Lasik Techniques and Qutcomes
Ioannis G. Pallikaris
George D. Kymionis
One of the fields that could characterize the last decade in ophthalmology is the evolution and advancement of refractive surgery. An important factor in the general acceptance of refractive surgery by patients and doctors was the introduction of laser in-situ keratomileusis (LASIK) (1,2). Quick visual rehabilitation, minimal postoperative discomfort, the ability to correct high degrees of ametropia, reduced risk of postoperative corneal haze, improved predictability, and stability are a few of the reasons for LASIK’s popularity over other surgical refractive correction options. It has been estimated that every year approximately 1.5 million patients worldwide undergo LASIK. This chapter describes this technique that continues to evolve.
ESSENTIAL LASER PHYSICS FOR THE REFRACTIVE SURGEONS
Excimer lasers are gas lasers that emit powerful ultraviolet pulses lasting from a few to hundreds of nanoseconds. The usual active medium is a gas mixture containing a rare gas and a halogen, which are combined to form a short-lived rare-gas halide molecule. Clinical excimer lasers use argon and fluorine gases to generate ultraviolet light with a wavelength of 193 nm. The energy from this wavelength of light is high enough to break the molecular bonds in the cornea and remove tissue. The ablation results in submicron tissue removal with every laser pulse, with minimal to no damage to the remaining tissue.
Ablation Depth
An algorithm developed by Munnerlyn et al. (3) depicts the relationship between the refractive effect produced and the depth of ablation. The Munnerlyn formula was based on affecting a theoretical lenticular curve within polymethylmethacrylate (PMMA) model, refined through in vivo models. The essentials of the Munnerlyn formula are found in the following formula:

The main principle to be drawn from the formula is that the depth of ablation increases with the square of the optical zone. A small increase in the optical zone results in a large increase in the amount of tissue ablated for any dioptric correction.
Optical Zone
An evolution of technique toward larger optical zones continues despite the resultant greater depth of ablation, increasing the risk of corneal ectasia. Larger optical zones have two primary benefits—reduced night glare and reduced regression of effect—leading to more stable high corrections.
Eye Tracking System
Active eye tracking means that the laser detects a change in the eye’s location and moves the next laser pulse in an attempt to meet the change. Passive tracking, however, simply detects change and shuts down further laser pulsing when the change exceeds a predetermined distance.
Fluence
Fluence correlates the amount of tissue that is ablated with each pulse (millijoules/sq cm). A fluence test is performed prior to each surgery and is crucial for laser beam calibration, homogeneity and alignment.
Custom Ablation
The linking of the laser device to various instruments (such as topography, wavefront analyzers) allows for correction of irregular (eccentric) ablations and high-order aberrations.
Microkeratome: A Critical Element
Microkeratome is another issue that is critical to the LASIK technique. There are several characteristics that can describe a microkeratome. Some of them are the following:
Function (automated or manual)
Cutting mechanism (blade, water or laser beam)
Oscillation rate (customizable, predetermined)
Hinge position (nasal, superior, 360-degree placement)
Disposability
Visibility of the cornea during keratectomy
Suction to create a lamellar corneal flap and ability to check the intraocular pressure (IOP) intraoperatively
Complexity, service, and cost
An important issue for each microkeratome is the cutting flap thickness. A microkeratome that tends to cut thin flaps is more likely to produce buttonholes, whereas thick flaps leave a thinner residual corneal bed, which limits the amount of ablation that can be safely performed. The average flap thickness does not predictably follow the manufacturer’s label due to instrument variability and other operative factors (preoperative corneal thickness and curvature, microkeratome oscillation rate, suction ring pressure) (4). Intraoperative pachymetry (pre- and intraoperative after the flap is lifted, to determine flap and residual corneal bed thickness after flap creation) and predicted stromal ablation (calculated from the nomograms of the laser device according to the attempted correction and optical zone size) are important factors in maximizing the safety of the procedure.
Each of these factors is important for the evaluation of a microkeratome, and, regrettably, there is no perfect microkeratome. A general rule is that the microkeratome that meets the needs of each surgeon is the best microkeratome.
PREOPERATIVE EVALUATION
Limitations and Contraindications of LASIK
Preoperative evaluation of candidate LASIK patients consists of a detailed ophthalmic examination, which includes a complete medical and ophthalmic history and an informed consent.
There are several reasons for not performing LASIK. These contraindications result from the accumulated experience with LASIK with retro- and prospective studies (5). Some of them are the following:
The upper limit of attempted correction: There are many factors that could affect the accepted upper limit for LASIK; we cannot simplify and state a single accepted attempted correction in LASIK procedures. Several factors, such as attempted correction, flap thickness, pupil diameter, pre- and intraoperative (after the flap’s creation) corneal thickness, are some of the parameters that determine the attempted correction in each patient individually. But attempted myopic corrections of more than 10 D or predicted myopic post-LASIK topographic curvature readings of less than 32 D are unacceptable (even though the previous criteria are fulfilled) due to increased risk of postoperative ectasia, induced optical aberrations, the decrease in functional optical zone, and the induced multifocality of the post-LASIK cornea. All these induced alterations result in a decrease in safety and efficacy of the LASIK procedure. Furthermore, hyperopic corrections of more than 5 D have poor results due to lost lines of best corrected visual acuity (BCVA), increased induced optical aberrations, and high incidence of regression.
Patient’s personality, occupation, psychological condition (patients with high expectations of the surgery)
Patients younger than 18 years old (or older than 50 years old especially with high ammetropies) or unstable refraction (more than 0.5 D of change over 1 year)
Previous intraocular or corneal surgery in the eye to undergo LASIK
Good uncorrected visual acuity
Corneal warping due to contact lens (CL) (soft CL must be removed 3 weeks before surgery and rigid CL at least 2 months before surgery)
Thin corneas (less than 500 μm) for myopic patients
Corneal dystrophies (ectatic-epithelial-stromal)
Active ocular infection
Pupil diameter more than 8 mm
The presence of cataract
Monocular patients
Glaucoma or glaucoma suspects
Retinal diseases (macular degeneration, myopic maculopathy, retinal tears)
Systemic diseases (diabetes mellitus, Sjögren’s syndrome, rheumatoid arthritis, and collagen vascular disorders)
Pregnancy-lactation
All these limitations are debatable and can be changed at any time as they correlate with the current status of research.
OPERATIVE TECHNIQUE
Although LASIK offers almost immediate visual correction, improved comfort and stability, and minimum wound healing complications compared to photorefractive keratectomy (PRK), it requires far more surgical skill, as it involves the use of both sophisticated and complicated microkeratome technology.
The technician and the surgeon should check the laser and the microkeratome before surgery. The surgeon should also confirm that the correct treatment data are entered
into the laser computer. Both the surgeon and the technician should verify the patient’s name, the pupil diameter (in scotopic conditions), the thickness of the central cornea, and the attempted correction.
into the laser computer. Both the surgeon and the technician should verify the patient’s name, the pupil diameter (in scotopic conditions), the thickness of the central cornea, and the attempted correction.
An eyelid speculum is inserted in the operative eye, which has been anesthetized topically, and the fellow eye is covered. The cornea is marked with an instrument that can allow postoperative proper flap alignment. A suction ring is placed on the eye to achieve an adequate IOP for the creation of the cornea flap. There are several indications that suction is adequate for flap creation, such as pupil dilatation, contact applanation device, or the patient’s decreased vision. Corneal lamellar dissection has a steep learning curve, with the potential for severe, vision-threatening complications. Newer microkeratomes have improved the safety and reliability of the procedure. After flap creation (some microkeratomes give surgeons the ability to choose the hinge position—superior, nasal, or oblique), the residual corneal bed stroma is examined for irregularities. The next steps include flap protection, intraoperative pachymetry, centration and ablation; all these steps should be done as quickly as possible to minimize the time of exposure of the stromal surface (avoiding stromal dehydration, which eventually leads to overcorrection and, in very rare conditions, to corneal perforation).
Centration of the laser beam is also crucial for a successful operation. For myopic eyes, the ablation beam is centered on the center of the pupil. It is centered slightly nasal to the corneal light reflex for hyperopic corrections.
The tracking system is activated during the beam centration. Small saccadic eye movements are acceptable, but the surgeon must stop the ablation if the eye starts drifting away from the fixation target. Once the ablation is completed, the corneal stromal bed is cleaned with a dry sponge. The flap is replaced onto the bed using a bent cannula while irrigation of the interface with balanced salt solution is performed to remove any remaining debris. This also facilitates the floating of the flap back into its original position. Aggressive irrigation should be avoided because it leads to flap edema, which increases the incidence of epithelial ingrowth (presence of an area of poor flap adherence). For proper flap alignment, the corneal marks should be properly aligned.
POSTOPERATIVE MANAGEMENT
The majority of LASIK patients require minimum postoperative follow-up and have excellent refractive results, even in the presence of minor flap complications. Severely complicated cases, however, require intensive monitoring of the eye’s status.
The main goals of postoperative management include the proper flap alignment to the stromal bed, the recognition and management of complications, and the modulation of refractive status. LASIK patients are typically examined 1 to 2 hours after the operation (to ensure that the flap is properly aligned), on the first postoperative day (if striae or other flap irregularities are evident, the flap should be lifted back and repositioned), and at 1, 3, 6, and 12 months postoperatively.
The postoperative regimen varies significantly between refractive surgeons, but in general it includes a topical combined antibiotic-steroid agent tapered for 15 days to prevent infection and control inflammation.
AVOIDANCE OF LASIK COMPLICATIONS
The widespread growth of LASIK has not resulted in notably serious complications. The few that have occurred, however, are of great importance when considering the elective nature of such a procedure and the ever-growing number of available alternatives (6, 7, 8). Among the many classifications of LASIK complications, the most popular is the one that lists complications in chronological order.
Intraoperative
Intraoperative complications include buttonholes, half flaps, irregular/thin flaps, total caps, epithelial defects, and overhydrated or dehydrated flaps (Fig. 77-1). Most, if not all, are the results of a poor surgical technique and are preventable (9). Some of the predisposing factors for improper keratectomy are extreme corneal keratometric values (corneas steeper than 46.00 D are more prone to buttonholed or centrally thinned flaps, whereas corneas flatter than 41 D are more prone to free caps), lack of synchronization between oscillatory blade and microkeratome movement,
irregular oscillation rate, poor suction, and defective microkeratome plates (7,8,10). Proper assembly of the microkeratome, marking of the cornea prior to the keratectomy, good exposure of the treated eye, customized microkeratome settings depending on the corneal keratometric readings (larger suction ring for flat corneas) as well as adequate suction during keratectomy (pressure above 80 mm Hg) are some of the details that are fundamental in order to eliminate these complications.
irregular oscillation rate, poor suction, and defective microkeratome plates (7,8,10). Proper assembly of the microkeratome, marking of the cornea prior to the keratectomy, good exposure of the treated eye, customized microkeratome settings depending on the corneal keratometric readings (larger suction ring for flat corneas) as well as adequate suction during keratectomy (pressure above 80 mm Hg) are some of the details that are fundamental in order to eliminate these complications.
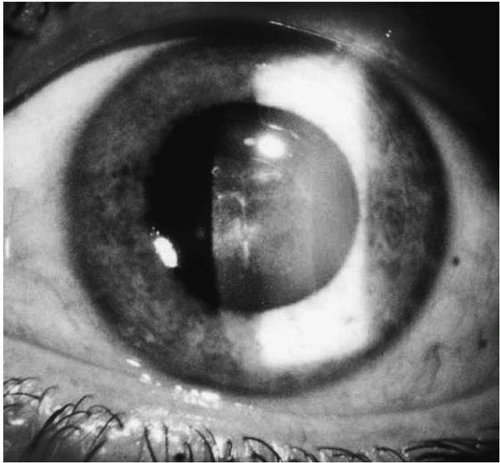 FIGURE 77-1. Slit-lamp photograph of a patient with post-LASIK buttonhole, showing a central irregular corneal scar.(see color image) |
The operation should be aborted if serious intraoperative complications occur. A new LASIK should be attempted no sooner than 3 months. This interval is necessary to allow the flap to adhere strongly to the stromal bed. A deeper depth plate should be used for reoperation (180 or 200 μm). It may be safe to complete the operation in selected cases, for example, where a total cap seems regular and of reasonable thickness.
Early Postoperative
The majority of early postoperative complications present during the first week after LASIK. We discuss those that are most common.
Flap Striae
Small irregularities of the corneal surface are almost unavoidable after LASIK. Although extremely wrinkled or dislodged flaps are very rare, flap striae may complicate even the most uneventful operation. Thinner, larger flaps and high attempted corrections are some of the predisposing factors for surface wrinkling (Fig. 77-2).
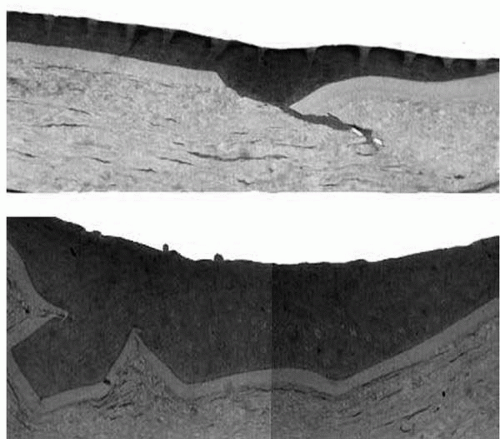 FIGURE 77-2. Histopathology of excised cornea reveals areas of epithelial ingrowth (top) and flap shrinking (bottom) (trichrome stain). |
Striae are evident as soon as the first few hours after LASIK. Insignificant striae are asymptomatic, whereas significant ones cause irregular astigmatism with optical aberrations and BCVA loss in the presence of successful refractive outcome and regular topographic ablation pattern (11). Macrofolds (full-thickness flap tenting) are visualized by slit-lamp examination, whereas microfolds (wrinkles in Bowman’s layer in the epithelial basement membrane) are visualized by retroillumination (12).
Flap striae are not a self-limiting condition. Significant striae (especially those that cross the visual axis) should be treated as soon as they are diagnosed, because with time they become embedded into the stromal bed and cause permanent damage to Bowman’s membrane, with subsequent failure of any attempt to realign the flap. Several techniques have been described for management of flap striae (10,13). A technique that has worked well is the so-called flap ironing. During this procedure, the flap is reflected back and the stromal surface is hydrated with balanced salt solution (BSS) for about 30 seconds. The flap is then floated back into position. After irrigation is completed, ironing of the flap is done using a moistened sponge, starting from the hinge and pressing toward the opposite end of the flap (painting of the flap) while stretching it perpendicular to the striae. The flap is left for 5 minutes to attach to the bed. Hypertonic saline solution, 5%, may be applied to enhance striae treatment.
Infectious Keratitis
Keratitis is extremely rare after LASIK (0.1%), as the intact epithelium acts as a barrier to invasion of micro-organisms (14,15). Conjunctival injection and moderate to severe pain that persists throughout the first postoperative day are the most common symptoms. Any corneal infiltrate associated with an epithelial defect after LASIK should be considered infective and should be treated aggressively. Patients with epithelial defects should be examined daily until reepithelialization, to detect early signs of bacterial keratitis. Proper draping of the operating eye and sterilization of the microkeratome and assisting instruments can minimize the risk of infection.
Diffuse Lamellar Keratitis (DLK)
Diffuse lamellar keratitis (a relatively infrequent complication) was first described in 1998 by Smith and Maloney (16). The reported incidence of this complication in the literature varies with the etiology and the severity of the complication from 0.2% in mild cases up to 30% in so-called epidemic DLK (17).
A classification in four stages, according to the severity and the evolution, has been described with clinical observation and confocal microscopy measurements (17, 18, 19). In stage I, granulocytes and mononuclear cells are localized at
the peripheral flap (in the interface level). In stage II there is an additional involvement of the central cornea with linear acellular spindle-shaped bodies in the interface. In stage III there are sparse infiltrates in the anterior stroma and accumulation of decayed inflammatory cells in the central portion of the interface (spindle-shaped bodies and debris in confocal microscopy observation). Finally, in stage IV there are inflammatory cells, stromal and Bowman’s folds, keratocyte activation in confocal microscopy, and flap melting, resulting in a decrease of flap thickness.
the peripheral flap (in the interface level). In stage II there is an additional involvement of the central cornea with linear acellular spindle-shaped bodies in the interface. In stage III there are sparse infiltrates in the anterior stroma and accumulation of decayed inflammatory cells in the central portion of the interface (spindle-shaped bodies and debris in confocal microscopy observation). Finally, in stage IV there are inflammatory cells, stromal and Bowman’s folds, keratocyte activation in confocal microscopy, and flap melting, resulting in a decrease of flap thickness.
The exact cause and the ideal treatment of DLK have not been determined. The possibility of infection was excluded by negative culture (20). Contaminations of the interface during LASIK from soap, disinfectants, microkeratome blade debris, topical antiinflammatory nonsteroidal (AINS) agents and anesthetics, have been described (21). Late, recurrent or traumatic epithelial defect and erosion (22,23), meibomian gland secretion, and concomitant contact dermatitis (24) have also been blamed (25).
Early recognition of DLK is essential in order to optimize the treatment effect. Linebarger et al. (17) proposed guidelines for the management of DLK in correlation with the stage of this postLASIK complication. Intense topical corticosteroids (prednisolone 1%) must be administered every hour for moderate inflammation (stages I to II). In severe cases (stages III to IV) flap lift, irrigation, and scrape-off should be added. Close follow-up every day is necessary until decrease of inflammation.
Late Postoperative
Dry Eye
A frequent postLASIK complication (up to 30% to 40%) is dry-eye symptoms, especially in patients with preexisting dry eye (26). This postLASIK complication may be due to decreased corneal sensation with subsequent decreased blinking frequency and or to damage to the keratolimbalarea goblet cells from the suction ring. Perez-Santonja et al. (27) found that corneal sensitivity returned to preoperative levels 6 months after LASIK, whereas Chuck et al. (28) reported that corneal sensation tended to return to near baseline levels 3 weeks after surgery. In addition, a statistically significant correlation with attempted correction and reduction in corneal sensation has been proved (29). Frequent use of artificial tears and/or temporary punctal plugs has proved to be effective for the time period of post-LASIK dry-eye symptoms.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


