Chapter 40 Lateral Neck Dissection
Technique
 Please go to expertconsult.com to view related video Lateral Neck Dissection for Differentiated Thyroid Cancer.
Please go to expertconsult.com to view related video Lateral Neck Dissection for Differentiated Thyroid Cancer.
Cervical lymphadenectomy, or neck dissection, plays an important role in the management of patients with thyroid cancer. Herein, we detail the technique for lateral cervical lymphadenectomy; the indications for neck dissection are discussed elsewhere (see Chapter 39, Lateral Neck Dissection: Indications).
Background
Historical Overview
Removal of cervical lymphadenopathy has long been recognized as an important component in the care of head and neck cancer, dating back to the early 19th century.1 Although case reports and case series for removal of isolated cervical metastases were published by von Langenbeck, Billroth, and von Volkmann in the 1870s and 1880s, Kocher advocated for resection of lymphadenopathy with a margin of normal tissue in 1880.2 The first radical neck dissection was described in 1888 by the Polish surgeon Jawdynski,2 who performed the procedure on a patient who lived for 7 years postoperatively. However, Crile is credited with popularizing the procedure in 1906 with his report comparing the outcomes of 36 patients who had undergone radical neck dissections and 96 patients who had more selective neck dissections. Of the traceable patients who had radical en bloc neck dissections, 75% were alive at 3 years compared to 19% of those who had undergone more selective operations.3
Given the significant morbidity associated with sacrificing the spinal accessory nerve, the sternocleidomastoid muscle, and the internal jugular vein, surgeons increasingly looked to minimizing functional deficits while maintaining oncologic outcome. In 1926, Bartlett and Callander reported similar recurrence rates between radical neck dissection and more conservative neck dissections that spared nonlymphatic structures in the neck.4 However, the concept of nonradical neck dissections remained controversial, with Hayes Martin strongly endorsing routine radical neck dissections for cervical metastases.5 In his 1951 manuscript, Martin declared that techniques sparing the spinal accessory nerve “should be condemned unequivocally.”5 In 1963, Suarez described the first functional neck dissection based on cervical fascial compartments,6 which was later popularized by Bocca and Pignataro.7 Ballantyne furthered the concept of a modified radical neck dissection by advocating the removal of only those lymph node groups most likely to drain the site of the primary tumor.8 More conservative lymphadenectomy paralleled the development of adjuvant therapies. Published literature has demonstrated the effectiveness of selective neck dissection in the appropriate clinical settings.9
In 1955, George Crile, Jr, reported similar outcomes for patients with thyroid malignancy undergoing either radical or conservative neck dissections.10 He emphasized that radical procedures were unnecessary for thyroid cancers, which anatomically drain primarily to the central compartment first and only secondarily to the jugular chain.11
Anatomy
The lymphatic drainage of the head and neck has been well demonstrated (Table 40-1), allowing surgeons to perform more conservative neck dissections to avoid morbidity while maintaining oncologic integrity. The thyroid gland drains primarily to the prelaryngeal, para- and pretracheal, and superior mediastinal lymph basins, which secondarily drain to the jugular lymphatic chain. These drainage patterns are so reliable that a prelaryngeal lymph node found anterior to the cricothyroid membrane is often referred to as the Delphian node. It is named for the Greek oracle, Delphi, because enlargement of this lymph node often heralds the presence of thyroid malignancy.
Table 40-1 Lymphatic Drainage Patterns by Anatomic Site16,17
| Site | Lymphatic Basins |
|---|---|
| Oral cavity | Levels I, II |
| Oropharynx | Levels II, III, IV |
| Hypopharynx | Levels II, III, IV |
| Larynx | Levels II, III, IV |
| Nasopharynx | Levels II, III, IV, V |
| Thyroid/cervical trachea | Levels VI, VII, II, III, IV |
Cervical and superior mediastinal lymph nodes are divided into seven levels that are delineated by anatomic boundaries (Table 40-2; see also Chapter 39, Lateral Neck Dissection: Indications, Figure 39-1). Level I, which is rarely involved with thyroid malignancy, includes both submental (level IA) and submandibular (level IB) lymph node groups. Level IA, which comprises the submental triangle, lies between the anterior bellies of bilateral digastric muscles, superior to the hyoid. Level IB is situated posterior to the anterior belly of the digastrics muscle, superior to the posterior belly of the digastrics muscle, and anterior to the posterior border of the submandibular gland.
Table 40-2 Cervical Lymph Node Levels
| Level | Boundaries | |
|---|---|---|
| I | Anterior: Contralateral anterior belly of the digastric muscle Superior: Mandible Posterior: Posterior border of the submandibular gland Inferior: Hyoid bone | |
| IA: Submental lymph nodes between anterior bellies of digastric muscles IB: Submandibular lymph nodes posterior to the anterior belly of the digastric muscle | ||
| II | Anterior: Posterior border of the submandibular gland Superior: Skull base Posterior: Posterior border of the sternocleidomastoid muscle Inferior: Carotid bifurcation (surgical landmark) or hyoid bone (clinical landmark) | |
| IIA: Superior to the spinal accessory nerve IIB: Inferior to the spinal accessory nerve | ||
| III | Anterior: Lateral limit of the sternohyoid muscle Superior: Carotid bifurcation (surgical landmark) or hyoid bone (clinical landmark) Posterior: Posterior border of the sternocleidomastoid muscle Inferior: Junction of the omohyoid muscle with the internal jugular vein (surgical landmark) or the inferior border of the cricoid (clinical landmark) | |
| IV | Anterior: Lateral limit of the sternohyoid muscle Superior: Junction of the omohyoid muscle with the internal jugular vein (surgical landmark) or the inferior border of the cricoid (clinical landmark) Posterior: Posterior border of the sternocleidomastoid muscle Inferior: Clavicle | |
| V | Anterior: Posterior border of the sternocleidomastoid muscle Posterior: Anterior border of the trapezius muscle Inferior: Clavicle | |
| VA: Superior to the spinal accessory nerve (surgical landmark) and the inferior border of the cricoid (clinical landmark) VB: Inferior to the spinal accessory nerve (surgical landmark) and the inferior border of the cricoid (clinical landmark) | ||
| VI | Lateral: Bilateral carotid sheaths Superior: Hyoid bone Inferior: Suprasternal notch | |
| VII | Lateral: Bilateral carotid sheaths Superior: Suprasternal notch Inferior: Brachiocephalic vein | |
Levels VI and VII constitute the central compartment, which is bounded on either side by the carotid sheath. Level VI extends from the hyoid superiorly to the suprasternal notch inferiorly. Level VII, often referred to as superior mediastinal lymph nodes, extends from the suprasternal notch superiorly to the innominate vein inferiorly.12
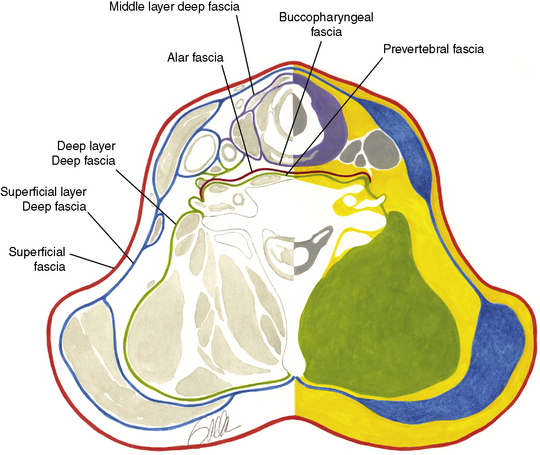
In addition to understanding cervical lymphatic anatomy, it is important to know the cervical fascial planes (Figure 40-1). The superficial cervical fascia contains subcutaneous fat and sheaths the platysma muscle. The deep cervical fascia has three layers: superficial, middle, and deep. The superficial layer of the deep cervical fascia invests the posterior belly of the omohyoid muscle and the sternocleidomastoid and trapezius muscles. The middle layer of the deep cervical fascia envelops the strap muscles (muscular subdivision) and the thyroid, larynx, trachea, and esophagus (visceral subdivision). The deep layer of the deep cervical fascia invests the deep paravertebral muscles of the neck. All three layers of the deep cervical fascia contribute to the carotid sheath.
Types of Neck Dissection
The classic or radical neck dissection description entails inclusion of the spinal accessory nerve, sternocleidomastoid muscle, and internal jugular vein with removal of levels I to V. Including an additional lymph node group or nonlymphatic structure in the resection constitutes an extended radical neck dissection. A modified radical neck dissection involves removing levels I to V while preserving one or more of the spinal accessory nerve, internal jugular vein, or sternocleidomastoid muscle (Table 40-3).
Table 40-3 Classification of Neck Dissections
| Name | Involved Structures | |
|---|---|---|
| Radical neck dissection | Sacrifices levels 1-5, CN XI, SCM, IJ | |
| Modified radical neck dissection | Radical neck dissection sparing one or more of the SCM, CN XI, or IJ | |
| Type I | Sparing CN XI | |
| Type II | Sparing CN XI and IJ | |
| Type III | Spares CN XI, IJ, and SCM | |
| Selective neck dissection | Preserves one or more lymph node levels | |
| Supraomohyoid | Levels I, II, III | |
| Lateral | Levels II, III, IV | |
| Posterolateral | Levels II, III, IV, V | |
| Central | Levels VI, VII | |
| Extended radical neck dissection | Radical neck dissection with an additional lymph node group or nonlymphatic structure in the resection | |
*SCM, sternocleidomastoid muscle; IJ, internal jugular vein; CN XI, cranial nerve XI.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


