Lids
The eyelids are thin structures comprised of skin, muscle, and fibrous tissue that serve to protect the eye. The great mobility of the lids is possible because the skin is among the thinnest of the body. Beneath the skin lies a very thin fibroadipose layer through which septa pass and closely adhere to the orbicularis oculi muscle. The orbicularis oculi muscle consists of striated muscle innervated on its deep surface by the facial nerve (cranial nerve VII). The muscle functions to close the lids and is divided into orbital, preseptal, and pretarsal divisions. The orbital portion, which functions primarily in forcible closure, is a circular muscle with no temporal insertion. The preseptal and pretarsal muscles are more involved in involuntary lid movements (blink). They have superficial and deep medial heads that participate in lacrimal pump function (see Lacrimal Apparatus).
The lid margins are supported by the tarsi, rigid fibrous plates connected to the orbital rim by the medial and lateral canthal tendons. The lateral canthus lies 1–2 mm higher than the medial. The orbital septum originates from the orbital rim and functions as an important barrier between the eyelids and the orbit. In the upper lid, the septum attaches to the levator aponeurosis which then joins the tarsus. Behind the septum lies the medial and the central or preaponeurotic fat pad, a helpful surgical landmark. In the lower lid, the septum joins the inferior border of the tarsus. The lower lid has three anatomically distinct fat pads beneath the orbital septum.
Deep to the fat lies the levator muscle complex—the principal retractor of the upper eyelid—and its equivalent, the capsulopalpebral fascia in the lower lid. The levator muscle originates in the apex of the orbit and is innervated by the oculomotor nerve (cranial nerve III). As it enters the eyelid, it forms an aponeurosis that attaches to the lower third of the superior tarsus. In the lower lid, the capsulopalpebral fascia originates from the inferior rectus muscle and inserts on the inferior border of the tarsus. It serves to retract the lower lid in downgaze. The superior (Müller’s muscle) and inferior tarsal muscle form the next layer, which is adherent to the conjunctiva. These sympathetically innervated muscles are also lid retractors. Conjunctiva lines the inner surface of the lids. It is continuous with that of the eyeball and contains glands essential for lubrication of the ocular surface.
The upper lid is larger and more mobile than the lower. A deep crease usually present in the mid position of the upper lid in Caucasian populations represents an attachment of levator muscle fibers. The crease is much lower or is absent in the Asian eyelid. With age, the thin skin of the upper lid tends to hang over the lid crease and may touch the eyelashes. Aging also thins the orbital septum and reveals the underlying fat pads.
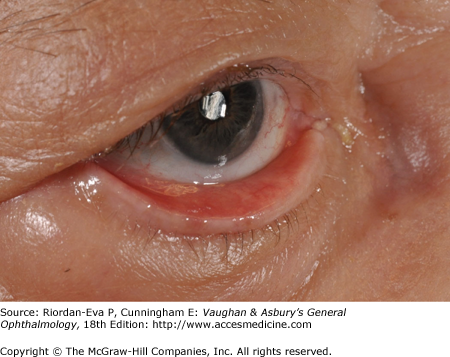
A hordeolum is an infection of one or more glands of the eyelid. When the meibomian glands are involved, it is called an internal hordeolum. An external hordeolum (sty) is an infection of a gland of Zeis or Moll.
Pain, redness, and swelling are the principal symptoms. The intensity of the pain is a function of the amount of lid swelling. An internal hordeolum may point to the skin or to the conjunctival surface. An external hordeolum always points to the skin.
Most hordeola are caused by staphylococcal infections, usually Staphylococcus aureus. Culture is seldom required. Treatment consists of warm compresses three or four times a day for 10–15 minutes. If the process does not begin to resolve within 48 hours, incision and drainage of the purulent material is indicated. A vertical incision should be made on the conjunctival surface to avoid cutting across the meibomian glands. The incision should not be squeezed to express residual pus. If the hordeolum is pointing externally, a horizontal incision should be made on the skin to minimize scar formation.
Antibiotic ointment is routinely applied to the conjunctival sac 4 times daily. Systemic antibiotics are indicated if cellulitis develops.
A chalazion (Figure 4–1) is a sterile, focal, chronic inflammation of the eyelid that results from obstruction of a meibomian gland. It is commonly associated with rosacea and posterior blepharitis. Symptoms begin with mild inflammation and tenderness that persists over a period of weeks to months. It is differentiated from a hordeolum by the absence of acute inflammatory signs. Most chalazia point toward the conjunctival surface, which may be slightly reddened or elevated. If sufficiently large, a chalazion may press on the globe and cause astigmatism. Excision is indicated if the lesion distorts vision or is cosmetically unacceptable.

Laboratory studies are seldom indicated, but on histologic examination, there is proliferation of the endothelium of the acinus and a granulomatous inflammatory response that includes Langerhans-type giant cells. Biopsy is indicated for recurrent chalazion, since sebaceous gland carcinoma may mimic the appearance of chalazion.
Surgical excision is performed via a vertical incision into the tarsal gland from the conjunctival surface followed by careful curettement of the gelatinous material and glandular epithelium. Intralesional steroid injections alone may be useful for small lesions, and in combination with surgery in difficult cases.
Anterior blepharitis (Figure 4–2) is a common, chronic bilateral inflammation of the lid margins. There are two main types: staphylococcal and seborrheic. Staphylococcal blepharitis may be due to infection with S aureus, Staphylococcus epidermidis or coagulase-negative staphylococci. Seborrheic blepharitis is usually associated with the presence of Pityrosporum ovale, although this organism has not been shown to be causative. Often, both types are present (mixed).

The chief symptoms are irritation, burning, and itching of the lid margins. The eyes are “red-rimmed.” Many scales or scurf can be seen clinging to the lashes of both the upper and lower lids. In the staphylococcal type, the scales are dry, the lids are erythematous, the lid margins are ulcerated, and the lashes tend to fall out. In the seborrheic type, the scales are greasy, ulceration does not occur, and the lid margins are less inflamed. Seborrhea of the scalp, brows, and ears is also frequently found. In the more common mixed type, both dry and greasy scales are present with lid margin inflammation and possible ulceration. Staphylococcal species and P ovale can be seen together or singly in stained material scraped from the lid margins.
Staphylococcal blepharitis may be complicated by hordeola, chalazia, epithelial keratitis of the lower third of the cornea, and marginal corneal infiltrates (see Chapter 6). Both forms of anterior blepharitis predispose to recurrent conjunctivitis.
Treatment consists of eyelid hygiene particularly in the seborrheic type of blepharitis. Scales must be removed daily from the lid margins by gentle mechanical scrubbing with a damp cotton applicator and baby shampoo.
Staphylococcal blepharitis is treated with antistaphylococcal antibiotic or sulfacetamide ointment applied on a cotton applicator once daily to the lid margins.
Both types may run a chronic course over a period of months or years if not treated adequately. Associated staphylococcal conjunctivitis or keratitis usually disappears promptly following local antistaphylococcal medication.
Posterior blepharitis (Figure 4–3) is inflammation of the eyelids secondary to dysfunction of the meibomian glands. Like anterior blepharitis, it is a bilateral, chronic condition. Anterior and posterior blepharitis may coexist. Seborrheic dermatitis is commonly associated with meibomian gland dysfunction. Colonization or frank infection with strains of staphylococci is frequently associated with meibomian gland disease and may represent one reason for the disturbance of meibomian gland function. Bacterial lipases may cause inflammation of the meibomian glands and conjunctiva and disruption of the tear film.

Posterior blepharitis is manifested by a broad spectrum of symptoms involving the lids, tears, conjunctiva, and cornea. Meibomian gland changes include inflammation of the meibomian orifices (meibomianitis), plugging of the orifices with inspissated secretions, dilatation of the meibomian glands in the tarsal plates, and production of abnormal soft, cheesy secretion upon pressure over the glands. Hordeola and chalazia may also occur. The lid margin shows hyperemia and telangiectasia, and may become rounded and rolled inward as a result of scarring of the tarsal conjunctiva, causing an abnormal relationship between the precorneal tear film and the meibomian gland orifices. The tears may be frothy or abnormally greasy. Hypersensitivity to staphylococci may produce a secondary keratopathy. The cornea may also develop peripheral vascularization and thinning, particularly inferiorly, sometimes with frank marginal infiltrates. Posterior blepharitis is often associated with rosacea (see Chapter 15).
Regardless of disease severity, the primary therapy is application of warm compresses to the eyelids, with periodic meibomian gland expression. Further treatment is determined by the associated conjunctival and corneal changes. Topical therapy with antibiotics is guided by results of bacterial cultures from the lid margins. Frank inflammation of the lids calls for anti-inflammatory treatment, including long-term therapy with topical metrogel (0.75% twice daily) and/or systemic doxycycline (50–100 mg twice daily). Short-term treatment with weak topical steroids (eg, prednisolone acetate, 0.125% twice daily) can be considered. Tear film dysfunction may necessitate artificial tears, but toxic reactions to preservatives need to be identified. Hordeola and chalazia should be treated appropriately.
Entropion is an inward turning of the lid margin (Figure 4–4). It may be involutional, spastic, cicatricial, or congenital. Involutional entropion is the most common and by definition occurs as a result of aging. It always affects the lower lid and is the result of a combination of horizontal eyelid laxity, disinsertion of the lower lid retractors, and upward migration of the preseptal orbicularis muscle.

Cicatricial entropion may involve the upper or lower lid and is the result of conjunctival and tarsal scar formation. It is most often found with chronic inflammatory diseases such as trachoma or pemphigoid.
Congenital entropion is rare and should not be confused with congenital epiblepharon, which usually afflicts Asians. In congenital entropion, the lid margin is rotated toward the cornea, whereas in epiblepharon, the pretarsal skin and muscle cause the lashes to rotate around the tarsal border.
Trichiasis is misdirection of eyelashes toward the cornea and may be due to entropion, epiblepharon, or simply misdirected growth. It causes corneal irritation and encourages ulceration. Chronic inflammatory lid diseases such as blepharitis may cause scarring of the lash follicles and subsequent misdirected growth.
Distichiasis is a condition manifested by accessory eyelashes, often growing from the orifices of the meibomian glands. It may be congenital or the result of inflammatory metaplastic changes in the glands of the eyelid margin.
Surgery to evert the lid is effective in all kinds of entropion. Useful temporary measures in involutional entropion are to tape the lower lid to the cheek with tension exerted temporally and inferiorly or to inject botulinum toxin. Trichiasis without entropion can be temporarily relieved by epilating the offending eyelashes. Permanent relief may be achieved with electrolysis, laser, cryotherapy or lid surgery.
Ectropion is an outward turning of the lid margin (Figure 4–5). It may be involutional, paralytic, cicatricial, mechanical or congenital. Involutional ectropion is the result of horizontal eyelid laxity from aging. Paralytic ectropion follows facial nerve palsy. Cicatricial ectropion is caused by contracture of the skin of the lid from trauma or inflammation. Mechanical ectropion usually occurs because of bulky tumors of the lid. Symptoms of tearing and irritation with exposure keratitis may occur with any type.
Involutional and paralytic ectropion can be treated surgically by horizontal shortening of the lid. Treatment of cicatricial ectropion requires surgical revision of the scar and often skin grafting. Correction of mechanical ectropion requires removal of the neoplasm followed by eyelid reconstruction.
Congenital coloboma is the result of incomplete fusion of fetal maxillary processes. The consequence is a lid margin cleft of variable size. The medial aspect of the upper lid is most often involved, and there is often an associated dermoid tumor. Surgical reconstruction can usually be delayed for years but should be done immediately if the cornea is at risk. A full-thickness eyelid defect from any cause is sometimes referred to as a coloboma.
Epicanthus is characterized by vertical folds of skin over the medial canthi. It is typical of Asians and is present to some degree in most children of all races. The skinfold is often large enough to cover part of the nasal sclera and cause “pseudoesotropia.” The eye appears to be crossed when the medial aspect of the sclera is not visible. The most frequent type is epicanthus tarsalis, in which the superior lid fold is continuous medially with the epicanthal fold. In epicanthus inversus, the skinfold blends into the lower lid. Other types are less common. Epicanthal skinfolds may also be acquired after surgery or trauma to the medial eyelid and nose. The cause of epicanthus is vertical shortening of the skin between the canthus and the nose. Surgical correction is directed at vertical lengthening and horizontal shortening. Epicanthal folds in normal children, however, diminish gradually by puberty and seldom require surgery.
The normal distance between the medial canthus of each eye, the intercanthal distance, is equal to the length of each palpebral fissure (approximately 30 mm in adults). A wide intercanthal distance may be the result of traumatic disinsertion or congenital craniofacial dysgenesis. Minor degrees of telecanthus (eg, blepharophimosis syndrome) can be corrected with skin and soft-tissue surgery. Major craniofacial reconstruction, however, is required when the orbits are widely separated, as in Crouzon’s disease (see Chapter 17).
Blepharochalasis (Figure 4–6) is a rare condition of unknown cause, sometimes familial, which resembles angioneurotic edema. Repeated attacks begin near puberty, diminish during adulthood, and cause atrophy of periorbital structures. Eyelid skin appears thin, wrinkled, and redundant and is described as resembling cigarette paper. A sunken appearance is the result of fat atrophy. Involvement of the levator aponeurosis produces moderate to severe ptosis. Medical management is limited to symptomatic treatment of edema. Surgical repair of levator dehiscence and excision of redundant skin is most likely to be successful after attacks have abated.

Dermatochalasis (Figure 4–7) is eyelid skin redundancy and loss of elasticity, usually as a result of aging. In the upper lid, the preseptal skin and orbicularis muscle, which normally forms a crease near the upper tarsal border in Caucasians, hangs over the pretarsal portion of the lid. When dermatochalasis is severe, the superior visual field is obstructed. Weakness of the orbital septum causes the medial and preaponeurotic fat pads to bulge. “Bags” in the preseptal region of the lower lid represent herniated orbital fat.


Blepharoplasty may be indicated for visual or cosmetic reasons. In the upper lid, superfluous eyelid skin is removed as well as muscle and fat for optimum aesthetics. Lower lid blepharoplasty is considered cosmetic surgery unless extreme redundancy contributes to ectropion of the lid margin. Pulsed CO2 and erbium lasers, while effective for facial aesthetic surgery, must be used with extreme caution in the periocular area.
Benign essential blepharospasm is an uncommon type of involuntary muscle contraction characterized by bilateral, synchronous, involuntary, spasms of the eyelids with onset typically during adulthood. The spasms tend to progress in force and frequency, resulting in a grimacing expression and involuntary closure of the eyes. Patients are incapacitated and often only able to experience only brief intervals of vision between spasms. When the entire face and neck are involved, the condition is known as Meige syndrome. Diagnosis is frequently delayed.
The cause of blepharospasm is not known, but studies have implicated dysfunction of the basal ganglia and a number of cortical and subcortical centers that control blinking. Emotional stress and fatigue sometimes make the condition worse.
It is important to differentiate benign essential blepharospasm from hemifacial spasm. The latter condition tends to be unilateral and to involve the upper and lower face. Hemifacial spasm can result from compression of the facial nerve by an artery or posterior fossa tumor. Jenetta’s neurosurgical decompression is the definitive mode of treatment; however, temporary neuromuscular blockade (see below) is less invasive and more frequently employed.
Other types of involuntary facial movements include tardive dyskinesia, which results from prolonged phenothiazine therapy and seldom affects the orbicularis muscle selectively; and facial tics, common in children, which are thought to be psychogenic.
The primary treatment of blepharospasm is repeated injections of botulinum toxin to produce temporary neuromuscular paralysis of the orbicularis oculi muscle. Rarely, unusual instances of psychoneurotic behavior may be identified that benefit from psychotherapy, neuroleptic drug treatment, biofeedback training, and hypnosis. If intolerance or unresponsiveness to botulinum toxin develops, selective extirpation of the orbicularis muscles or surgical ablation of the facial nerve can be performed.
The upper lid normally rests approximately midway between the superior limbus and the pupillary margin. Considerable variation may exist as long as symmetry is maintained. Blepharoptosis, or “ptosis,” as it is more commonly called, is the condition in which one or both upper eyelids assume an abnormally low position.
Blepharoptosis may be congenital or acquired (Table 4–1). Classification is important for selection of appropriate treatment.
| Congenital Ptosis |
| Myogenic |
| Simple |
| With superior rectus weakness |
| Blepharophimosis Syndrome |
| Neurogenic |
| Congenital oculomotor nerve palsy |
| Congenital Horner’s Syndrome |
| Marcus Gunn Jaw-Winking Syndrome |
| Congenital Fibrosis of the Extraocular Muscles |
| Mechanical |
| Eyelid mass (eg. capillary hemangioma) |
| Acquired Ptosis |
| Aponeurotic |
| Senescent (Involutional) |
| Trauma |
| Blepharochalasis |
| Pregnancy |
| Graves’ Disease |
| Myogenic |
| Chronic Progressive External Ophthalmoplegia |
| Oculopharyngeal Dystrophy |
| Myotonic Dystrophy |
| Myasthenia Gravis |
| Neurogenic |
| Acquired oculomotor nerve palsy |
| Ischemia (microvascular disease) |
| Trauma |
| Compression |
| Acquired Horner’s Syndrome |
| Levator muscle botulinum toxin injection |
| Mechanical |
| Pseudo-Ptosis |
| Dermatochalasis |
| Contralateral upper lid retraction |
| Hypotropia |
| Reduced orbital volume |
| Enophthalmos |
| Microphthalmos |
| Phthisis Bulbi |
Congenital myogenic ptosis is the result of an isolated dystrophy of the levator muscle affecting both contraction and relaxation of the fibers. Ptosis is present in the primary position of gaze, and there is reduced movement of the lid in upgaze and impaired closure on downgaze. Lid lag on downgaze is an important clue to diagnosis of levator maldevelopment. Other ocular abnormalities, such as strabismus, may be present. In 25% of cases, the superior rectus muscle shares the same dystrophic changes as the levator, resulting in weakness of upgaze. Successful surgical outcome in the presence of superior rectus weakness requires the resection of an additional length of levator.
Blepharophimosis syndrome accounts for 5% of cases of congenital ptosis. Severe ptosis with poor levator function is accompanied by telecanthus, epicanthus inversus, and sometimes ectropion of the lower lids. It can also be associated with premature ovarian failure in females. The condition is autosomal dominant and caused by a mutation in the FOXL2 gene on chromosome 3.
Congenital oculomotor nerve palsy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


