Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

19

Leukocoha
When white light enters the eye, it passes through the transparent ocular media (i.e., cornea, aqueous, lens, and vitreous) until it reaches the retina and choroid. The highly vascular choroid is responsible for the normal red fundus glow. The red reflex is the blurred illuminated image of the patient’s retina that is formed in the pupillary plane.
Under normal circumstances, the pupil of a patient will appear black when examined with a penlight. The red reflex can be observed only when the observing eye and the illuminating point are coaxial. This alignment can be easily achieved by using a direct ophthalmoscope. The red reflex should be evaluated in a darkened room using a bright direct ophthalmoscope light. Normally the red reflex from both pupils should be symmetrical. Slight luminosity of the pupil may be seen with a penlight examination in highly hyperopic eyes and in pathological conditions where the retina is displaced forward as in retinal detachment or an intraocular tumor. The emergent rays under these circumstances are divergent; therefore, it is not necessary for the observing eye to be coaxial, and the pupil will appear feebly illuminated even with a penlight examination (Figs. 19-1 and 19-2).

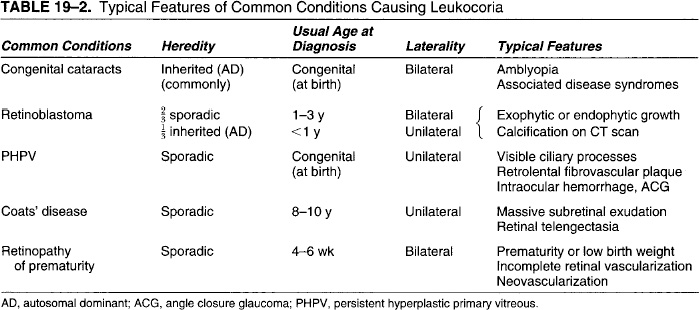
FIGURE 19-1. Unilateral leukocoria (left eye).
Leukocoria literally means “white pupil.” It is a gross sign of intraocular pathology. Ocular conditions that interrupt the path of the light rays as they strike the vascular choroid may cause a whitish reflex to be produced at the pupil instead of the normal red reflex (Table 19-1). Because enucleation, chemotherapy, and radiation are favored treatments for malignant lesions such as retinoblastoma, the problem of differentiating nonmalignant lesions is more than academic.1 Table 19-2 lists important differentiating features of common conditions that cause leukocoria. Leukocoria is an important clinical sign that should prompt an urgent detailed general physical and ophthalmologic examination to identify the underlying pathology. Table 19-3 lists some of the signs that may help to identify the underlying pathology.

FIGURE 19-2. Bilateral leukocoria.
| Congenital |
| Cataracts |
| Persistent hyperplastic primary vitreous |
| Retinopathy of prematurity |
| Familial exudative vitreoretinopathy |
| Coats’ disease (retinal telengectasia) |
| Fundus colobomas |
| Medullated nerve fibers |
| Tumors |
| Retinoblastoma |
| Astrocytoma |
| Diktyoma |
| Infections |
| Endophthalmitis |
| Toxocariasis |
| Toxoplasmosis |
 Congenital Cataracts
Congenital Cataracts
Cataracts are the most common cause of childhood leukocoria (Fig. 19-3). Visually disabling, bilateral, congenital cataracts often present with early nystagmus (by 3 months), which is indicative of a poor prognosis for visual recovery. Early surgical removal of congenital cataracts is associated with the best visual prognosis. Congenital cataracts are reported to occur in 1 out of 250 newborns.2,3 It is significant that approximately one third of cataracts in children arehereditary, another third are associated with various syndromes or other diseases, and the final third are idiopathic.4 Genetic and metabolic disease syndromes (e.g., Down syndrome, Lowe’s syndrome, galactosemia) and intrauterine maternal infections with TORCH (toxoplasmosis, other infections, rubella, cytomegalovirus, herpes simplex) organisms are known specific causes of congenital cataracts.

FIGURE 19-3. Congential cataract prominently visible in the pupil of the right eye.
Congenital cataracts can be polar (anterior or posterior), sutural, nuclear (pearly white nuclear cataract of rubella), capsular, or lamellar (most common). Of the various morphologic types of cataracts, anterior polar, posterior lentiglobus, and unilateral persistent hyperplastic primary vitreous (PHPV) are not usually related to systemic disorders. Many of the metabolic diseases can be treated, or further deterioration can be prevented with appropriate treatment.5 Modern diagnostic techniques such as ultrasonography or magnetic resonance imaging can help identify posterior segment lesions behind the lens and opacified lens.6
Early surgical intervention (as soon as possible) and visual rehabilitation are the mainstays of management for visually significant congenital cataracts. A lensectomy (limbal or pars plana approach) is usually performed. Posterior capsulectomy and anterior vitrectomy are usually performed to prevent posterior capsular opacification. Visual rehabilitation is obtained with an intraocular lens (preferred, depending on age), contact lens, or aphakic glasses. Postoperative amblyopia therapy may require eye patching.
 Retinoblastoma
Retinoblastoma
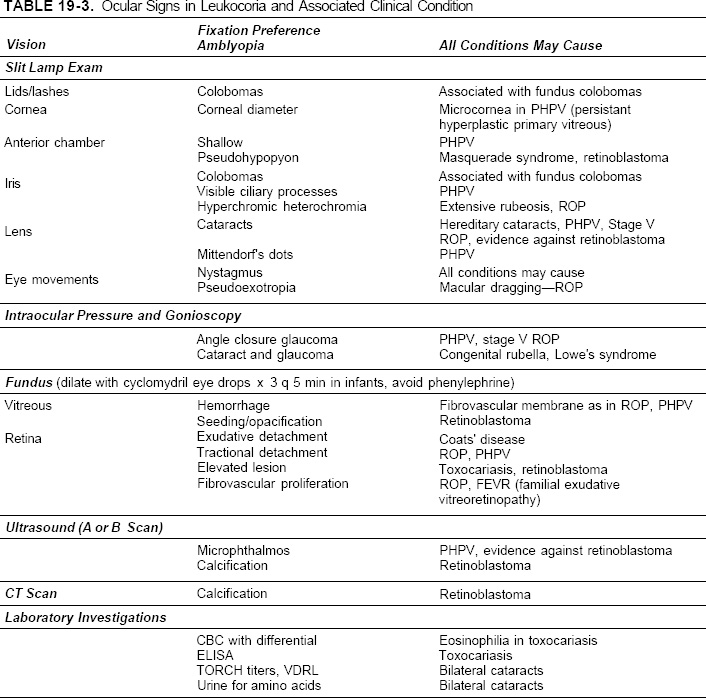
Retinoblastoma is the most common malignant intraocular tumor of childhood.7,8 It is a neuroblastic tumor that is caused by a mutation in the long arm of chromosome 13. It is familial in one third of cases (bilateral tumors) and sporadic in two thirds of cases (unilateral tumors)and typically is diagnosed at approximately 1 year of age. The most common initial sign is leukocoria (Fig. 19-4) followed by strabismus. Two growth patterns have been identified: endophytic, which occurs when tumor breaks through the internal limiting membrane and is visible in the vitreous cavity as a whitish mass (Fig. 19-5), and exophytic, which occurs when tumor grows in the subretinal space producing a yellowish mass with overlying dilated and tortuous retinal vessels (Fig. 19-6). Radiographic or ultrasonographic demonstration of intraocular calcification aids in the diagnosis. Treatments include enucleation external-beam radiotherapy, radioactive plaque treatment, cryotherapy, and photocoagulation. Radiotherapy or chemotherapy may be used in an attempt to preserve at least one globe in bilateral cases.

FIGURE 19-4. Leukocoria secondary to retinoblastoma.
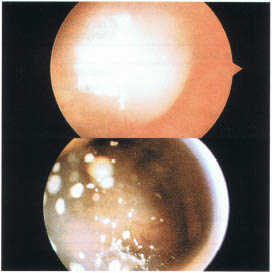
FIGURE 19-5. Fundus photograph of retinoblastoma, endophytic type.
 Persistent Hyperplastic Primary Vitreous
Persistent Hyperplastic Primary Vitreous
Present at birth, persistent hyperplastic primary vitreous (PHPV) is unilateral in over 90% of cases. When it presents bilaterally, chromosomal defects may be present. Pathophysiologically, PHPV develops when the fibrovascular component of the primary vitreous fails to involute by the seventh month of gestation when the secondary or mature vitreous develops. PHPV presents as a white fibrovascular mass behind or extending to the lens. Leukocoria may result from the PHPV material itself or from the secondary cataract that frequently is present (Fig. 19-7). The eye is slightly microphthalmic and on dilation of the pupil may show elongated ciliary processes, which are particularly diagnostic of this disorder. Various degrees of severity may occur, ranging from mild persistent stalks that do not interfere with visual function and development to massive retinal tractional detachments and intraocular hemorrhage. Some time later, the eye also may lose all useful vision from secondary angle closure glaucoma as the lens swells. Modern surgical techniques have salvaged many eyes; however, the risk of glaucoma remains.9
FIGURE 19-6. Fundus photograph of retinoblastoma, exophytic type.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


