The excimer laser revolutionized the field of refractive surgery and greatly facilitated its acceptance into mainstream ophthalmology. As techniques evolved, laser-assisted in situ keratomileusis (LASIK) replaced photorefractive keratectomy (PRK) as the procedure of choice given its lack of postoperative pain, quick visual rehabilitation, and ability to treat higher degrees of ametropia. LASIK has been shown to be a safe and efficacious technique for the correction of myopia, hyperopia, and astigmatism, but limitations exist (1, 2, 3, 4, 5, 6). These limitations have inspired surgeons to combine LASIK with other ophthalmologic procedures for the correction of both naturally occurring and postsurgical refractive error.
Combining LASIK with other technologies appeals to the refractive surgeon for several reasons. First, it may allow for the successful treatment of high myopia and astigmatism beyond what is generally considered the safe range for LASIK [approximately 10 diopters (D) of myopia and 5 D of astigmatism]. Higher levels of myopia cannot be treated with deeper excimer laser ablations because a sufficient amount of corneal stromal tissue must remain to guard against potential keratectasia and refractive instability (7,8). Current recommendations suggest a minimal residual stromal bed thickness of approximately 250 μm. This precludes the application of highly myopic ablations, especially in those patients with thinner corneas. The residual myopia remaining after a maximal LASIK treatment could be corrected by combining LASIK with another refractive procedure that does not involve the removal of stromal tissue.
In eyes with moderate to high myopia and low pachymetry values, concerns over residual stromal bed thickness and potential iatrogenic keratectasia may preclude full LASIK correction or limit retreatment options should regression occur. These patients could also benefit from a combined approach that reduced ablation depth by redistributing part of the LASIK-dependent correction to another procedure. Reports of keratectasia occurring in patients with residual stromal beds greater than 250 μm suggests that less central stromal tissue removal may be safer (9, 10, 11). Additionally, decreasing the magnitude of refractive error to be corrected by LASIK may allow for the use of larger optical zones (OZs) with a smaller chance of subjective optical disturbances.
A last theoretical advantage of combining LASIK with another procedure is adjustability. If the additional technology is reversible or adjustable, it could allow for subsequent refractive changes desired by the patient.
COMBINATION OF LASIK WITH OTHER REFRACTIVE SURGERY TECHNIQUES
Combined LASIK and Incisional Keratotomy
Incisional keratotomy refers to procedures that decrease refractive error by means of almost full-thickness corneal incisions. Their effect is a function of incision length and OZ size. Examples include radial keratotomy (RK) and astigmatic or arcuate keratotomy (AK). These techniques are uncommonly performed today given the more predictable outcomes associated with excimer laser surgery (12).
There is one published report of RK enhancements after LASIK to treat residual myopia. Damiano and colleagues (13) reported on 60 eyes of 41 patients treated with combined RK and LASIK for a preoperative spherical equivalent (SE) −8.09 ± 2.60 D (range, −4 to −15.25 D). After the initial LASIK procedure, the SE decreased to −2.02 ± 1.02 D (range, −0.50 to −5.50 D). RK was chosen over LASIK retreatment for several reasons including a residual stromal bed of less than 250 μm, insufficient stromal thickness to safely correct the myopia with LASIK alone (planned procedure), and surgeon preference in the presence of a stromal bed thick enough to safely allow a full LASIK re-treatment. RK was performed using four, six, or eight centrifugal incisions with a 3-to 6-mm OZ. AK was performed if astigmatism greater than 1 D was observed. The mean time between LASIK and RK was 7.3 ± 6.5 months. After RK, the SE decreased to −0.43 ± 0.61 D (range, −2 to +0.75 D).
There are multiple theoretical concerns when performing incisional keratotomy on a postLASIK cornea. First, multiple incisions could potentially lead to epithelial ingrowth under the LASIK flap. Second, it may be difficult to predict the patient’s response given the presence of a thinned cornea. Third, RK incisions could further weaken an already thinned cornea, resulting in iatrogenic keratectasia. Alternatively, a thinned cornea may develop pronounced flattening with a greater progressive hyperopic shift than has been observed with RK alone (14). Fourth, there may be a risk of the flap separating into fragments if the patient ever sustains corneal trauma or needs to have the flap relifted [i.e., for late diffuse lamellar keratitis (DLK)].
Damiano et al. (13) reported none of these complications after a mean follow-up time of 15.4 months. No eye lost two or more lines of best spectacle-corrected visual acuity (BSCVA), and all eyes had a BSCVA of 20/30 or better. Three patients with sufficient stromal bed thickness desired a LASIK enhancement after the RK procedure and this was performed uneventfully by lifting the original flap. All three eyes had an uncorrected visual acuity (UCVA) of 20/20 after the second LASIK treatment. Postoperative complications included mild glare and halos (23%), diurnal fluctuation (10%), and distorted vision (4%).
AK was most often used in conjunction with LASIK before the United States Food and Drug Administration (FDA) approved astigmatic excimer laser ablation corrections. Surgeons could perform AK to decrease a patient’s astigmatism, followed by LASIK several months afterward to treat the residual spherical error. Some surgeons still combine AK with LASIK for select patients. These include individuals whose astigmatism exceeds that amount for which the laser is approved to correct and those patients with larger pupils who are at risk for optical aberrations with an excimer induced elliptical OZ.
Guell and Vazquez (15) described a staged procedure combining AK and LASIK to treat high astigmatism in 15 eyes. Thirteen of the eyes had naturally occurring astigmatism and two of the eyes had surgically induced astigmatism resulting from a phacoemulsification and a penetrating keratoplasty. AK was performed initially followed by LASIK 3 to 5 months later. The preoperative mean SE and the mean refractive astigmatism were −2.47 ± 3.69 D (range, −3.25 to + 1.50 D) and −4.59 ± 1.66 D (range, −3.25 to −8 D), respectively. After both procedures, the mean cylinder power decreased to −1.21 ± 1.07 D and the mean SE measured −0.09 ± 1.50 D (12-month follow-up). One eye lost a line of best corrected visual acuity (BCVA) and two eyes gained one and two lines, respectively. No patients experienced epithelial ingrowth through the AK incision sites. No other complications occurred.
Limbal relaxing incisions (LRIs) to reduce astigmatism have also been reported in conjunction with LASIK (16). Unlike AK, LRIs are placed more peripherally near the limbus and are usually only 600 μm in depth. Their location places them outside of the lamellar corneal flap. LRIs are less effective than AK, but have the theoretical advantage of inducing less irregularity.
A role may exist for incisional keratometry after LASIK to treat topographic irregularities. Pulaski (17) reported both AK and combined AK/RK to treat asymmetrical steep islands in seven eyes after LASIK. Patients complained of poor UCVA and unwanted optical side effects. After undergoing the incisional secondary procedure, the SE decreased from −0.94 ± 0.48 D to −0.21 ± 0.12 D. Optical aberrations were reduced in all patients and the average UCVA improved from 20/40 to 20/25. Two patients experienced inferior steepening, and one microperforation occurred. No eyes lost two or more lines of BSCVA. The author suggested that this technique might be helpful in similar patients until topographically guided custom excimer laser ablations become available for the management of this problem.
The limited data available suggest that combined LASIK and AK/RK may be a safe procedure. Incisional keratotomy is an extraocular procedure (although microperforations can occur), it can be performed in an office or laser suite setting, and it does not further compromise corneal thickness. Additionally, accommodation is preserved. Disadvantages include its lack of predictability and stability, its inability to treat high myopia, the potential for flap complications, and its lack of adjustability and reversibility. We do not recommend performing RK primarily with a planned secondary LASIK treatment, given the above issues and the potential for healing problems and flap-related complications (18, 19, 20).
Combined LASIK and Phakic Intraocular Lenses
Phakic intraocular lenses (P-IOLs) are designed to correct high ametropia following surgical implantation anterior to the crystalline lens. P-IOLs may be angle fixated (e.g., Nuvita lens, Bausch & Lomb, Irvine, CA), iris fixated (e.g., Artisan lens, Ophtec B.V., Groningen, Netherlands), or located in the posterior chamber (e.g., STAAR lens, STAAR Surgical, Nidau, Switzerland). P-IOLs have been used for many years in Europe and South America. All models have undergone multiple design refinements to improve safety profiles, and several lenses are currently in FDA trials (21, 22, 23).
The practice of combining P-IOLs with LASIK is called bioptics and was first described by Zaldivar et al. (24). The concept’s inspiration was the inability of P-IOLs alone to sufficiently correct very high degrees of myopia (greater than 15 to 20 D) and astigmation. A P-IOL thickens with increasing power; so concerns about lenticular or endothelial touch limit the lens’ clinical utility. Decreasing the P-IOL OZ could mitigate this issue, but that could also result in glare or halos. The solution was bioptics—a P-IOL served to reduce the spherical error and a supplementary LASIK procedure corrected the residual sphere and astigmatism, thus extending the range of correction without compromising P-IOL OZ size (25,26).
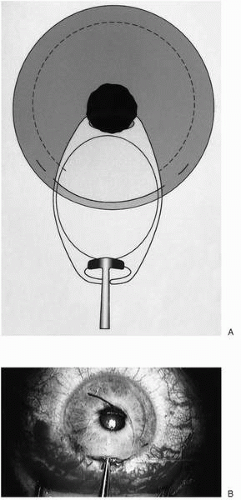
Bioptics is a two-staged surgical procedure. Topical anesthesia may be used, but a retrobulbar block may be preferred to avoid inadvertent lenticular touch with eye movement. In the first stage, a hinged lamellar corneal flap is created using a microkeratome. The flap is inspected and refloated back into position without performing a laser ablation. The surgeon next fashions a scleral tunnel or clear corneal wound, the length of which is determined by the P-IOL size and material [i.e., foldable material vs. polymethylmethacrylate (PMMA)]. The next steps are determined by the intended location of the P-IOL. If the lens is to reside in the anterior chamber, acetylcholine is injected to induce miosis. This protects the crystalline lens from inadvertent contact and allows proper centering over the pupil. The anterior chamber is then filled with a viscoelastic agent. If the lens is to lie in the posterior chamber, the pupil is dilated preoperatively and viscoelastic is injected into the anterior chamber. Once a P-IOL is inserted into the anterior chamber, it must be manipulated into the proper orientation. Paracentesis sites may be helpful to allow for additional instruments. Depending on lens design, it may be tucked under the iris into the posterior chamber or manipulated so that the footplates reside in the angle or are enclavating iris tissue. If fixated in the posterior chamber, acetylcholine is injected to induce miosis and protect against P-IOL dislocation. If not performed preoperatively, a peripheral iridectomy should be created to prevent angle-closure glaucoma. Viscoelastic is then exchanged for balanced salt solution (BSS) and the incision may be sutured closed if necessary. Figure 80-1 illustrates these steps with the Artisan P-IOL. The target SE following P-IOL placement is low to moderate myopia.
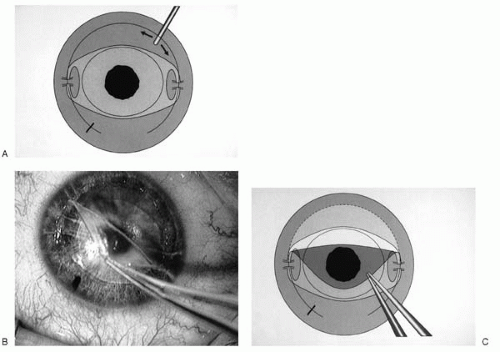
The second stage of bioptics is the excimer laser ablation, which occurs 3 to 5 months later once the refraction has stabilized and all sutures have been removed (Fig. 80-2). The flap is relifted and the laser applied to treat the remaining refractive error. The flap is then refloated back onto the stromal bed.
Some authors have deferred creation of the LASIK flap until the second stage of the procedure (24), but theoretical safety concerns suggest that the surgical steps proceed in the aforementioned order. For instance, creating the LASIK flap prior to insertion of the P-IOL may prevent potential intraocular P-IOL movement during the microkeratome pass. This theoretically avoids P-IOL, endothelial touch in the case of anterior chamber lenses and P-IOL, and lenticular contact in the case of posterior chamber lenses. It may also preclude posterior chamber lenses from dislocating during the temporary mydriasis that occurs with suction ring application. The disadvantage of creating the LASIK flap during the first stage is the need to relift the flap for the second stage, which may increase the risk of epithelial ingrowth (28).
FIGURE 80-1. A,B: The first surgical stage of bioptics. A LASIK flap is created and refloated back into position without performing a laser ablation. A phakic intraocular lens (Artisan lens shown) is introduced into the anterior chamber and centered over the pupil. (From Guell JL, Vazquez M, Gris O. Adjustable refractive surgery: 6 mm artisan lens plus laser in situ keratomileusis for the correction of high myopia. Ophthalmology 2001;108: 945-952, with permission.)
The suggested indications for bioptics include myopia greater than 15 to 18 D or myopia greater than 11 D with more than 1.50 to 2 D of astigmatism (24,29,30). A thorough preoperative examination is necessary including an evaluation of the corneal topography, corneal thickness, cycloplegic refraction, pupil size in scotopic conditions, anterior chamber depth, endothelial cell counts, and retinal periphery. Contraindications include a history of corneal irregularity (i.e., keratoconus), uveitis, glaucoma, shallow anterior chamber (for anterior chamber P-IOLs), low endothelial cell counts (<2,000 cells/mm2), cataract, anterior segment pathology, dry eye, unstable refraction, autoimmune disease, or uncontrolled systemic or eye disease.
FIGURE 80-2. A-C: The second stage of bioptics. Months later, once the sutures have been removed and the refraction has stabilized, the flap is relifted and the LASIK ablation performed. (From Guell JL, Vazquez M, Gris O. Adjustable refractive surgery: 6 mm artisan lens plus laser in situ keratomileusis for the correction of high myopia. Ophthalmology 2001;108:945-952, with permission.)
TABLE 80-1. SUMMARY OF VISUAL OUTCOMES FOLLOWING LASIK COMBINED WITH OTHER PROCEDURES