This article reviews the important aspects of glomus tumor management. The biology and histology of these tumors are unique and have an impact on treatment strategies. Nonsurgical options, such as radiation therapy, are discussed. Surgical resection can be performed safely only after appropriate diagnostic testing is completed. Imaging and other diagnostic testing are explored. The various resection and reconstructive strategies are discussed.
Glomus jugulare tumors are benign tumors arising from paraganglia of neural crest origin near the jugular bulb. They grow along the planes of least resistance within the temporal bone, which leads to great variability in the extent of involvement of vital structures. The safe removal of these tumors has required great innovation and collaborative thinking among various surgical specialties. The specialty of neurotologic skull base surgery has evolved in conjunction with the development of surgical techniques for the management of glomus jugulare tumors. The current surgical philosophy has developed out of a realization that a team approach, in which neurotologists, neurosurgeons, and head and neck/reconstructive surgeons design and implement a surgical plan, is the optimal way to remove these tumors safely.
Glomus tumors are slow-growing tumors that can become extensive before they cause symptoms. Traditionally, surgical resection has been the main treatment option for glomus tumors of the lateral skull base. Radiation therapy—external beam and stereotactic radiosurgery—has been used with success . Complete resection is the ideal goal of surgical management , and this generally can be achieved. Issues that led to incomplete resection or unresectability in the past, such as cranial nerve deficits or intracranial extension (ICE), are now manageable because of improved reconstruction techniques.
This article reviews the important aspects of glomus tumor management. The biology and histology of these tumors are unique and have an impact on treatment strategies. Nonsurgical options (eg, radiation therapy) are discussed. Surgical resection can be performed safely only after appropriate diagnostic testing is completed. Imaging and other diagnostic testing are explored. The various resection and reconstructive strategies are discussed.
Tumor origin
The term “glomus” is a misnomer that was applied incorrectly before our current understanding of the origin of these tumors. The term “paraganglioma” more descriptively represents such tumors as originating from special neural crest elements, the paraganglion cells. The paraganglion cells, along with autonomic ganglion cells, form the paraganglia . The paraganglia are part of the neuroendocrine system that usually is associated with the sympathetic ganglia and consist of the adrenal medulla and extra-adrenal paraganglia . Craniocervical paraganglia are distributed along the arteries and cranial nerves of the ontogenetic gill arches. Derived from the branchiomeric system, they may be jugulotympanic, intracarotid, coronary, orbital, aorticopulmonary, pulmonary, coronary, or laryngeal. The vagal paraganglia are considered separate .
The paraganglia of the temporal bone are ovoid, lobulated bodies measuring 0.1 to 1.5 mm. On average, three paraganglia can be found in each ear, typically along the course of Jacobson’s or Arnold’s nerve. The ascending pharyngeal artery provides the primary blood supply to these paraganglia . In contrast, the intravagal paraganglia are located within the perineurium of the vagus nerve, generally within or approximating the jugular ganglion or nodose ganglion .
Paraganglia contain two types of cells: type I (also referred to as chief cells, granular cells, glomus cells, or epithelioid cells) and type II (also called sustentacular cells, satellite cells, or supporting cells). Immunohistochemically, the chief cells are reactive for neuron-specific enolase, chromogranin A, and synaptophysin, whereas type II cells are positive for S-100 and glial fibrillary acidic protein . Ultrastructurally, chief cells contain cytoplasmic granules containing catecholamines.
Grossly, paragangliomas appear as deep red-purple or brown-gray encapsulated masses with a firm, rubbery consistency. Typically, their appearance reflect their substantial vascular supply, and brisk bleeding is to be expected should one be incised. Although carotid body paragangliomas often are clearly delineated from their surrounding structures, jugulotympanic paragangliomas commonly exhibit some degree of local invasion, frequently manifesting as erosion of the temporal bone .
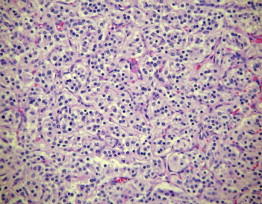
Microscopically, paragangliomas resemble adrenal pheochromocytomas ( Fig. 1 ). The tumor contains all of the cellular elements normally present in a paraganglion: chief cells, sustentacular cells, and a rich supporting vascular network. Typically, chief cells predominate—arranged in an organoid-nested pattern, known as zellballen—and the architecture may be enhanced by reticulin stain. The cells are polygonal or spindle-shaped and exhibit cuffing by sustentacular cells. A delicate capillary network also is characteristic, sometimes producing confusion with vascular neoplasms . Immunohistochemical analysis can be helpful in evaluating suspected paragangliomas, with a staining pattern similar to that of normal paraganglia. Although electron microscopy is not usually necessary for diagnosis, ultrastructural analysis of a paraganglioma reveals intracytoplasmic dense core (neuroendocrine) granules . The usefulness of fine needle aspirates for the diagnosis of paragangliomas is disputed, although some investigators demonstrated successful fine needle aspiration analysis .
The assessment of malignancy based on pathologic findings is problematic. Necrosis, nuclear pleomorphism, and vascular perineural invasion may be seen in benign tumors. Only the presence of metastasis establishes malignancy . Although most head and neck paragangliomas are considered hormonally inactive , the detection of hormone-secreting tumors is clinically significant. Morphologically, it is impossible to differentiate hormone-secreting tumors from inactive tumors; thus, the distinction must be made with specific laboratory evaluation.
Biochemistry
The chief cells of the paraganglia are one of 40 cell types classified in the diffuse neuroepithelial system and can produce neuropeptides and catecholamines Fewer than 4% of paragangliomas found in the head and neck are hormonally active such that they are considered functional . The clinical presentation and biochemical behavior of secreting tumors is variable, depending on the substance elaborated. Catecholamine elaboration, dopamine secretion, carcinoid syndrome, and paraneoplastic anemia have been reported .
The occurrence of familial and syndromic paragangliomas is well documented and is believed to account for 10% to 50% of head and neck paragangliomas . Pheochromocytoma, thyroid and visceral neoplasms, parathyroid adenoma, and multiple endocrine neoplasia syndromes are associated with paragangliomas. Additional tumors can be ipsilateral or contralateral, located at any of the branchiomeric paraganglionic stations. The most common association is glomus jugulare and carotid body tumors . Genetic testing and counseling is available, although the usefulness and role of these services have yet to be determined.
Paragangliomas rarely exhibit malignant degeneration, although several cases have been reported over the past 60 years. The reported prevalence of malignancy varies between 1% and 12%; 4% is the most commonly quoted prevalence. The rate of malignancy is greater for vagal paraganglioma (19%) . Certain familial or syndromic presentations may have substantially higher rates of malignancy . The determination of malignancy cannot be made histologically; it is made by the detection of paraganglioma tissue at a site not normally associated with the paraganglionic system. The more common metastatic sites include regional lymph nodes, skeleton, lung, and liver . A worse clinical course, greater cranial nerve deficits, and higher morbidity and mortality are found in malignant tumors; however, prolonged survival is possible with active disease .
Tumor classification
Tumor classification criteria have been reported , although none has gained universal acceptance. The criteria proposed by Fisch and Oldring and Glasscock and colleagues are among the more commonly applied. Both of these systems are relevant to surgical planning and are based on an evaluation of tumor extension with specific designation for ICE. The categorization of neuroendocrine neoplasms, including paragangliomas based on World Health Organization classification, also has been described .
Clinical diagnosis
Like all diagnoses, the history and physical examination are vital. They raise the suspicion of a glomus tumor, but the diagnosis cannot be confirmed without imaging. Pulsatile tinnitus is the most common presenting symptom of a glomus tumor . This is caused by the turbulent flow through the tumor and is seen in 76% of patients . Hearing loss is the second most common symptom, seen in 60% of patients , and usually is a conductive hearing loss because of mass effect on the ossicular chain . Sensorineural hearing loss is caused by erosion of the tumor into the labyrinth or cochlea . Pure sensorineural hearing loss is unusual, occurring in approximately 5% of patients, but mixed hearing loss is more common, occurring in 17% of patients .
Physical findings should alert the clinician to the possibility of a glomus tumor. A vascular mass in the inferior aspect of the middle ear behind an intact ear drum is the most common physical examination finding . It is important to differentiate between a glomus tympanicum tumor and a glomus jugulare tumor. The inferior border of a glomus jugulare tumor is not visible because the tumor extends into the hypotympanum and to the jugular bulb . A glomus tympanicum tumor may have 360° of its border visible . Because glomus jugulare tumors arise from the jugular bulb, lower cranial nerve symptoms may be encountered. Hoarseness is caused by vagus nerve involvement with concomitant laryngeal dysfunction; it is seen in approximately 12% of patients with glomus jugulare tumors . Dysphagia is caused by dysfunction of one or several lower cranial nerves and occurs in less than 10% of patients . Tongue weakness and shoulder weakness are the result of cranial nerve XII and XI involvement. Headache or signs of increased intracranial pressure can be seen in patients with large intracranial involvement of tumor.
Imaging
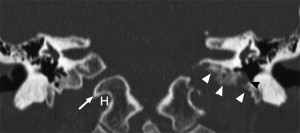
Paraganglioma, schwannoma, meningioma, and metastatic disease are the primary diagnostic considerations when a jugular foramen mass is encountered. A schwannoma usually appears as a sharply demarcated, contrast-enhancing tumor centered in a smoothly enlarged jugular foramen, with sharp, rounded bony margins. Highly vascular jugular paragangliomas usually display intense contrast enhancement, flow voids within the tumor are often visible, and bony infiltration or destruction typically is present ( Fig. 2 ). A “salt and pepper” appearance may be apparent on T1- and T2-weighted MRIs , although this is an uncommon finding. These hyper- and hypointense foci are related to slow- and fast-flowing intravascular blood and to intratumoral hemorrhage. Jugular paragangliomas produce irregular erosion of the enlarged jugular foramen margins, the earliest sign being loss of the caroticojugular spine. Thin-section CT using bone algorithm reconstruction usually allows differentiation of jugular foramen paraganglioma from schwannoma .
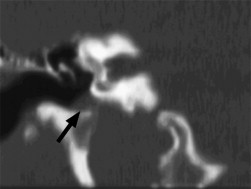
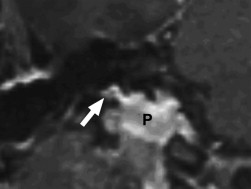
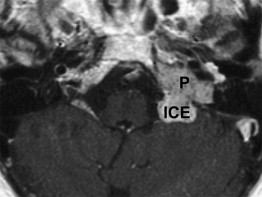
MRI is required to assess the extent of jugular paragangliomas. The coronal postcontrast T1-weighted images are inspected carefully to assess for extension of tumor into the hypotympanum (glomus jugulotympanicum tumor) ( Figs. 3 and 4 ) and to identify the inferior extent of the tumor below the jugular foramen. The distal cervical internal carotid artery flow void is identified on the axial T2-weighted images, and the extent and direction of displacement is noted. Involvement of the hypoglossal canal may be apparent clinically, but the full extent of involvement is assessed on the axial postcontrast fat-suppressed T1-weighted images. Similarly, intracranial extent (intradural and extradural) ( Fig. 5 ) is assessed on the axial postcontrast images. Larger tumors involve the carotid canal, and MRI is essential to identify petrous internal carotid artery displacement and encasement. CT and MRI are useful to determine the extent of facial nerve and otic capsule structure involvement.
Although routine MRI of the neck should cover the temporal bone, it is essential that dedicated thin-section images through the jugular foramen and petrous pyramid are obtained to adequately assess the jugular paraganglioma. The MRI examination should include axial T1-weighted images as well as axial T2-weighted images with or without fat-suppression. Coronal T1-weighted images may be useful to determine the extent of bony skull base extension with good contrast between the tumor and the T1-hyperintense fatty marrow. After intravenous gadolinium contrast, axial and coronal T1-weighted sequences are performed. Fat-suppressed postcontrast images allow for improved distinction between the brightly enhancing paragangliomas and the bony skull base–suppressed fatty marrow. Thus, CT and MRI of jugular foramen masses are considered complementary; CT is useful to assess the bony margins of the jugular foramen, and MRI allows for exquisite delineation of tumor extension. Van den Berg and colleagues are strong proponents of the time-of-flight, enhanced MR angiography technique to depict the extent of the paraganglioma and to identify additional, small paragangliomas in other locations in the head and neck. In contrast to conventional MR angiography, this technique does not necessarily show the blood supply to the tumor, but it reveals a pronounced distinction between the intensely enhancing tumor and the surrounding dark, signal-suppressed tissues. This enhanced MR angiography technique has proven invaluable to detect additional lesions ( Figs. 6–9 ) and is considered an essential MR sequence when evaluating for other glomus tumors.
Conventional angiography may be useful to assess vascularity, and preoperative embolization can be performed at the same time. Uncommonly, catheter angiography is necessary to confirm the preoperative diagnosis of paraganglioma. Blood supply is primarily from the ascending pharyngeal branch of the external carotid artery, with contribution from muscular branches of other external carotid artery vessels and the vertebral artery.
Clinical diagnosis
Like all diagnoses, the history and physical examination are vital. They raise the suspicion of a glomus tumor, but the diagnosis cannot be confirmed without imaging. Pulsatile tinnitus is the most common presenting symptom of a glomus tumor . This is caused by the turbulent flow through the tumor and is seen in 76% of patients . Hearing loss is the second most common symptom, seen in 60% of patients , and usually is a conductive hearing loss because of mass effect on the ossicular chain . Sensorineural hearing loss is caused by erosion of the tumor into the labyrinth or cochlea . Pure sensorineural hearing loss is unusual, occurring in approximately 5% of patients, but mixed hearing loss is more common, occurring in 17% of patients .
Physical findings should alert the clinician to the possibility of a glomus tumor. A vascular mass in the inferior aspect of the middle ear behind an intact ear drum is the most common physical examination finding . It is important to differentiate between a glomus tympanicum tumor and a glomus jugulare tumor. The inferior border of a glomus jugulare tumor is not visible because the tumor extends into the hypotympanum and to the jugular bulb . A glomus tympanicum tumor may have 360° of its border visible . Because glomus jugulare tumors arise from the jugular bulb, lower cranial nerve symptoms may be encountered. Hoarseness is caused by vagus nerve involvement with concomitant laryngeal dysfunction; it is seen in approximately 12% of patients with glomus jugulare tumors . Dysphagia is caused by dysfunction of one or several lower cranial nerves and occurs in less than 10% of patients . Tongue weakness and shoulder weakness are the result of cranial nerve XII and XI involvement. Headache or signs of increased intracranial pressure can be seen in patients with large intracranial involvement of tumor.
Imaging
Paraganglioma, schwannoma, meningioma, and metastatic disease are the primary diagnostic considerations when a jugular foramen mass is encountered. A schwannoma usually appears as a sharply demarcated, contrast-enhancing tumor centered in a smoothly enlarged jugular foramen, with sharp, rounded bony margins. Highly vascular jugular paragangliomas usually display intense contrast enhancement, flow voids within the tumor are often visible, and bony infiltration or destruction typically is present ( Fig. 2 ). A “salt and pepper” appearance may be apparent on T1- and T2-weighted MRIs , although this is an uncommon finding. These hyper- and hypointense foci are related to slow- and fast-flowing intravascular blood and to intratumoral hemorrhage. Jugular paragangliomas produce irregular erosion of the enlarged jugular foramen margins, the earliest sign being loss of the caroticojugular spine. Thin-section CT using bone algorithm reconstruction usually allows differentiation of jugular foramen paraganglioma from schwannoma .
MRI is required to assess the extent of jugular paragangliomas. The coronal postcontrast T1-weighted images are inspected carefully to assess for extension of tumor into the hypotympanum (glomus jugulotympanicum tumor) ( Figs. 3 and 4 ) and to identify the inferior extent of the tumor below the jugular foramen. The distal cervical internal carotid artery flow void is identified on the axial T2-weighted images, and the extent and direction of displacement is noted. Involvement of the hypoglossal canal may be apparent clinically, but the full extent of involvement is assessed on the axial postcontrast fat-suppressed T1-weighted images. Similarly, intracranial extent (intradural and extradural) ( Fig. 5 ) is assessed on the axial postcontrast images. Larger tumors involve the carotid canal, and MRI is essential to identify petrous internal carotid artery displacement and encasement. CT and MRI are useful to determine the extent of facial nerve and otic capsule structure involvement.



