavy alcohol consumption will dilate blood vessels, predisposing to hematoma formation. Avoidance of alcohol during the perioperative period is recommended. Ideally, tobacco and nicotine products should be avoided, at least 8 weeks before and after surgery. Even smoking cessation for 2 days before surgery and 7 days after surgery has been shown to have beneficial effects on flap survival. Smokers develop skin necrosis three times more frequently than nonsmokers, and the extent and depth of skin slough are more severe (21). Nicotine causes systemic vasoconstriction through activation of the adrenergic nervous system, which may lower tissue oxygenation pressure by greater than 50%. This occurs within 10 minutes of smoking a cigarette and lasts approximately 50 minutes. Smoking also produces carbon monoxide, which has a higher affinity for hemoglobin than oxygen, thereby producing high levels of carboxyhemoglobin (22, 23, 24, 25, 26). When possible, consideration is given to delaying surgical procedures until smoking cessation can be assured.
HEALING BY SECONDARY INTENTION
Small superficial cutaneous defects involving concave facial surfaces may granulate and epithelialize with an acceptable aesthetic result. Ideal locations for healing by secondary intention include the temple and medial canthus. It is imperative to keep wounds moist during the healing phase. Wounds are cleaned twice daily, removing fibrinous debris during each cleaning. Wounds are then covered with a topical water-based ointment containing mupirocin and nonadherent gauze for the initial 2 weeks, followed by a topical petroleum-based ointment and nonadherent gauze until complete reepithelialization occurs. For patients with larger defects or concerns for slower wound healing, wet-to-dry dressings are employed daily. These patients are instructed to place a moist, but not dripping wet, gauze to the wound in the evening, followed by removal in the morning. The morning wound care is as previously described, with topical ointment application and nonadherent gauze. Patients are counseled that wounds often take 4 to 6 weeks to heal, and massage may be indicated to address any contour irregularities. Patients may be offered resurfacing procedures if surface irregularities are persistent.
PRIMARY CLOSURE
Adjacent facial tissue provides the ideal color, thickness, and texture for repair of most facial defects. Unfortunately, scars associated with primary closure or local flaps do not always fall along borders between aesthetic units; nonetheless, the benefits gained in establishing appropriate contour and skin color may outweigh this potential disadvantage. In general, oval and linear defects along RSTLs in a patient with redundant skin are ideal defects for primary closure; in addition, an M-plasty modification can be performed to shorten the length of the anticipated scar (Fig. 173.4). Modification of underlying facial tissue or framework may facilitate wound closure (i.e., dorsal nasal framework modification), and suspension sutures may be indicated to prevent distortion of mobile structures (i.e., canthal, nasal valve, and alar suspension sutures).
Wide undermining of the skin adjacent to the defect is performed in subcutaneous plane for most facial defects; however, with nasal defects, the dissection is usually performed in a submuscular plane. Dissection in an appropriate plane minimizes bleeding and postoperative bruising, and wide undermining helps avoid trapdoor deformity. The effect of primary closure on surrounding structures such as the nasal tip, alar margin, eyelid, canthus, oral commissure, and hairline should be evaluated. The method of repair should be reconsidered if there is significant distortion that is not expected to resolve with time and postoperative massage.
Figure 173.4 Comparison of the closure of a fusiform excision and an M-plasty excision. The straight portion of the M-plasty closure is significantly shorter than the fusiform closure.
FACIAL CUTANEOUS FLAPS
When primary wound closure is not possible, local flaps from adjacent facial cutaneous tissue may be used to repair defects. Repair with local flaps may be limited by the laxity of the donor skin, and thorough analysis of blood supply, wound closure tension (Table 173.6), and strength of the underlying facial framework should be performed prior to performing a cutaneous flap. Cartilage grafting or suspension sutures may be necessary to prevent distortion of mobile or weaker structures. Standing cutaneous deformities should be anticipated, and incisions should be placed along aesthetic borders or RSTLs when possible. Occasionally, flaps are combined with skin grafting for cutaneous restoration.
Wound created when skin flap is transferred to the primary defect—goal is to place secondary defect in area of greatest tissue laxity.
Primary tissue movement
Movement of flap to defect
Secondary tissue movement
Displacement of skin surrounding defect toward center of wound usually secondary to wound closure tension and movement of tissue to close the donor site
TABLE 173.7 TYPES OF FLAP CLASSIFICATION
Location: local, regional, or distant
Vascular supply: axial or random
Flap design and method of tissue movement
Flap Classification and Description
Cutaneous flaps are generally described as having skin and subcutaneous tissue with direct vascular supply and are usually transferred to an immediately adjacent or nearby location. Flaps can be classified based on (a) location, (b) vascular supply, and/or (c) flap design and method of tissue movement (Table 173.7).
Flaps may be classified based on location of flap relative to the defect. Local cutaneous flaps involve use of tissue immediately adjacent to or near the defect. Regional flap involves use of tissue from outside of the face, scalp, or neck, where arterial pedicle is sufficient to reach the facial defect (pectoralis muscle flap). Distant flaps involve harvesting of tissue from a distant location, requiring microvascular anastomosis of vessels (free flap tissue transfer).
Flaps may also be classified based on vascular supply, being described as having random or axial vascular supply (Tables 173.8 and 173.9). Random cutaneous flaps are supplied by musculocutaneous arteries near the flap base, and blood travels to the tip of the flap via the interconnecting subdermal plexus. Survival of random cutaneous flaps depends on the physical properties of the supplying vessels and the perfusion pressure (27). Flap necrosis occurs when perfusion pressure drops below the critical closing pressure of the arterioles in the subdermal plexus and there is not improved survival with a wider flap base if the arteriolar pressure remains the same (28). Axial cutaneous flaps have a greater likelihood of survival compared to random cutaneous flaps, with the survival advantage largely related to the incorporation of a septocutaneous artery within the longitudinal axis. Survival is related to the length of the included artery, and vascular supply to the portion of skin beyond the direct arterial supply is based on the subdermal plexus, similar to a random cutaneous flap.
TABLE 173.8 AXIAL FLAPS WITH NAMED BLOOD SUPPLY
Paramedian forehead flap
Supratrochlear artery
Lip crossover flap (Abbe or Estlander flap)
Orbicularis oris artery
Temporoparietal flap
Superficial temporal artery
TABLE 173.9 RANDOM CUTANEOUS FLAPS
Rotation flaps
Transposition flaps
Advancement flaps
Postauricular interpolation flap
Flaps may be described based on the method of tissue movement and include three general types: pivotal, advancement, and hinge flaps (Table 173.10). Each of these methods will be described in more detail with the following discussion.
Pivotal Flaps
Pivotal flaps move toward the center of the wound by pivoting around a fixed point at the base of the flap pedicle, and examples include rotation, transposition, and interpolation. In general, the greater the pivot of the flap, the shorter the effective length of the flap. The effective length is reduced 5%, 15%, and 40% for flaps pivoted 45, 90, and 180 degrees, respectively (29). When designing a pivotal flap, greater degrees of pivot usually require a longer flap to account for loss of effective length, and pivoting greater than 90 degrees should be avoided. Incidentally, the greater the amount of pivot of the flap, the larger the amount of redundant tissue at the base (standing cutaneous deformity).
Rotation Flaps
Rotation flaps are pivotal flaps with curvilinear design (Fig. 173.5). In general, rotation flaps involve transfer of tissue immediately adjacent to the defect and are best used for repair of triangular defects. When rotation flaps involve pivoting of tissue only, and no advancement component, the greatest wound closure tension has been shown to be at the site perpendicular to the periphery of the flap (30). Classically, rotation flaps are designed so that the length of the arc incision is four times the width of the defect. This configuration minimizes the need for any modifications. Rotation flaps have great flexibility in design, and position should be optimized so the flap border falls along aesthetic borders or RSTLs; in addition, flaps should be inferiorly based to facilitate lymphatic drainage. If the defect is not triangular, the defect can be modified to allow for removal of the standing cutaneous deformity at the inferior edge of the defect, thereby converting the wound to a triangular shape. Bilateral rotation flaps can be designed, with opposing flaps both transferred along curvilinear borders into the defect. When two opposing flaps are used, they result in a T-shaped scar (known as an O-to-T closure). Opposing rotation flaps can be of unequal lengths, depending on the surrounding tissue, aesthetic borders, and anatomic structures. A facial location that is particularly amenable to closure using opposing rotation flaps is the temple, with the T-shaped incision placed along the lateral canthal creases and the hairline.
TABLE 173.10 FLAP CLASSIFICATION BY DESIGN AND METHOD OF MOVEMENT
Pivotal flaps
Rotation flaps
Transposition flaps
Interpolated flaps
Advancement flaps
Uni-or bipedicled advancement flaps
V-Y or Y-V advancement flaps
Island advancement flaps
Hinge flaps
Figure 173.5 Rotation flap with semicircular design. Standing cutaneous deformity is removed at the base of the donor site.
Only gold members can continue reading. Log In or Register to continue