28 Limited Utility of Intraoperative MRI in Endoscopic Pituitary Surgery
Pituitary neoplasms represent 15 to 20% of all intracranial tumors. The overwhelming majority of pituitary tumors are low-grade adenomas. As with most low-grade neoplasms, total resection may be curative and therefore represents the goal of pituitary surgery.1 Additional goals of pituitary surgery are decompression of the optic apparatus and preservation or restoration of normal pituitary function.2 Unfortunately, large operative series show recurrence rates of 5 to 20% in various types of pituitary adenomas and gross total resection rates of 30 to 90%, signifying that complete cure may not always be possible.1 This may be attributed to the tumor’s invasion of the cavernous sinus, or envelopment of the carotid artery or the visual apparatus, leading to the surgeon’s intentionally leaving residual tumor or to the surgeon’s inability to visualize tumor remnants during the operation and leaving unintentional residual tumor. Attempts to evacuate tumor that is adherent to vital structures may lead to devastating complications and generally should be avoided, although sharp dissection in these situations may be feasible. On the other hand, incomplete visualization of the tumor may lead to postoperative residual tumor that could have been safely removed during the initial operation. Residual tumor requires treatment with radiation therapy, repeat operation, or pharmacotherapy, all of which could have been avoided had the residual tumor been appreciated during the first operation. These factors serve as a great impetus to continually improve the surgeon’s ability to visualize pituitary tumors and the surrounding structures.
Neurosurgeons employ numerous adjuncts to safely maximize the extent of tumor evacuation. Intraoperative ultrasound and echo probes permit the localization of the carotid arteries3 as well as localization of residual tumor.4,5 Intraoperative magnetic resonance imaging (IMRI), which continues to proliferate as high-power imaging units become more available and affordable, provides the surgeon with the ability to evaluate the extent of resection radiographically while the patient is still under anesthesia. A “second look” can be performed during the first operation to remove any residual tumor.6–11 Likewise, evolving hematomas, although rare in occurrence, can be visualized and treated before the patient leaves the operating room. Finally, endoscopy has increased the size of the operative field, permitting surgeons to see around corners by bringing the light source and the scope lens directly into the operative field and using angled scopes to see structures that are not in the direct line of sight.12–17 Both IMRI and endoscopy have similar functions, which increases the ability of the surgeon to remove the entire tumor safely. This chapter discusses the issues that will be involved in definitively determining whether one technology achieves this goal more effectively than the other or whether they provide complementary information.
 Intraoperative MRI
Intraoperative MRI
MRI technology, in combination with stereotaxis, was introduced into the operating room to maximize the safety and efficacy of surgery. In skull base surgery, it allows precise localization of vital structures such as the carotid artery and cranial nerves. Exact determination of their location in three-dimensional space in reference to the lesion boundaries and the resection cavity maximizes the surgeon’s ability to avoid and preserve those structures. Furthermore, MRI allows visualization of certain portions of the lesion that extend beyond normal lines of sight, such as the suprasellar cistern or the superior lateral aspect of the sella. Although conventional stereotaxis based on preoperative imaging also allows similar functions, any intraoperative shift of the anatomy renders these images useless. IMRI permits the surgeon to update the images and thus update the basis of stereotactic space. In addition, the appearance and consistency of certain portions of the lesion may not be readily discerned from normal tissue with the naked eye or magnification and may become apparent only with MRI after administration of intravenous contrast. Thus, intraoperative imaging may significantly enhance the safety of the operation as well as allow maximal resection of the lesion.18
The first intraoperative MR unit was introduced at the Brigham and Women’s Hospital (Boston, MA) and was described by Black et al.19 Since then, numerous IMRI suites have been introduced with a wide range of magnet strengths. Many of the high-power magnet suites rely on the principle of bringing the operating room to the MR suite. The patients may be positioned in the MRI donut, with the operation taking place within the confines of the imager. Alternatively, various permutations of moving imagers and operating room tables have been implemented to remove the patient from the imaging core and to allow comfortable positioning of the surgeon and staff. Although special nonferromagnetic instruments are required to operate in the proximity of the MRI donut, standard instruments may be used outside of the “fringe field,” generally several feet away from the magnet.
Alternatively, several MR imagers were designed with the principle of bringing the imaging technology into the operating room, while attempting to alter as little of the standard operating room setup as possible. Such magnets generally have low magnetic field strength and may be stored under the operating table. Standard operating instruments may be used.
 Low-Field-Strength IMRI
Low-Field-Strength IMRI
Low-field-strength imagers require minimal alteration of the operating room setup and workflow. The PoleStar N20 (Medtronic Navigation, Louisville, CO) uses a 0.15-tesla (T) magnet and has two vertical magnet poles (Fig. 28.1). The imager is mobile and may be stored in a recessed steel cage when not in use, allowing the operating room to be used for any procedure under standard protocols without MRI precautions. During IMRI-aided operations, the device is posi-tioned under the patient’s head and elevated to the operating field when imaging is desired. The imager allows a 15- × 20-cm field of view and does not impose restrictions on the positioning of the patient, enabling a full-lateral head position if required. Standard ferromagnetic instruments may be used when the imager is lowered but must be removed from the operating field during image acquisition. The mean additional time that was attributed to implementation of this imager has been reported as 1.1 hour, with a range of 0.5 to 2 hours.10
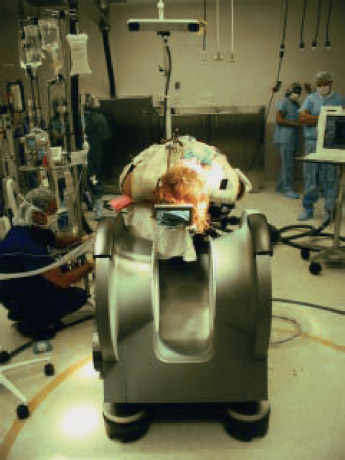
Fig. 28.1 An 0.15-Tesla imager installed at the University of Medicine and Dentistry of New Jersey Medical School.
A larger, nonmobile 0.2-T imager has been implemented at the University of Toronto. This imager also employs two vertical magnet poles. However, because the magnet is not mobile, the operating room table is moved into the imaging field when required and the operation is performed outside of the magnet to allow convenient access for two surgeons. Nonferromagnetic instruments are used inside the magnet, and regular instruments are used when the patient’s head is 60 to 90 cm outside of the field. A specially designed non-ferromagnetic nasal speculum and endoscopes are used in transsphenoidal surgery.6
An alternative 0.2-T imager (Open Viva, Siemens Medical Solutions, Hannover, Germany) uses two horizontally positioned magnets mounted on a C-arm (Fig. 28.2). The operating table has tilting and rotating capabilities allowing for placing the patient in Trendelenburg and reverse Trendelenburg positions and tilting the operating field to obtain optimal visualization. Standard operating instruments may be used when outside of the magnet field. However, when endoscopy was used, MR-compatible scope, light-source, camera, and LCD display were required. An average imaging time of 35 minutes was reported.8
The surgical team in the Oulu University Hospital in Finland has been using a 0.23-T, horizontally open imager. The magnet has fast shutdown and power-up capabilities (6 minutes). Thus, the operation is performed with the magnet turned off. When imaging is desired, non–MRI-compatible instruments, including electrocautery, endoscopes, operating microscope, and ferromagnetic instruments, are moved outside of the 5-mT line or into an adjacent room, and the magnet is turned on. Each imaging session requires approximately 30 to 40 minutes.20
Finally, a 0.3-T imaging unit (AIRIS II, Hitachi Medical Corp., Tokyo, Japan) has been actively employed at the University of Cincinnati Medical Center. The imager is similar to open-MRI systems that use two horizontal magnets. This imager is housed in a room that is adjacent to the standard operating room. The operation may take place in the standard operating room, and the patient is transported to the scanner through a sterile corridor, or the operation may be performed in the MRI room with the patient’s head positioned either within the imaging isocenter or outside of it. Each intraoperative scanning session added approximately 20 minutes to the operative time. Such setup allows the use of the MR imager for nonoperative imaging, although a 1-hour sterile cleansing procedure must be performed prior to operative imaging.21
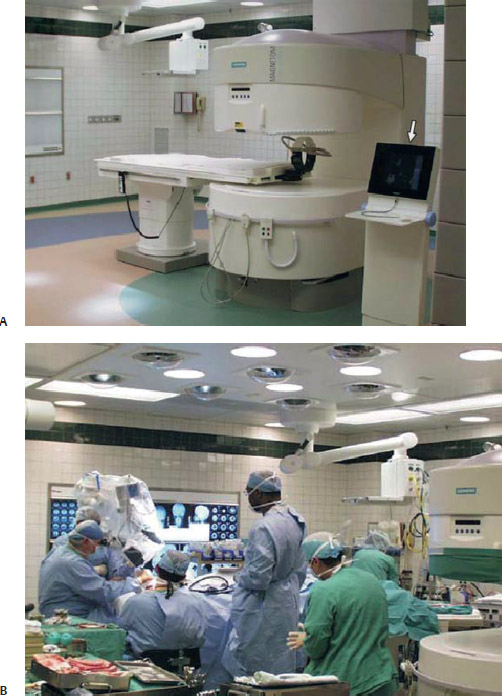
Fig. 28.2 (A) A 0.2-Tesla open intraoperative imager installed at the University Hospitals of Cleve-land/Case Western Reserve University. (B) When the operating table is outside of the scanner, standard operating room instruments may be used.
 Mid-Field-Strength IMRI
Mid-Field-Strength IMRI
Several centers employ a 0.5-T “double-donut” imaging system (Signa SP, General Electric Medical Systems, Milwaukee, WI) that was first used at the Brigham and Women’s Hospital (Fig. 28.3). The system uses two vertically oriented circular magnets with a vertical gap between them. The vertical gap between the two donuts allows access to the operative field for two surgeons. Because the patient’s head is positioned in the magnet isocenter at all times, all of the operating instruments and the microscope must be MR-compatible. This machine allows real-time imaging while operating without moving the patient or the imager.11,19
 High-Field Strength IMRI
High-Field Strength IMRI
A mobile 1.5-T imager was developed in Calgary, Canada (Innovative Magnetic Resonance Imaging Systems, Inc., Winnipeg, Manitoba, Canada). The ceiling-mounted magnet may be moved into the surgical field when imaging is desired (Fig. 28.4). This allows the use of standard operating equipment during the operations, as long as the ferromagnetic equipment is moved into the fringe zone during imaging. This imager avoids the movement of the patient during the operation, potentially improving the safety of the procedure.7 Positioning of the imager, acquisition of a set of T1-weighted images, and reexposure of the surgical field require approximately 25 minutes.
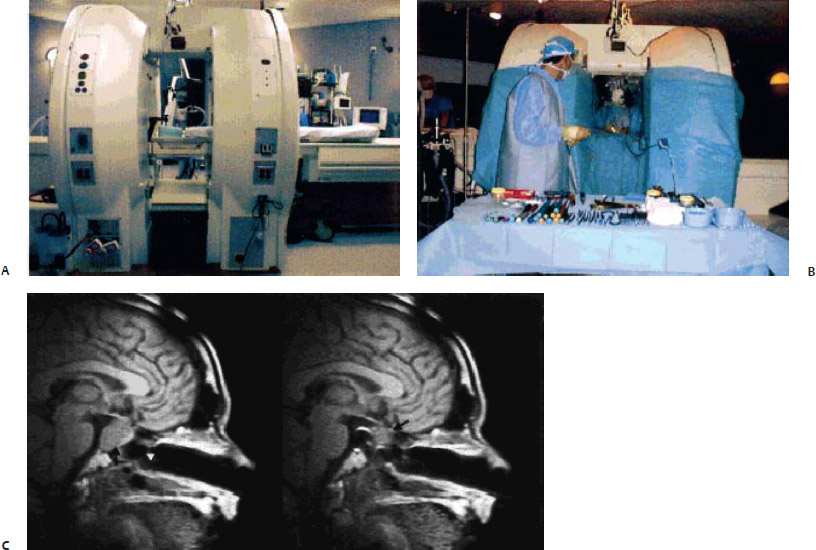
Fig. 28.3 (A) A 0.5-Tesla imager installed at Brigham and Women’s Hospital (Boston, MA). (B) The open design of the imager allows the surgeon to have access to the patient while imaging is in progress. (C) Intraoperative images of a sella tumor pre-resection and after partial resection with residual tumor identified.
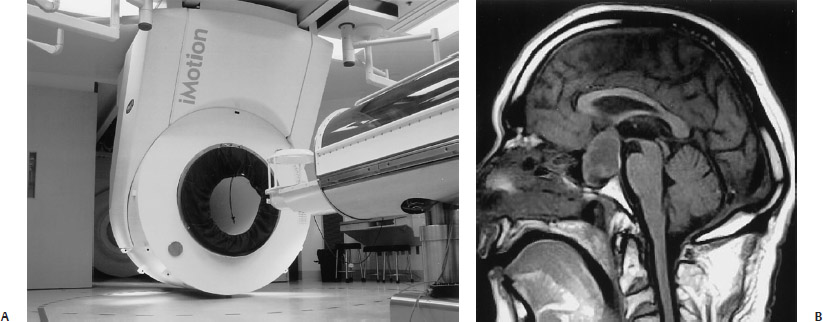
Fig. 28.4 (A) A 1.5-Tesla imager installed at the University of Calgary. The imager slides along a ceiling-mounted rail system, bringing the system to the operating field when required. (B) Image obtained prior to the start of resection shows a large pituitary tumor with su-prasellar extension.
A different 1.5-T imager (Magnetom Sonata Maestro Class, Siemens Medical Solutions) has been developed in Erlangen, Germany (Fig. 28.5
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


