Neurotologic and skull base surgery involves working around important neurovascular and neurotologic structures and can incur unwarranted complications. Knowledge of surgical anatomy, good preoperative planning, intraoperative monitoring, and excellent microsurgical technique contribute to minimizing and avoiding complications. In the event of a complication, however, the neurotologic surgeon should be prepared to manage it. In this article, the authors focus on the management of complications encountered in neurotologic skull base surgery, including hemorrhage, stroke, cerebrospinal fluid leak, extraocular motility deficits, facial paralysis, hearing loss, dizziness, lower cranial nerve palsies, and postoperative headache.
Neurotologic and skull base surgery involves working around important neurovascular and neurotologic structures and can incur unwarranted complications. Knowledge of surgical anatomy, good preoperative planning, intraoperative monitoring, and excellent microsurgical technique contribute to minimizing and avoiding complications. In the event of a complication, however, the neurotologic surgeon should be prepared to manage it. In this article, the authors focus on the management of complications encountered in neurotologic skull base surgery, including hemorrhage, stroke, cerebrospinal fluid leak, extraocular motility deficits, facial paralysis, hearing loss, dizziness, lower cranial nerve palsies, and postoperative headache.
Vascular complications: hemorrhage and stroke
Vascular complications can be devastating and possibly life threatening in neurotologic skull base surgery . Neurotologic lesions and skull base approaches to access them often require work in and around important vascular structures, such as the petrous segment and cavernous segment of the internal carotid artery, vertebral artery, basilar artery, transverse and sigmoid sinuses, superior petrosal and inferior petrosal sinuses, jugular bulb and vein . To avoid vascular complications at the time of surgery, it is important to determine the relationship of the lesion to the neighboring vascular structures with careful study of preoperative images on CT and MRI. For example, a petrous apex lesion could displace or encase the petrous internal carotid artery ( Fig. 1 ).
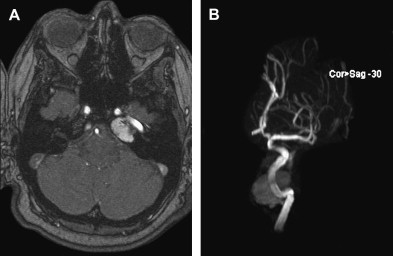
In some instances, a formal vascular study, such as an MR angiogram, MR venogram, or conventional catheter angiogram, may be required to study the vascular supply of tumors to determine patterns of venous drainage and dominance of the vertebral artery and venous sinuses. Preoperative embolization may be necessary for some vascular tumors, such as meningiomas or glomus jugulare tumors. A balloon test occlusion of the internal carotid artery or vertebral artery provides useful information if the vessels are intimately involved or encased by tumor . If inadvertent injury to the vessel is encountered, the vessel can be occluded during surgery if the test occlusion is tolerated. Planned sacrifice of the vessel with the tumor resection can be performed with or without revascularization and depends on the balloon occlusion results .
If a vascular complication is encountered, the neurotologic surgeon should be prepared to manage it. Intraoperative hemorrhage can arise from violation of an artery or vein. Venous bleeding can be controlled with gentle pressure with a hemostatic agent, such as Gelfoam soaked in thrombin followed by coverage with a cottonoid patty. Alternatively, Surgicel or Surgicel fibrillar can be used as the hemostatic agent, which works particularly well for venous bleeding from the cavernous sinus or from a small rent in the transverse or sigmoid sinus. If there is a large tear in the venous sinus, primary repair with a 5-0 prolene suture may be necessary. To avoid a venous infarct, it is critical to preserve and not coagulate important draining veins, such as the vein of Labbé. Small arterial bleeding can be coagulated with a bipolar cautery; however, if bleeding arises from a small branch off a major vessel or from an eloquent portion of brain, gentle pressure with Gelfoam or Surgicel followed by a cottonoid patty is recommended. With time this usually stops the bleeding. Injury to a major artery, such as the internal carotid artery or posterior inferior cerebellar artery, may require direct repair with a suture. In the case of a vascular occlusion, sacrifice with an aneurysm clip may be necessary, although it may result in an ischemic stroke. It is important that preoperative balloon test occlusion studies be performed beforehand. The surgeon should be prepared for cerebral revascularization if necessary.
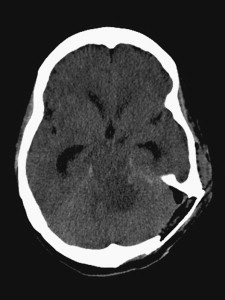
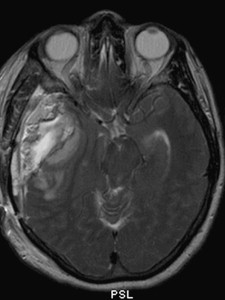
Postoperative stroke can arise from arterial occlusion (embolic or thrombotic) or venous occlusion (venous infarct). Arterial strokes usually present as sudden postoperative neurologic deficits, whereas venous infarcts present more insidiously as seizures, altered mental status, cerebral edema, and intracerebral hemorrhage . After a stroke is encountered, the patient is medically managed with hypertonic saline and hyperosmotic agents (mannitol) to prevent cerebral edema and high intracranial pressures. Anticonvulsants should be initiated if the patient exhibits seizure activity. If the patient has altered mental status, intubation for airway protection and mechanical ventilatory support should be considered, which allows controlled hyperventilation, keeps Pa co 2 down (32 mm Hg to 35 mm Hg), and minimizes cerebral edema. Temporary sedation and paralytic agents may be required in the initial recovery period in severe cases of cerebral edema. In some cases of generalized cerebral edema or acute hydrocephalus, a ventriculostomy may be required to monitor and relieve intracranial pressure by draining cerebrospinal fluid (CSF). Cerebellar edema after cerebellopontine angle surgery sometimes can cause acute hydrocephalus by occluding the fourth ventricle, which warrants a ventriculostomy ( Fig. 2 ). Postoperative edema also can arise from external compression and occlusion of the sigmoid sinus as a result of excessive fat packing at the time of closure. Excessive fat packing also can cause mass effect, particularly on the temporal lobe in middle fossa operations ( Fig. 3 ). A re-exploration for reduction of fat packing may be required in these instances.
We routinely obtain an immediate postoperative head CT after a craniotomy to rule out the presence of intracranial hemorrhage. A large compressive epidural or subdural hematoma that results in mass effect and neurologic compromise requires immediate evacuation of the hematoma. Careful inspection to remove the source of hemorrhage is necessary for adequate hemostasis. An intracerebral hemorrhage may occur at the site of the tumor resection or from a venous infarct. If there is no mass effect, they can be managed medically with close observation and serial imaging. If there is significant mass effect and impending cerebral herniation, however, surgical evacuation of the hematoma is warranted.
Cerebrospinal fluid leak
CSF leakage is the most commonly reported complication after a neurotologic procedure. The overall incidence of a CSF leak after surgical removal of an acoustic neuroma (translabyrinthine, retrosigmoid, and middle fossa approaches) has been reported to be between 11% and 12% . The biggest concern for an ongoing CSF leak is the risk of developing meningitis. Otorrhea manifests when there is violation of the arachnoid, dura, bone, and mucosal lining of the mastoid and middle ear, and CSF communicates through a defect in the external auditory canal or tympanic membrane. CSF also can travel from the middle ear through the eustachian tube to present as rhinorrhea .
CSF leakage can be continuous or can be elicited with a Valsalva maneuver while the patient is leaning forward with the nose pointing down. Some leaks may be intermittent and not always reproducible at the bedside. The presence of a halo sign on the bed sheets should raise suspicion of a CSF leak. The sample can be tested for β-2 transferrin, a highly specific and sensitive CSF indicator . If the leak presents during the early postoperative period, the dural defect is easily localized to the surgical site. If a leak occurs years after mastoid surgery, however, a meningoencephalocele or encephalocele should be suspected, and further evaluation is warranted. Diagnostic modalities, such as CT cisternography, radionuclide cisternography, and intrathecal fluorescein, may be performed to help localize the skull base defect and site of the leak.
The risk of developing a postoperative CSF leak is best minimized at the time of closure during the initial surgery . Meticulous wound closure, a watertight dural closure, and reconstruction with well-vascularized tissues significantly influence the incidence of postoperative CSF leakage. If a primary dural closure cannot be achieved, a dural patch (autologous fascia graft or dural substitute allograft) can be sewn into the dural defect. In some approaches, such as the middle fossa or translabyrinthine approach, the dural defect is best filled in with an autologous fat graft. We routinely augment our dural closures with a dural sealant, such as Tisseal (Baxter International, Deerfield, Illinois) fibrin glue or DuraSeal (Confluent Surgical, Inc., Waltham, Massachusetts). A monolayer of Surgicel is placed onto the dural closure before applying the dural sealant to allow a matrix for the sealant to adhere to. Care should be taken to avoid applying too much dural sealant, particularly DuraSeal, because it can create an epidural mass effect on the brain, especially in the temporal lobe for middle fossa approaches. DuraSeal sealant gel can swell up to 50% of its size in any dimension and cause neural compression.
The middle ear cavity also should be occluded. In translabyrinthine approaches, we generally use a piece of autologous muscle to occlude the aditus followed by more autologous fat in the mastoid defect. In retrosigmoid transmeatal approaches, we wax off the sides of the porous acousticus that has been drilled away and place a small piece of fat to fill the porous defect. Care is taken to not place too much fat and avoid facial nerve compression. Exposed mastoid air cells, such as those in the lateral aspect of a retrosigmoid craniotomy or those in the inferior aspect of a middle fossa craniotomy, are also filled with bone wax during closure. Meticulous closure of the muscle and fascial layers in the soft tissue provides additional closure over the skull to prevent pseudomeningocele formation. Excellent skin closure is necessary to prevent fluid leaking through the skin. If healthy vascularized tissue is not available, then coverage with a free tissue transfer should be considered .
In most skull base operations, we generally use an intraoperative lumbar drain for brain relaxation. The lumbar drain is left in place after surgery for approximately 3 days to promote healing at the dural closure site, especially if a watertight dural closure was not achieved. Lumbar drainage should be avoided or minimized if there is supratentorial mass effect from brain retraction edema. Care is taken to avoid overdrainage of CSF because it can result in symptomatic intracranial hypotension and life-threatening downward herniation. Patients with excessive lumbar drainage usually present with low-pressure headaches, which can progress to a decline in mental status, obtundation, and dilated, nonreactive pupils. In cases of severe intracranial hypotension, the lumbar drain should be clamped immediately and the patient should be placed in the Trendelenburg position. Slow infusion of sterile preservative-free saline (approximately 30 mL over 10 minutes) back into the lumbar drain can immediately reverse the neurologic deficit.
If a patient continues to have a persistent CSF leak despite an initial trial of lumbar drainage and there is any concern regarding the quality of the dural closure, a wound re-exploration with secondary reconstruction should be considered. Obliteration of the middle ear, eustachian tube, external auditory canal, or blind sac closure may be necessary . Re-exploration is usually needed if leakage onset is delayed. Temporal tegmen defects may require further reconstruction with fascial grafting followed by autologous bone grafting and resurfacing with calcium phosphate bone cement. In cases of refractory CSF leaks, occult hydrocephalus or idiopathic intracranial hypertension (pseudotumor cerebri) should be ruled out, and CSF diversion with ventriculoperitoneal or lumboperitoneal shunting should be strongly considered.
In our experience, we prefer placing a lumboperitoneal shunt if there is absence of hydrocephalus . This procedure avoids the risks of ventricular catheterization, including intracranial hematoma and ventriculitis. We also use lumboperitoneal shunts to treat pseudomeningoceles in patients who have undergone skull base approaches in which dural repair is difficult or not feasible. In cases of overdrainage headaches, the shunt is either ligated (with a suture or clip) or removed. If the CSF leak has resolved, no further shunting is required. If further shunting is required, we typically place a ventriculoperitoneal shunt with a programmable valve. Placement of the ventricular catheter with stereotactic guidance may be needed in patients with small ventricles.
Cerebrospinal fluid leak
CSF leakage is the most commonly reported complication after a neurotologic procedure. The overall incidence of a CSF leak after surgical removal of an acoustic neuroma (translabyrinthine, retrosigmoid, and middle fossa approaches) has been reported to be between 11% and 12% . The biggest concern for an ongoing CSF leak is the risk of developing meningitis. Otorrhea manifests when there is violation of the arachnoid, dura, bone, and mucosal lining of the mastoid and middle ear, and CSF communicates through a defect in the external auditory canal or tympanic membrane. CSF also can travel from the middle ear through the eustachian tube to present as rhinorrhea .
CSF leakage can be continuous or can be elicited with a Valsalva maneuver while the patient is leaning forward with the nose pointing down. Some leaks may be intermittent and not always reproducible at the bedside. The presence of a halo sign on the bed sheets should raise suspicion of a CSF leak. The sample can be tested for β-2 transferrin, a highly specific and sensitive CSF indicator . If the leak presents during the early postoperative period, the dural defect is easily localized to the surgical site. If a leak occurs years after mastoid surgery, however, a meningoencephalocele or encephalocele should be suspected, and further evaluation is warranted. Diagnostic modalities, such as CT cisternography, radionuclide cisternography, and intrathecal fluorescein, may be performed to help localize the skull base defect and site of the leak.
The risk of developing a postoperative CSF leak is best minimized at the time of closure during the initial surgery . Meticulous wound closure, a watertight dural closure, and reconstruction with well-vascularized tissues significantly influence the incidence of postoperative CSF leakage. If a primary dural closure cannot be achieved, a dural patch (autologous fascia graft or dural substitute allograft) can be sewn into the dural defect. In some approaches, such as the middle fossa or translabyrinthine approach, the dural defect is best filled in with an autologous fat graft. We routinely augment our dural closures with a dural sealant, such as Tisseal (Baxter International, Deerfield, Illinois) fibrin glue or DuraSeal (Confluent Surgical, Inc., Waltham, Massachusetts). A monolayer of Surgicel is placed onto the dural closure before applying the dural sealant to allow a matrix for the sealant to adhere to. Care should be taken to avoid applying too much dural sealant, particularly DuraSeal, because it can create an epidural mass effect on the brain, especially in the temporal lobe for middle fossa approaches. DuraSeal sealant gel can swell up to 50% of its size in any dimension and cause neural compression.
The middle ear cavity also should be occluded. In translabyrinthine approaches, we generally use a piece of autologous muscle to occlude the aditus followed by more autologous fat in the mastoid defect. In retrosigmoid transmeatal approaches, we wax off the sides of the porous acousticus that has been drilled away and place a small piece of fat to fill the porous defect. Care is taken to not place too much fat and avoid facial nerve compression. Exposed mastoid air cells, such as those in the lateral aspect of a retrosigmoid craniotomy or those in the inferior aspect of a middle fossa craniotomy, are also filled with bone wax during closure. Meticulous closure of the muscle and fascial layers in the soft tissue provides additional closure over the skull to prevent pseudomeningocele formation. Excellent skin closure is necessary to prevent fluid leaking through the skin. If healthy vascularized tissue is not available, then coverage with a free tissue transfer should be considered .
In most skull base operations, we generally use an intraoperative lumbar drain for brain relaxation. The lumbar drain is left in place after surgery for approximately 3 days to promote healing at the dural closure site, especially if a watertight dural closure was not achieved. Lumbar drainage should be avoided or minimized if there is supratentorial mass effect from brain retraction edema. Care is taken to avoid overdrainage of CSF because it can result in symptomatic intracranial hypotension and life-threatening downward herniation. Patients with excessive lumbar drainage usually present with low-pressure headaches, which can progress to a decline in mental status, obtundation, and dilated, nonreactive pupils. In cases of severe intracranial hypotension, the lumbar drain should be clamped immediately and the patient should be placed in the Trendelenburg position. Slow infusion of sterile preservative-free saline (approximately 30 mL over 10 minutes) back into the lumbar drain can immediately reverse the neurologic deficit.
If a patient continues to have a persistent CSF leak despite an initial trial of lumbar drainage and there is any concern regarding the quality of the dural closure, a wound re-exploration with secondary reconstruction should be considered. Obliteration of the middle ear, eustachian tube, external auditory canal, or blind sac closure may be necessary . Re-exploration is usually needed if leakage onset is delayed. Temporal tegmen defects may require further reconstruction with fascial grafting followed by autologous bone grafting and resurfacing with calcium phosphate bone cement. In cases of refractory CSF leaks, occult hydrocephalus or idiopathic intracranial hypertension (pseudotumor cerebri) should be ruled out, and CSF diversion with ventriculoperitoneal or lumboperitoneal shunting should be strongly considered.
In our experience, we prefer placing a lumboperitoneal shunt if there is absence of hydrocephalus . This procedure avoids the risks of ventricular catheterization, including intracranial hematoma and ventriculitis. We also use lumboperitoneal shunts to treat pseudomeningoceles in patients who have undergone skull base approaches in which dural repair is difficult or not feasible. In cases of overdrainage headaches, the shunt is either ligated (with a suture or clip) or removed. If the CSF leak has resolved, no further shunting is required. If further shunting is required, we typically place a ventriculoperitoneal shunt with a programmable valve. Placement of the ventricular catheter with stereotactic guidance may be needed in patients with small ventricles.
Extraocular motility deficits
Surgery of lesions that involve the cavernous sinus and petroclival region can risk postoperative palsies to cranial nerves III, IV, and VI and result in extraocular motility deficits, mainly as binocular diplopia. Surgery of lesions in the cerebellopontine angle poses the risk of injury to cranial nerve VI. Patients who have binocular diplopia complain of seeing double when both eyes are open, but occlusion of either eye resolves their diplopia . These cranial nerve palsies are usually transient if the nerves are anatomically intact and resolve within several months to a year. For adult patients with binocular diplopia, an eye patch, occlusive lens, special glasses, or prisms (Fresnel) may be used to correct the double vision. In patients with persistent binocular diplopia, strabismus surgery can be considered to restore single binocular vision in the functional positions of gaze .
Facial nerve paralysis
Facial nerve paralysis is one of the most disfiguring and noticeable complications after neurotologic surgery, and it can be psychologically and physically traumatizing to patients . A weakened orbicularis oculi muscle prevents eye closure and can increase the risk of ocular complications, such as corneal damage and visual loss, if not properly managed. Facial paralysis also can impair speech and chewing because of weakness of the orbicularis oris and buccinators muscles. The goals of managing facial paralysis should include protection of the cornea and avoidance of ocular complications and restoration of symmetry, form, and function. Facial paralysis after a neurotologic skull base procedure in which the nerve remains intact should resolve and have relatively normal function after recovery. It may take up to 1 year for natural functional recovery. Physical therapy with electrical stimulation of the face and biofeedback exercises is often helpful in maximizing function during the recovery period .
In patients with lagophthalmos and during the time of facial nerve rehabilitation, care should be taken to protect the eye. Initial medical therapy to protect the cornea includes artificial tears, lubricating ointments, taping the eye shut, and protective moisture chambers, such as eye goggles . These techniques depend on patient compliance and can be effective if the duration of facial paralysis is expected to be short-term. For debilitated patients who are unable to comply with conservative measures, a tarsorrhaphy may be considered. It is aesthetically unappealing, however, and limits peripheral vision.
If delay of facial nerve recovery is expected, early implantation of a gold weight into the upper eyelid is a good option to facilitate lid closure and corneal protection for patients with paralytic lagophthalmos . This procedure is well tolerated and offers excellent eye closure and reduced reliance on eye ointments. Because the gold weight depends on gravity, the mechanical advantage is diminished when the patient is asleep in the supine position. The major contraindication for gold weight implantation is corneal anesthesia. An alternative to the gold weight is the palpebral spring, in which a wire spring is implanted in the upper lid. When the levator muscle relaxes as the opposite eye closes, the spring actively pushes the lid down and closes the affected eye.
Lower lid laxity and malposition may be encountered in patients with paralysis of the orbicularis, resulting in further corneal exposure and chronic inflammation of the conjunctiva. A modified lateral canthoplasty is effective in resuspending and tightening the lower lid and can supplement upper lid surgery for complete correction of lagophthalmos .
In some cases, the facial nerve can be transected during surgery because of inadvertent injury or intended removal of a tumor arising from the facial nerve. Primary end-to-end anastomosis or cable nerve graft interposition should be performed to allow optimal recovery of function. When the proximal segment of the facial nerve is not available or suitable for anastomosis, however, a hypoglossal–facial nerve (XII-VII) anastomosis should be considered early during the initial hospitalization . This operation is contraindicated in patients who have concomitant lower cranial nerve palsies because an additional ipsilateral hypoglossal nerve palsy can exacerbate pre-existing dysphagia. Modifications of the classic XII-VII anastomosis have been described in attempts to preserve hypoglossal function by performing the anastomosis in a side-to-end fashion .
In some cases after cerebellopontine angle surgery in which the facial nerve is anatomically intact but remains paralyzed postoperatively at 12 months, a XII-VII anastomosis should be considered for facial reanimation. In our practice, we generally perform a facial electromyography at 9 months after surgery if facial paralysis persists and perform a XII-VII anastomosis by 12 months after the onset of facial paralysis. If end-stage muscle or nerve fibrosis is present, a XII-VII anastomosis is not a good option, and muscle transfers should be considered. Return of facial function usually begins 4 to 6 months after anastomosis. The region of initial reanimation activity is often noted around the lips and oral commissure, less so in the eye and forehead. Improvement in facial movement continues for up to 2 years. A successful result includes restoration of facial tone, resting symmetry, and voluntary facial expression .
If facial reanimation is not performed after 2 years of facial nerve discontinuity, neural and muscular degeneration can ensue, resulting in fibrosis, and can preclude facial nerve substitution operations such as the XII-VII anastomosis. In these situations, a temporalis muscle transfer, which provides suspension of the lower face and corner of the mouth, can be a viable option . This procedure also provides immediate restoration of facial symmetry and a balanced smile, which can be of great psychological benefit to patients. More than 90% of patients can control temporalis muscle contraction and obtain a significant degree of motion to simulate a smile . This strategy is effective for reanimation of the lower half of the face but has not been effective in facilitating eye closure .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


