Management of petrous apex pathology poses a unique challenge even to the most seasoned skull base surgeons. The central location in the skull base with adjacent critical neurovascular structures makes access to this region more than a trivial matter. Significant advances in diagnostic imaging have greatly facilitated the diagnosis of petrous apex lesions. The introduction of modern skull base surgery techniques also has provided skull base surgeons with numerous avenues to the petrous apex while significantly decreasing morbidity. The latest diagnostic and management strategies are discussed and an update of some of the more common pathologic entities is provided.
Anatomy
The petrous apex is a pyramid-shaped structure that is the most medial aspect of the temporal bone. The base of the pyramid is the otic capsule, semi-canal of the tensor tympani and the petrous carotid artery. The superior surface—or meatal plane—extends from the arcuate eminence to the precavernous carotid artery and Meckel’s cave. The posterior surface faces the cerebellopontine angle and begins laterally at the common crus/vestibular aqueduct and ends medially at Dorello’s canal and petroclinoid ligament. The jugular fossa and inferior petrosal sinus are located at the inferior aspect of the petrous apex. The internal carotid artery enters the petrous apex along the inferior surface via the carotid canal. The internal auditory canal begins at the porus acousticus on the posterior face of the petrous apex and ends at the fundus. When viewed from above, the petrous apex may be divided into anterior and posterior segments by drawing a parallel line through the internal auditory canal. The cochlear aqueduct enters the petrous apex along its inferior surface just medial to the jugular fossa. The petrous apex is primarily composed of bone marrow or dense bone, with only 9% to 30% of subjects showing some pneumatization. Pneumatization of the petrous apex is variable and often differs among sides in the same subject .
Presentation
Petrous apex lesions can present with various symptoms and signs, depending on the size, location, and nature of the pathologic process. Muckle and colleagues reported hearing loss as the most common symptom followed by vestibular dysfunction, headache, tinnitus, facial spasm, diplopia, facial paralysis, and otorrhea. Symptoms often present months or years before diagnosis, and incidental discovery is not uncommon.
Presentation
Petrous apex lesions can present with various symptoms and signs, depending on the size, location, and nature of the pathologic process. Muckle and colleagues reported hearing loss as the most common symptom followed by vestibular dysfunction, headache, tinnitus, facial spasm, diplopia, facial paralysis, and otorrhea. Symptoms often present months or years before diagnosis, and incidental discovery is not uncommon.
Imaging
CT
CT of the temporal bone enables a detailed evaluation of the osseous architecture of the petrous apex. Lesions within or involving the petrous apex may be further characterized based with CT by evaluating for different patterns of bone erosion or invasion. A distinct advantage of CT is the ability to determine the proximity of a petrous apex lesion—with submillimeter accuracy—to critical structures, such as the internal auditory canal, otic capsule, and carotid artery. CT is often complementary to MRI in evaluating petrous apex pathology .
MRI
Before the introduction of MRI, evaluation of petrous apex pathology was limited to evaluating changes in the temporal bone with plain films, tomography, and early CT. In most cases, MRI with the history and physical examination allows the clinician to make a diagnosis without obtaining tissue for pathologic examination. Most of the reported petrous apex lesions have unique MRI characteristics that allow for definitive diagnosis ( Table 1 ) .
| MRI | ||||||
|---|---|---|---|---|---|---|
| Lesion | T1 pre | T1 post | T1 fat saturated gadolinium | T2 | CT | Other |
| Cholesterol granuloma | Hyperintense | No enhancement | Hyperintense | Smooth erosion | ||
| Petrous apicitis | Hypointense | Rim enhancement | Rim enhancement | Hyperintense | Destroyed septae | |
| CSF cyst/cephalocele | Hypointense | No enhancement | No enhancement | Hyperintense | Smooth erosion, FLAIR, hypointense, diffusion-weighted, hypointense | May connect to Meckel’s cave |
| Epidermoid | Hypointense | No enhancement | Hyperintense | FLAIR – hyperintesne, diffusion-weighted imaging, hyperintense | ||
| Effusion | Isointense or hypointense | Enhancement | Hyperintense | Intact septation | ||
| Mucocele | Isointense | No enhancement | No enhancement | Hyperintense | Destroyed septae | |
| Asymmetric pneumatization | Hyperintense | Some enhancement | Hypointense, no enhancement | Hypointense | Marrow on lesion side, air cells on contralateral side | |
| Carotid aneurysm | New thrombus, hypointense; older thrombus, hyperintense | Hyperintense | Smooth expansion of carotid canal, heterogeneous contrast enhancement | MRI, central flow void, onion skin appearance | ||
| Chordoma | Hypointense/isointense | Enhancement less intense than chondrosarcoma | Enhancement | Hyperintense | Lobulated, bone destruction with residual bone fragments | Centrally located in clivus with lateral spread to petrous apex |
| Chondrosarcoma | Hypointense/isointense, homogeneous | Enhance | Enhancement | Hyperintense, heterogeneous | Infiltrative, remnants of eroded bone | Centered in petrous apex in region of foramen lacerum, calcified areas may show as signal voids |
| Metastasis | Depends on primary | Enhancement | Enhancement | Depends on primary | Bone erosion | Depends on primary tumor |
| Paraganglioma | Isointense | Enhancement | Enhancement | Hyperintense | Opacified and destroyed air cells | Flow voids, blush on angio, salt and pepper |
| Meningioma | Isointense/hyperintense | Enhancement | Enhancement | Isointense/hyperintense | Hyperostosis, isointense or hyperdense, calcification | Dural tails, sessile, eccentric |
| Schwannoma | Isointense | Enhancement | Enhancement | Hyperintense or hypointense | May show dilation of internal auditory canal | Centered in internal auditory canal |
Angiography: conventional, magnetic resonance angiography, magnetic resonance venography, computed tomography angiography/venography
Petrous apex lesions may compress, invade, or abut the carotid artery, jugular bulb, and inferior and superior petrosal sinuses. Angiographic studies provide detailed information about these vascular structures and may help the surgeon to select an appropriate surgical approach. Conventional angiography via femoral artery or vein catheterization provides an opportunity to assess a lesion’s vascularity and its relationship to other vascular structures . This technique also provides an opportunity to devascularize lesions and extensive feeding vessels to decrease intraoperative blood loss . The primary disadvantage of conventional angiography is its risk of hematoma, stroke, pseudoaneurysm formation, and risk of cranial nerve palsies . The introduction of magnetic resonance angiography and venography has provided a low-risk technique of assessing the skull base vasculature. Although the resolution of these studies is good, the primary disadvantage of magnetic resonance angiography/venography is the inability to perform interventional measures . CT angiography and venography allow for another detailed means of assessing petrous apex lesions and vessels. This technique uses ultra-thin slices with timed administration of contrast and provides incredible detailed information. An additional advantage of temporal bone CT angiography compared with its counterparts is the ability to define the vascular structures and their relationship with the lesion and other structures in or adjacent to the petrous apex .
Management
Surgical approaches
Nonhearing preservation
Infracochlear
Traditionally, the most common approach to cystic lesions of the petrous apex in patients with serviceable hearing was the infralabyrinthine approach. This approach is limited in patients with a high jugular bulb, however. The alternative in these patients is the infracochlear approach to the petrous apex . There are several advantages to the infracochlear approach, including dependent drainage in a well-aerated middle space adjacent to the eustachian tube, adequate access to the petrous apex despite a high jugular bulb, simple revision if required, and preservation of the normal middle ear mechanisms .
Continuous intraoperative facial nerve monitoring is recommended. A standard postauricular incision is made. An incision is made in the mastoid periosteum along the linea temporalis and is extended inferiorly to the mastoid tip. The periosteum is elevated anteriorly until the osseous external auditory canal is exposed. The external auditory canal is transected through the cartilaginous portion. Canal incisions are made at 2 and 10 o’clock, and a tympanomeatal flap is elevated. The tympanic membrane remains attached to the umbo and superior canal wall. Removing an adequate amount of anterior and inferior tympanic bone within the external auditory canal is a critical step to expose the hypotympanum. Once exposure is adequate, the chorda tympani nerve can be traced posteriorly and inferiorly to identify the facial nerve. Next the jugular bulb and petrous carotid artery are identified. Once these structures have been identified, medial dissection continues with diamond burs and curettes. The boundaries of the dissection include the carotid artery anteriorly, the jugular bulb inferiorly, the facial nerve posteriorly, and the basal turn of the cochlea superiorly. Jacobson’s nerve can be followed inferiorly and leads to the bone between the carotid artery and jugular bulb. Confining the exposure inferior to the round window prevents inadvertent injury to the basal turn of the cochlea during dissection. The cyst is entered and the loose contents are removed using suction and irrigation. A piece of Silastic tubing is placed in the surgical defect. The bony defect of the inferior bony annulus is repaired with bone pate. The tympanomeatal flap is returned to its normal position. The external auditory canal is packed with Gelfoam, and the postauricular incision is closed .
Brackmann and Toh reported a recurrence rate of 16.7% in cholesterol granulomas treated with the infracochlear approach. Fibrous occlusion of the drainage tract was responsible for all failures. The use of Silastic tubing decreases the rate of recurrence in infralabyrinthine and infracochlear approaches . Because recurrence can occur years after the initial surgery, long-term radiographic follow-up is necessary. Preoperative symptoms of hearing loss, vertigo, and cranial nerve deficits often improve or resolve after treatment . Complications are rare; however, inadvertent injury to the carotid artery is a potentially devastating injury. The infracochlear approach to the petrous apex should be performed by a surgeon with an intimate knowledge of the anatomy.
Subtemporal approaches
The subtemporal approaches provide varying degrees of exposure to the petrous apex, clivus, ventral brainstem, and anterior cerebellopontine angle . The standard and extended middle fossa approaches provide excellent exposure of the internal auditory canal from the porus acousticus to the fundus . The extended approach requires more extensive bone removal anterior and posterior to the internal auditory canal. This additional bone removal, which exenterates a significant portion of the anterior and posterior petrous apex, provides additional exposure to the cerebellopontine angle. The anterior limit of dissection is the lateral wall of Meckel’s cave, whereas the posterior limit is the blue-lined superior semicircular canal . The Kawase approach is a further elaboration of the extended middle fossa approach that requires downfracturing of the zygoma . This approach provides access to the ventral pons by removing the anterior petrous apex down to the level of the horizontal petrous carotid artery. The primary disadvantage of the subtemporal approaches is an increased risk of facial nerve injury because of its anterior superior location in the internal auditory canal; however, several studies have demonstrated no long-term difference . Temporal lobe injury from prolonged retraction or injury to the vein of Labbé is also an important consideration when using these approaches . The subtemporal approaches do not permit visualization of the inferior cerebellopontine angle. The subtemporal approaches may be combined with the pre- and postsigmoid approaches to address lesions that extend into multiple intracranial compartments .
Various skin incisions may be used for the subtemporal approaches. Once the skin and subcutaneous tissues are elevated, the temporalis muscle is cut just proximal to its origin from the temporal line to provide a site of attachment during closure. The temporalis muscle is elevated anteriorly and inferiorly and is secured with retractors or hooks. Identification of the zygoma and the osseous external auditory canal provides landmarks for the craniotomy bone flap. A 4 cm × 5 cm craniotomy bone flap that is centered 1.5 cm anteriorly to the root of zygoma is elevated. Occasionally, additional squamous temporal bone cortex must be removed so that the craniotomy is flush with the middle fossa floor. Once the craniotomy bone flap has been elevated, the dura is elevated off the floor of the middle fossa from posterior to anterior to prevent avulsion of the greater superficial petrosal nerve. The dura is elevated from the petrous ridge posteriorly to the dura of Meckel’s cave anteriorly. Cauterization or clipping of the middle meningeal is often necessary. The greater superficial petrosal nerve, arcuate eminence, petrous ridge, middle meningeal artery, and foramen ovale all serve as landmarks to guide the surgeon. House , Fisch , and Jackler each described three separate techniques to identify the internal auditory canal. A lateral to medial technique, described by Fisch, begins by blue-lining the superior semicircular canal and then identifying the internal auditory canal at a 60° degree angle. William House identified the fundus of the internal auditory canal by tracing the greater superficial petrosal nerve to the geniculate ganglion. Jackler and Gladstone described a medial to lateral technique that begins with drilling at the petrous ridge and identifying the internal auditory canal at the porous acousticus and following it laterally to the fundus. Once tumor removal is complete, air cells are waxed and muscle or fat is used to obliterate the defect.
Infralabyrinthine approach
During the preantibiotic era, the infralabyrinthine approach was most commonly used to drain petrous apex abscesses . With the advent of antibiotics, petrous apex infections are rare; however, the same approaches can be used to drain cystic lesions of the petrous apex. The advantages of the infralabyrinthine approach to the petrous apex include an anatomy familiar to most otologists, direct route to most cysts of the petrous apex, and avoidance of entering the middle ear. A high-riding jugular bulb may necessitate the use of the infracochlear approach as opposed to the infralabyrinthine approach.
The surgical procedure begins with a simple mastoidectomy. The middle fossa plate, sigmoid sinus, and facial nerve are identified. The posterior portion of the lateral semicircular canal and the posterior semicircular canal are skeletonized, with care taken not to create a fistula in the semicircular canals. Next, the sigmoid sinus is followed inferiorly until the jugular bulb is identified. The boundaries of the approach include the posterior semicircular canal, facial nerve, jugular bulb, and the posterior fossa dura. Medial dissection continues with diamond burs and curettes until the cyst is entered. The loose contents of the cyst are removed with suction and irrigation. A piece of Silastic tubing is placed through the surgical tract to prevent restenosis of the surgical drainage tract.
Complications reported as a result of the infralabyrinthine approach include sensorineural hearing loss and facial nerve paresis . Preoperative deficits, including hearing loss, imbalance, and cranial nerve neuropathies, may resolve after surgery, depending on the lesion. Long-term radiographic follow-up is necessary because recurrences can occur years after drainage. Importantly, the lack of aeration alone postoperatively should not be considered a failure; however, increased size of the lesion or return of symptoms is a sign of recurrence and may require re-exploration.
Subarcuate and sinodural angle approaches
The subarcuate and sinodural angle approaches are mainly used in suppurative processes of the petrous apex. These approaches are rarely used because of the limited access provided. A standard mastoidectomy is used in both approaches. In the subarcuate approach all three semicircular canals are skeletonized. A small diamond bur is used to open the area inferior to the superior semicircular canal and superior to the vestibule that follows the path of the subarcuate artery. In cases of suppuration of the posterior petrous apex, fistulous tracts may be found in this pathway and can be followed to the petrous apex. The sinodural angle is another avenue that can be followed to the posterior petrous apex, where air cells of the sinodural angle are followed to the posterior petrous apex .
Supracochlear approach
The supracochlear approach allows for drainage or biopsy of lesions located on the anterior superior aspect of the petrous apex. This approach begins with a standard mastoidectomy followed by an extended antrotomy that exposes the zygomatic root cells. In some cases the incus body and occasionally the malleus head must be removed. Drilling with a 2- to 3-mm diamond bur begins anterior to the superior semicircular canal, between the tegmen tympani and the tympanic facial nerve. In the series by Telischi and colleagues of 20 temporal bones, removal of the incus was required in many of the specimens to access the supracochlear air cell tract. Telischi found that the mean dimensions of the supracochlear triangle are 7.0 × 5.3 × 4.8 mm. The advantage of this approach, which provides access to the anterior superior petrous apex, is preservation of the external auditory canal and labyrinth. Unfavorable aspects of this approach include a significant risk to the labyrinthine facial nerve and the potential need for removal of the malleus head and incus. Intraoperative facial nerve monitoring is recommended with this approach because of the proximity of the tympanic and labyrinthine facial nerve.
Retrosigmoid approach
The retrosigmoid approach gives excellent access for tumors that arise in the cerebellopontine angle and involve the posterior cranial fossa. This approach is limited when tumors extend into the middle fossa and involve Meckel’s cave, however. In 1995, Cheung and colleagues described an approach combining a retrosigmoid craniotomy with opening of Meckel’s cave by removing bone anterior to the internal auditory canal. Samii and colleagues later reported a series of 12 petroclival meningiomas approached through a similar approach called the retrosigmoid intradural suprameatal approach. The suprameatal extension of the retrosigmoid approach allows improved access to the petrous bone anterior to the internal auditory canal and allows better visualization of the prepontine cistern, clivus, oculomotor nerve, and the posterior cerebral arteries.
Seoane and Rhoton studied the anatomic relationships concerning the suprameatal approach to Meckel’s cave. The suprameatal tubercle is a bony prominence superior to the internal auditory canal and blocks access to Meckel’s cave, the prepontine cistern, and clivus from a posterior approach. Removal of this bone allows approximately 1 cm additional exposure of the posterior root of the trigeminal nerve and an additional 1.3 cm of anterior extension to the retrosigmoid approach. This approach is most ideal for petroclival meningiomas or posterior fossa trigeminal schwannomas with a limited amount of middle fossa involvement. Disadvantages include drilling in a tight space with adjacent critical neurovascular structures, poor access to the cavernous sinus, and further working distance to the petrous apex when compared with other approaches .
Combined approaches
The combined approaches provide exposure for lesions that extend in the middle and posterior fossa. These approaches typically use a transtemporal approach (retrolabyrinthine, translabyrinthine, and transcochlear) in addition to a middle fossa craniotomy. The technical details of this approach already have been described except for several critical steps. The superior petrosal sinus must be divided after cauterization or placement of clips. After the transtemporal and middle fossa craniotomies are completed, the tentorium is divided being careful not to injure the trochlear nerve, Dandy vein, superior cerebellar artery, and vein of Labbé . Prolonged retraction of the temporal lobe dura poses a risk of injury or thrombosis of the vein of Labbé. Intermittent release of the retractor or division of the sigmoid sinus may prevent injury to the vein of Labbé . The primary advantages of these combined approaches are decreased brain retraction, which eliminates the need for a staged approach, improved exposure, which allows for a more complete excision, and the possibility of hearing preservation (retrolabyrinthine). The primary disadvantage to the combined craniotomy is sacrifice of hearing if either the translabyrinthine or the transcochlear approach is used .
Infratemporal approach
The preauricular infratemporal approach and its modifications provide generous access to the petrous apex and clivus. Various incisions have been used and described for the infratemporal approach, including a Y incision, a large postauricular C-shaped incision, and a pretragal incision . The skin flaps are elevated over the temporalis fascia until the temporal fat pad is identified. An incision is made in the superficial layer of the deep temporal fascia and dissection proceeds just lateral to the temporal fat down to the level of the zygoma. The periosteum of the zygoma is transected along its superior-medial surface and elevated to preserve the frontal branch of the facial nerve. Identifying the main trunk of the extratemporal facial nerve at the stylomastoid foramen allows for more generous inferior exposure of the infratemporal fossa. The zygoma is exposed from the root to the orbital rim. Miniplate drill holes are placed before performing the zygomatic osteotomy for later reconstruction. The zygoma is then transposed inferiorly with the attached masseter muscle.
The temporalis muscle is cut along its origin, taking care to preserve a cuff of muscle for later reattachment if necessary. The temporalis is carefully reflected inferiorly toward its insertion on the coronoid process so as not to interrupt the vascular supply. The mandibular condyle is displaced out of the glenoid fossa with a retractor or can be resected to provide more generous exposure. A high-speed otologic drill is then used to remove the glenoid fossa and expose the petrous carotid artery. The eustachian tube serves as a useful landmark for the carotid artery and must be obliterated. Division and cauterization of the mandibular division of the trigeminal nerve and middle meningeal artery permits exposure of the precavernous petrous carotid artery and the anterior clivus. Once the petrous carotid artery has been skeletonized, generous exposure of the anterior petrous apex and clivus is afforded. Inferior mobilization of the carotid artery provides improved visualization of the petrous apex and clivus but is associated with an additional risk of inadvertent injury or vasospasm. If a large defect is present, the temporalis muscle may be rotated into the defect. Lesions that extend into the middle ear may require additional exposure .
Transnasal endoscopic approach
Endoscopic-assisted pituitary surgery has become the favored technique in many centers, with resulting decreased hospital stay, decreased recovery times, and better visualization for tumor excision . More recently, several centers have pushed the envelope by performing transnasal endoscopic approaches to posterior, middle, and anterior cranial base lesions. Kassam and Jho recently reported on a modular approach to accessing posterior fossa lesions, including the petrous apex and jugular foramen, via a transnasal endoscopic approach. These techniques require intimate knowledge of the complex skull base anatomy. Petrous apex cholesterol granulomas and epidermoids occasionally can be drained into the sphenoid sinus if the carotid artery is not in the drainage pathway . Kassam and colleagues also described an endoscopic technique that mobilizes the petrous carotid artery to access the petrous apex. These endoscopic skull base techniques hold the same potential promise that endoscopic pituitary approaches provide but require advanced knowledge and training.
Translabyrinthine approach
The translabyrinthine approach was reintroduced by Drs. Hitselberger and House , and with the introduction of the operating microscope, initiated the era of modern skull base surgery. This approach is often used in the surgical management of petrous apex lesions when hearing is poor or the tumor is large .
A postauricular incision is made to expose the mastoid periosteum. The mastoid periosteum is divided carefully so as not to overlap the cutaneous incision from the periosteal incision. Once the periosteum is dissected from the cortex, an extensive mastoidectomy is performed carefully so as to identify the mastoid tegmen, posterior fossa plate, sigmoid sinus, and external auditory canal. The antrum is opened and the lateral semicircular canal is identified along with the previously mentioned structures. A labyrinthectomy is performed, leaving the ampullated end of the superior semicircular canal as a landmark. The internal auditory canal is then identified, and a thin layer of bone is left over its surface. Removing bone inferior and superior to the internal auditory canal often exposes air cells or pathology involving the anterior petrous apex. This approach gives wide exposure to the posterior petrous apex and adequate exposure to the anterior petrous apex. The primary disadvantages of this approach are the loss of any residual hearing, worsening balance function, and vertigo that occurs immediately after the surgery. There is also a significant risk of a cerebrospinal fluid (CSF) leak if the dura is violated. An abdominal fat graft is often harvested and later used to obliterate the cavity once the resection has been completed .
Transotic and transcochlear approaches
The transotic and transcochlear approaches, described by Fisch and House , respectively, were introduced to provide more anterior cerebellopontine angle exposure. These approaches and their variations allow for substantial exposure of the prepontine cistern and its contents, including the pons, medulla, basilar artery, vertebrobasilar junction, cranial nerves V through XI, and the clivus . The transcochlear approach is an extension of the translabyrinthine approach but includes removal of the entire otic capsule and posterior rerouting of the facial nerve from the porous acousticus to the stylomastoid foramen. The originally described transcochlear approach preserves the middle ear and external auditory canal, whereas the extended version requires removal of these structures with obliteration of the eustachian tube and over closure of the external auditory meatus . The transotic approach was introduced to remove small cerebellopontine angle tumors and decrease the risk of CSF leak. This approach preserves the bone overlying the sigmoid sinus and requires removal of the external auditory canal with obliteration of the eustachian tube. The facial nerve is left in situ, and the external auditory meatus is overclosured to provide a water-tight seal . The primary disadvantages of these approaches are hearing sacrifice and the potential for permanent facial nerve weakness in cases in which the nerve is mobilized. For complete facial nerve mobilization, additional morbidity includes sectioning of chorda tympani and greater superficial petrosal nerves .
Lesions of the petrous apex
Inflammatory/cystic
Cholesterol granuloma
Cholesterol granuloma is the most common abnormality found within the petrous apex. It is a cystic lesion that was first recognized as a distinct clinical entity in the early 1980s . Together with mucocele and cholesteatoma, cholesterol granuloma accounts for more than 90% of the lesions of the petrous apex. Cholesterol granuloma is an intraosseous cyst filled with dark, viscous, chocolate brown fluid and granulation tissue. Birefringent cholesterol crystals can be seen on microscopy. The cyst is often contained within a fairly thick fibrous capsule but has no true epithelial lining. (Consequently, complete surgical excision is not required.) Lo and colleagues estimated that cholesterol granulomas of petrous apex occur in approximately 0.6 per 1 million individuals. Cholesterol granulomas have been recognized in the middle ear and mastoid for many decades and have traditionally been described as “blue dome eardrum” or “blue dome cyst.” They are seen occasionally in individuals with chronic middle ear or mastoid disease. They can occur anywhere within the pneumatized temporal bone .
Traditional pathophysiology proposes that the cysts form in response to anaerobic catabolism of blood and blood products. Specifically, these cysts are believed to arise as an inflammatory reaction to cholesterol crystals released from blood breakdown products. Several histopathologic studies have verified that blood breakdown products can incite an inflammatory response .
The traditionally accepted hypothesis is that blood enters the mucosa-lined pneumatic air cell tracts of the temporal bone as a result of negative pressure, which arises either as a consequence of eustachian tube dysfunction or because mucosal edema has obstructed the passage of air through the air cell system. Negative pressure within these mucosa-lined air cells then results in transudative hemorrhage. Anaerobic breakdown of the transudated red blood cells frees cholesterol crystals. A foreign body giant cell reaction and cyst formation then develops in response to irritation produced by these cholesterol crystals.
Jackler and Cho raised cogent objections to this conventional hypothesis and noted the following points:
- 1.
Transudative hemorrhage rarely follows as a result of long-term eustachian tube dysfunction. Negative pressure generated as a consequence of obstruction of air flow through the mastoid air cell tract system does not seem to be sufficient to produce hemorrhage and bleeding, even when it is sufficient (over time) to produce significant tympanic membrane retraction.
- 2.
Cholesterol granuloma occurs only in well-pneumatized temporal bones. Extensive pneumatization is usually associated with a patent eustachian tube and unrestricted movement of air through the air cells tracts. Extensively pneumatized temporal bones are only uncommonly associated with chronic middle ear or mastoid disease.
- 3.
Once air cells have been filled with effusion (bloody or otherwise), the pressure should be equalized. The process should then stop. No additional bleeding should occur. Jackler and Cho stated several arguments that a single episode of bleeding would be insufficient to produce an expanding cholesterol granuloma.
Jackler and Cho proposed an alternative mechanism. They suggested that cholesterol granuloma results as a consequence of dehiscence of the bony partition between the petrous apex air cell system and bone marrow in the anterior temporal bone or clivus. Exposed marrow is a potential source for repeated hemorrhage. Their argument is supported by a radiologic investigation that demonstrates dehiscence between bone marrow in the petrous air cell system contralateral to a cholesterol granuloma in 6 of 13 patients. No control patients with highly pneumatized petrous apices—but without cholesterol granuloma formation—had such dehiscences.
Extensive pneumatization of the petrous apex is variously reported as occurring in somewhere between 10% and 30% of patients; thus only a limited segment of the population is potentially vulnerable to development of a petrous apex cholesterol granuloma .
Brackmann and Toh listed the signs and symptoms present in individuals at the time they seek help for cholesterol granulomas: 65% of patients had hearing loss or one of its associated symptoms (tinnitus, aural fullness). More than 50% of individuals reported dizziness. Headache occurred in one third of patients. One of five patients had either facial twitching or facial numbness. Facial weakness and diplopia were uncommon.
Unfortunately, Brackmann and Toh do not indicate the reason for which individuals sought care or accepted surgery for the removal of their cholesterol granulomas. Given the frequency of hearing loss in the population, it is likely that hearing loss was present incidentally and not as a consequence of the petrous apex abnormality in at least some subjects.
Hughes and colleagues indicated that most patients seeking intervention for petrous apex cholesterol granuloma do so because of headache. The pathognomonic headache for petrous apex cholesterol granuloma is retro-orbital, although generalized temporoparietal headache may occur as a consequence of irritation of the petrous apex.
Care should be taken to establish the petrous apex lesion as the cause of the headache. Headaches are common, and an effort should be made to determine whether the headache is related to the petrous apex cholesterol granuloma. A neurology consultation or migraine management is often helpful in determining the relationship of the lesion to the symptom.
Facial twitching is much more common than facial weakness and occurs in one fifth of patients with cholesterol granuloma of the petrous apex. Facial numbness and paresthesia (usually in the distribution of V3) also occurs in approximately one out of five patients and is easier to link to the pathologic process . It is often difficult to determine whether the cystic petrous apex lesion is causing the patient’s symptoms. If the symptoms are consistent with the anatomic location of the lesion, however (ie, neurosensory hearing loss is present and the lesion clearly encroaches on the otic capsule or internal auditory canal), then treatment should be initiated. Conversely, if the patient complains of facial paresthesia but the cholesterol granuloma is restricted to the interior/posterior petrous air cells, it is probably prudent to observe the lesion.
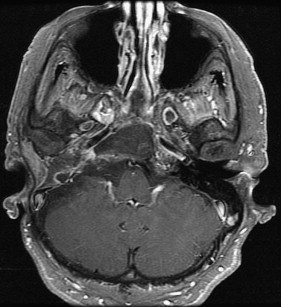
Diagnosis depends on imaging. Cholesterol granulomas are relatively unique in that they show a hyperintense signal on T1 and T2 images on MRI ( Figs. 1 and 2 ). Most of the other lesions confused with cholesterol granuloma (eg, cholesteatoma, fluid, mucocele, neoplasia) demonstrate only low or medium signal intensity on T1 images. The exception is asymmetric pneumatization of the petrous apex . Bone marrow in the nonpneumatized apex may suggest the presence of a lesion. Bone marrow can have a high signal intensity on T1- and T2-weighted images, but it is usually lower on T2-weighted images, which is sufficient to distinguish it from a granuloma on MRI . Cholesterol granulomas do not enhance with contrast, and contrast enhancement suggests a neoplasm.


The decision to operate on cholesterol granulomas of the petrous apex is often made only after determining that the lesion shows evidence of bone erosion or expansion or both. Consequently, fine-cut CT of the temporal bone is usually more useful in assessing and following these lesions than is MRI.
The first thing one should look for on a CT is the presence of normal septation of the air cell system in the petrous apex. If the lesion is not eroding and destroying these thin delicate septae, it is unlikely that it is growing or expanding. The presence of intact septation suggests that the lesion is not causing symptoms and can be “left alone.” Lesions that show normal septation rarely require intervention. There are some exceptions, however, as discussed in the section on petrous effusion.
Signs of erosion and expansion include scalloping and notching of the lesion into the clivus and posterior expansion into the labyrinth or internal auditory canal. Large cholesterol granulomas frequently bulge medially into the posterior fossa. They usually carry with them a rim of sclerotic bone that is often thin but detectable on CT. Cholesterol granulomas do not generally enhance with intravenous contrast, although some rim enhancement is consistent with a cholesterol granuloma.
If it is decided that intervention is necessary, several surgical approaches are available to remove lesions of the petrous apex ( Box 1 ). If serviceable hearing is present, every attempt should be made to conserve it; several surgical procedures can do so. The infralabyrinthine approach has been widely used as a hearing conservation technique. It is relatively quick and easy to perform and can provide dependent drainage to the cyst. Anatomic studies have shown that as much as 11 mm of space may be available using this approach, although on average approximately 5 mm is available . If the jugular bulb is high, however, access through this approach is not possible, which seems to be the case in approximately 40% to 50% of patients .
- 1.
Infracochlear
- 2.
Infralabyrinthine
- 3.
Middle fossa
- 4.
Transsphenoidal
- 5.
Transtemporal, preauricular
- 6.
Translabyrinthine
- 7.
Transcochlear
Surgical approaches to the petrous apex. First five approaches can all preserve hearing, the last two cannot.
The infracochlear approach has been championed by Brackmann and Toh. An infracochlear channel into the petrous apex cyst seems to have the highest likelihood of staying open. The approach is nondestructive and relatively straightforward. As noted by Brackmann and Toh , the infracochlear approach permits a fairly straightforward revision surgery.
The middle fossa approach permits wider exposure than the infracochlear and infralabyrinthine approach, except for the most inferior/posterior air cells. Cholesterol granulomas are often fairly extensively loculated, and it can be difficult or even impossible to break up these loculations and drain the entire cyst through the small openings afforded by the infracochlear or infralabyrinthine approaches.
The biggest disadvantage to the middle fossa approach is the lack of dependent drainage. At UT Southwestern we have used a small piece of shunt tubing placed from the petrous apex over the internal auditory canal into the mastoid air cell system to encourage aeration. Long-term postoperative aeration of the involved petrous apex has been the exception rather than the rule, however.
The endoscopic transsphenoidal approach is appealing for lesions that expand anteriorly into the sphenoid sinus itself. In such circumstances, the endoscopic transsphenoidal approach can be used successfully to drain the cyst. Brackmann and Presutti , however, indicated that long-term aeration is uncommon after endoscopic transsphenoidal procedures. If there is significant bone between the anterior margins of the petrous apex cyst and the sphenoid sinus itself, it is a difficult and potentially dangerous operation.
Neurosurgeons sometimes use the transtemporal, preauricular approach so as to completely remove cholesterol granulomas of the petrous apex but save hearing. Although such approaches seem to be successful, they seem unnecessarily invasive compared with the infracochlear and infralabyrinthine approaches .
In individuals who have lost all hearing (usually as a result of disease), translabyrinthine and transcochlear approaches provide generous access to the petrous apex and a high likelihood of persistent postoperative aeration. An experienced otologic surgeon can perform these procedures safely and relatively rapidly. Complete loss of residual hearing is inherent in these approaches. Most patients recover well from the associated loss of balance function, but these operations should be used with caution in individuals who have contralateral labyrinthine hypofunction.
Classical literature suggests that pneumatization is required to prevent recurrence. The extent to which this is true is unclear. Simple opacification of the cyst with an effusion does not necessarily indicate recurrence of the lesion; that is, nonopacified petrous apex cholesterol granulomas may remain asymptomatic indefinitely. The fact that the cystic area has filled with fluid does not necessarily mean it has become expansive or erosive. In Brackmann and Toh’s series of 21 patients who received postoperative imaging, only lesions were aerated. All lesions that were aerated had undergone infracochlear approaches. Of the 15 nonaerated lesions, only 1 had increased in size and only 5 have required revision surgery.
Epidermoid/cholesteatoma
Petrous apex epidermoid or cholesteatoma is a rare entity that comprises 4% to 9% of all petrous apex lesions . These lesions are classified as acquired or congenital, with the former being referred to as cholesteatoma and the latter referred to as epidermoid . Cholesteatoma that involves the petrous apex originates from disease in the middle ear or mastoid that gains access to the petrous apex via several preformed pathways. Epithelial cell remnants from an anomalous developing first branchial cleft or from multipotential embryonic cells or displaced otic capsule cells are thought to be the mechanism for epidermoid formation. Despite their different origins, cholesteatoma and epidermoid have an identical appearance on pathologic examination . An anatomic classification system reported by Sanna includes five categories: supralabyrinthine, infralabyrinthine, massive labyrinthine, infralabyrinthine-apical, and apical. Presenting symptoms include hearing loss, facial paresis/paralysis, dizziness, otorrhea, trigeminal paresthesia, and diplopia. In Kaylie’s series, cranial nerves V, VII, and VIII were most commonly involved. Cranial nerve deficits are thought to arise from encasement with resultant ischemia. CT often demonstrates a low-density mass that does not enhance but demonstrates smooth bone erosion. The T1- and T2-weighted MRI characteristics of petrous apex cholesteatomas are the same as CSF and arachnoid cysts ( Figs. 3 and 4 ). Unlike CSF and arachnoid cysts, fast fluid-attenuated inversion-recovery (FLAIR) and diffusion-weighted imaging reveal a hyperintense lesion with petrous cholesteatomas ( Figs. 5 and 6 ) . The presence of gadolinium enhancement should raise the suspicion of carcinoma within the lesion. The presence of a focus of squamous cell carcinoma despite a complete excision portends a poor prognosis .