Purpose
To evaluate the lenticular changes associated with congenital iridolenticular choroidal coloboma.
Design
Retrospective, observational case series.
Methods
setting : Tertiary eye care center in south India. study population : Total of 145 eyes of 98 patients. observation procedure : Medical records of all patients with the diagnosis of congenital iridolenticular choroidal coloboma between January 2011 and December 2012 were reviewed retrospectively for demographic profile, extent of coloboma, and associated lenticular changes.
Results
Median age of patients at the time of initial visit was 23 years (interquartile range, 13–38 years). The male-to-female ratio was ∼ 1:1. Forty-eight percent had bilateral involvement. Lens showed cataract changes in 68 eyes (48.9%). The most common type of cataract was nuclear sclerosis, which was noted in 51% of cases. A distinct type of cataract, called “coloboma cataract” (characterized by linear opacity in the region of the coloboma), was observed in 29% of cases. Other associated findings were phacodonesis in 3 eyes, dislocation in 3 eyes, and subluxation in 5 eyes. Disc and/or macular involvement in 57 eyes (39.3%) did not influence the type or density of cataract ( P > .05).
Conclusions
Congenital iridolenticular choroidal coloboma is associated with early cataractous changes. The most common type of cataract is nuclear sclerosis. The type and density of cataract do not seem to be related to the extent of the choroidal coloboma. We suggest a distinct description with the nomenclature “coloboma cataract” to be considered in the clinical grading of cataracts in patients with this condition.
Coloboma is found in 0.7 per 10 000 births and its incidence is ∼1 in 40 ocular anomalies in the Western literature. Uveal coloboma is caused by defects in the closure of the embryonic fissure of the optic cup, extending anywhere from the optic disc to the inferonasal border of the pupillary margin, between the 7 mm and 14 mm stages of development. It can occur as a result of a single gene abnormality or be part of a multisystem disorder with unknown etiology. Inheritance patterns are usually autosomal dominant in isolated cases; however, the genetic mechanism can be autosomal recessive or sporadic. Uveal coloboma can also be inherited in an X-linked fashion or be found in the context of chromosomal anomalies.
Associated ophthalmologic manifestations can include cataract, microcornea, nystagmus, optic atrophy, and retinal detachment (RD). In addition to posterior segment pathology, lenticular changes can lead to a significant visual impairment in these eyes. The literature on lenticular changes associated with iridolenticular choroidal coloboma is limited. The main purpose of this study is to evaluate and describe the lenticular changes occurring in iridolenticular choroidal coloboma. Also, we wanted to see the association of lens changes with the severity and extent of choroidal coloboma.
Materials and Methods
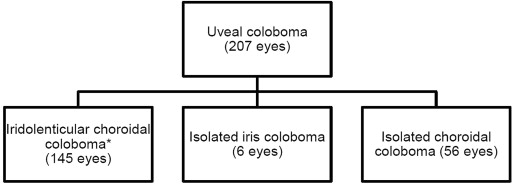
Approval from the Institutional Review Board/Ethics Committee of L V Prasad Eye Institute, Hyderabad, India was obtained for this retrospective review study and the research adhered to the tenets of the Declaration of Helsinki. This was an observational case series of 145 eyes of 98 patients with iridolenticular choroidal coloboma (combined coloboma of iris and posterior segment) seen at a tertiary eye care center in south India during a 2-year period (between January 1, 2011 and December 31, 2012). Eyes that had only iris coloboma with no involvement of posterior segment or only choroidal coloboma seen during the study period were not included ( Figure 1 ) because we wanted to make sure of the lens involvement in these eyes. As all eyes had both iris and choroidal involvement, they invariably had lens, zonular, and ciliary body involvement, which was well established from the clinical slit-lamp evaluation.
Data collected included the demographic profile, such as age at presentation and sex; ocular features such as extent of coloboma; status of lens and retina; and surgical interventions, if any. Data on the cataracts that were routinely graded according to Lens Opacities Classification System II (LOCS II ) and documented in the medical records were retrieved. Several anterior and posterior segment clinicians evaluated patients in the study group in their clinical care and comprehensive eye examination that were part of routine patient protocol. The clinicians had a universal system of documenting the lens opacity in the medical records, and each examination room in the institute is equipped with LOCS II grading charts. Although there were different ophthalmologists, all were trained to follow the same diagrammatic color-coding system, and grading was consistent. Two authors (A.M. and S.J.) reviewed and confirmed drawings and documentation of the lens findings from the medical records.
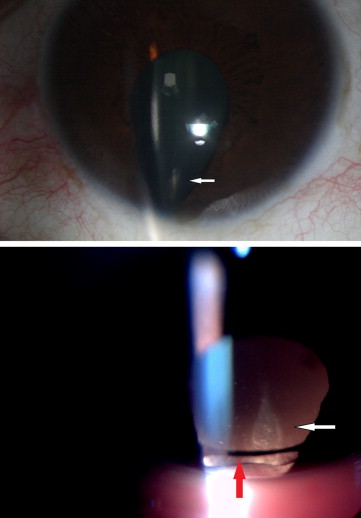
A unique “coloboma cataract” was described if there was a linear lenticular opacity overlying the coloboma area ( Figure 2 ). The linear opacity was generally seen in the nucleus, but rarely involved the anterior or the posterior cortex and was not reaching the edge of the lens. It was often close to pyramidal in shape, and not in the form of a cortical spoke. The terminology was used to describe this unique type of cataract, which is seen only in eyes with uveal coloboma. This is one of the subtypes of coloboma-associated cataract; other subtypes include presenile nuclear sclerosis, multiple cortical spokes, posterior subcapsular, traumatic, and postsurgical. As this type of cataract has not been described/defined under the LOCS II classification, we have called it “coloboma cataract.” Records were assessed for any posttraumatic cataracts, uncontrolled diabetic cataracts, or any systemic diseases associated with early-onset cataracts. None of the patients’ records had these conditions.
Data were analyzed using the statistical software Origin 7.0 (OriginLab Corporation, Northampton, Massachusetts, USA) and STATA 11.0 (StataCorp, College Station, Texas, USA). The Shapiro-Wilk test was applied to check for normality of distribution of continuous variables. Continuous parametric data were reported as mean ± standard deviation whereas continuous nonparametric data were described in terms of median and interquartile range (IQR). Group-wise comparisons were performed using an independent t test (for parametric data) and the Mann-Whitney U test (for nonparametric data). The χ 2 test was used for univariate analysis of categorical variables. A P value of less than .05 was considered statistically significant.
Results
Demographics
The median age of patients at the time of presentation was 23 years (IQR, 13–38 years; range, 3 months to 65 years). There were 53 male (54.1%) and 45 female patients (45.9%). Of the 98 patients, 47 (∼48%) had bilateral involvement. Among the 51 unilateral cases, 19 (37.3%) were right-sided and 32 (62.7%) had coloboma in the left eye. Disc and/or macular involvement by coloboma were seen in 57 eyes (39.3%), while in the rest the choroidal coloboma did not extend into the disc/macula. Nystagmus was observed in 28 patients (28.6%). RD was noted in 22 eyes (15.2%).
Cataractous Changes
Cataractous changes in the lens were noted in 68 eyes (48.9%). The median age of the patients who had cataract was 35.5 years (IQR, 22–43 years; range, 3 months to 65 years) and differed significantly from those who did not have any lens opacity ( P < .0001). The median age of those without cataract at the time of presentation was 15 years (IQR, 7–24 years; range, 3 months to 53 years). There was no significant association between presence of a cataract and disc and/or macular involvement in colobomatous eyes ( P = .97).
We observed what we defined as “coloboma cataract” in 19 eyes (29.2%). Coloboma cataract presented as an isolated entity in 15 eyes and in combination with anterior cortical (in 2 eyes) or nuclear and posterior subcapsular cataracts (in 2 eyes). Other types of cataracts observed included 8 eyes with total or white cataract and 1 eye with a dense black cataract (cataracta nigra). Three eyes had developmental nuclear cataract. Nuclear sclerosis (NS) alone was noted in 25 eyes and was seen in combination with anterior capsular cataract, coloboma cataract, cortical cataract, and posterior subcapsular cataracts (PSC) in 8 eyes. The grades of nuclear sclerosis were 1, 2, 3, and 4 in 6, 7, 8, and 9 eyes, respectively (data missing for 3 eyes). There was no significant difference in the age of patients with different grades of NS ( P = .78, ANOVA). Cortical cataract was found in 3 eyes and was associated with coloboma cataract, nuclear cataract, and posterior subcapsular cataract in 7 eyes.
Associated Lens Changes
Three eyes, 1 each associated with coloboma cataract, nuclear sclerosis, and white cataract, had phacodonesis. Three eyes had lens dislocation and 1 eye had posterior lens dislocation into vitreous clinically presenting as aphakia. Five eyes had subluxated lens, 1 eye had zonular dehiscence, and zonules were absent at the 4 o’clock position in 1 eye. Persistent pupillary membrane was present in 3 eyes and pigments were seen on the anterior capsular surface of 3 eyes.
Surgical Interventions
Ten eyes (14.7%) underwent cataract surgery (4 NS alone; 3 NS in combination with anterior capsular, cortical, and posterior subcapsular cataracts; 2 total or white cataract; 1 developmental nuclear cataract). The mean age at the time of cataract surgery was 37.7 ± 11.5 years (range, 19–51 years). Eight eyes underwent a barrier laser around the coloboma as prophylaxis and 6 eyes underwent a vitreoretinal intervention for retinal detachment. Two eyes underwent pars plana vitrectomy for lens management (dislocation in one and extreme subluxation with phacodonesis in the other).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


