21
Laser Treatment for Diabetic Retinopathy (Clinically Significant and Diffuse Macular Edema: Fundamentals of the Early Treatment Diabetic Retinopathy Study)
Yukihiro Sato
Macular edema is the most common cause of vision loss in patients with diabetic retinopathy. There are several reports of randomized clinical trials of photocoagulation for diabetic macular edema (1–6). Among these trials, the Early Treatment Diabetic Retinopathy Study (ETDRS) (5, 6) included by far the largest number of patients. The ETDRS was designed to address three major questions in the management of patients with nonproliferative or early proliferative diabetic retinopathy:
 When in the course of diabetic retinopathy is it most effective to initiate panretinal photocoagulation?
When in the course of diabetic retinopathy is it most effective to initiate panretinal photocoagulation?
 Is photocoagulation effective in the treatment of diabetic macular edema?
Is photocoagulation effective in the treatment of diabetic macular edema?
 Is aspirin treatment effective in altering the course of diabetic retinopathy?
Is aspirin treatment effective in altering the course of diabetic retinopathy?
Because the purpose of this chapter is to clarify the efficacy of macular surgery in diabetic retinopathy, only the answer to the second question is summarized and discussed.
Data from the ETDRS shows that focal photocoagulation for “clinically significant” macular edema (CSME) in diabetic retinopathy substantially reduces the risk of moderate visual loss. Focal treatment also increased the chance of visual improvement, decreases the frequency of persistent macular edema, and causes only minor visual-field losses. The beneficial effects of treatment demonstrated in this trial suggested that all eyes with CSME should be considered for focal photocoagulation, even if visual acuity is not yet reduced. CSME includes not only focal but also diffuse macular edema (5, 6). However, the beneficial effects of focal photocoagulation for diffuse macular edema are not clear, given that these eyes respond poorly to treatment as compared to eyes with focal macular edema (3).
CLASSIFICATION OF DIABETIC MACULAR EDEMA
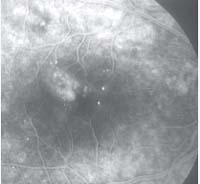
Bresnick (7, 8) classified diabetic macular edema into focal macular edema and diffuse macular edema (Table 21-1). Focal macular edema is characterized by focal leakage mainly from microaneurysms but occasionally from dilated capillaries. This leakage can be demonstrated clearly by intravenous fluorescein angiography. Often there is associated accumulation of extravascular lipoprotein exudate deposition in a circinate pattern (Fig. 21-1). In contrast, diffuse macular edema is characterized by diffuse leakage from retinal vessels in and around the macular area, often accompanied by cystoid macular changes (Fig. 21-2). Bresnick (7) stated that diffuse macular edema may result from not only a breakdown of the inner blood–retinal barrier (e.g., microaneurysms, retinal capillaries, and even arterioles) but also a breakdown of the outer blood–retinal barrier (i.e., retinal pigment epithelium).
TABLE 21-1 CLASSIFICATION OF DIABETIC MACULAR EDEMA
I. Focal leakage
A. Focal hard exudate rings
B. Multifocal edema
C. Perifoveolar edema and exudate
II. Diffuse leakage
A. Diffuse edema (cystoid)
B. Systemic factors
1. Fluid retention (cardiac, renal)
2. Severe hypertension
3. Pregnancy
C. Cystoid macular edema following panretinal photocoagulation
From Bresnick GH. Diabetic macular edema: a review. Ophthalmology 1986;93:989–997
DEFINITION OF CLINICALLY SIGNIFICANT MACULAR EDEMA
The ETDRS (5) defined CSME as the presence of one or more of the following criteria:
 Thickening of the retina at or within 500 mm of the center of the macula (Fig. 21-3A,B).
Thickening of the retina at or within 500 mm of the center of the macula (Fig. 21-3A,B).
 Hard exudates at or within 500 mm of the center of the macula, if associated with thickening of adjacent retina (not residual hard exudates remaining after disappearance of retinal thickening) (Fig. 21-3C).
Hard exudates at or within 500 mm of the center of the macula, if associated with thickening of adjacent retina (not residual hard exudates remaining after disappearance of retinal thickening) (Fig. 21-3C).
 A zone or zones of retinal thickening one disc area or larger, any part of which is within one disc diameter of the center of the macula (Fig. 21-3D).
A zone or zones of retinal thickening one disc area or larger, any part of which is within one disc diameter of the center of the macula (Fig. 21-3D).
STUDY DESIGN AND TREATMENT METHODS OF THE EARLY TREATMENT DIABETIC RETINOPATHY STUDY
The ETDRS had a somewhat complex randomization scheme (Figs. 21-4–21-6). First, eyes with macular edema were subdivided into two groups: eyes with less severe retinopathy (mild-to-moderate nonproliferative retinopathy), and eyes with more severe retinopathy (severe nonproliferative or early proliferative retinopathy). Then each subgroup was further randomly assigned to “early (immediate) photocoagulation” or “deferral of photocoagulation” until high-risk proliferative retinopathy developed. High-risk proliferative retinopathy has been previously defined by the Diabetic Retinopathy Study (9) as retinopathy with moderate or severe optic nerve neovascularization or any neovascularization with hemorrhage.
For focal treatment of macular edema, a pretreatment fluorescein angiogram was used during photocoagulation to identify “treatable lesions” (Table 21-2). Treatment was prescribed for all such lesions located within two disc diameters of the center of the macula. Treatment of lesions closer than 500 mm to the macula was not required initially. If vision was less than 20/40, however, and the retinal edema and leakage persisted, treatment of lesions up to 300 mm from the center was recommended. For focal macular edema, microaneurysms and other focal leakage sites received photocoagulation. Areas of diffuse leakage were treated in a grid pattern.
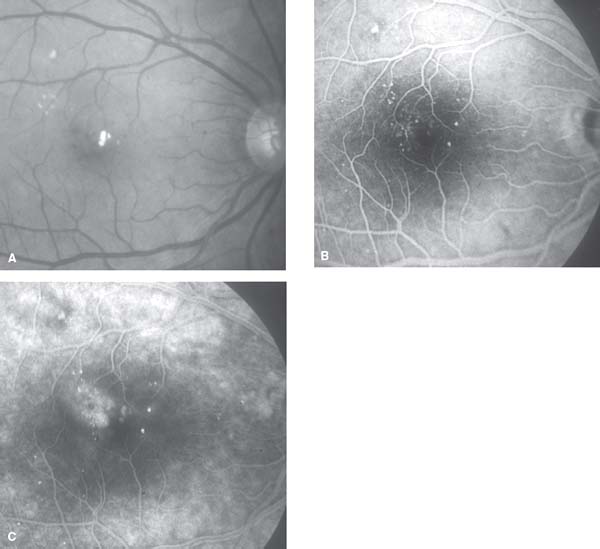
Figure 21-1. Focal macular edema. A: Right eye. Macular edema with central involvement, multiple microaneurysms scattered around the posterior pole, and hard exudates deposited in the macular and upper temporal area of the posterior pole (visual acuity 20/30). B: Early phase of fluorescein angiogram shows clusters of microaneurysms. C: Late phase of angiogram shows leakage from microaneurysms.
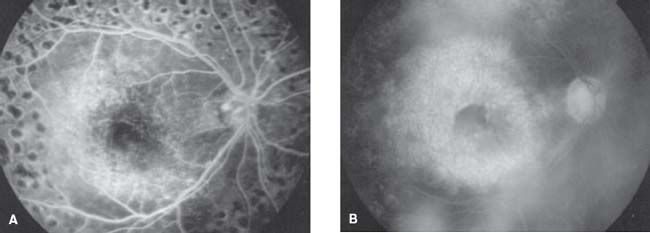
Figure 21-2. Diffuse macular edema with cystoid changes following panretinal photocoagulation. A: Early phase of fluorescein angiogram shows widespread capillary dilation and leakage in the posterior pole. B: Late phase of angiogram shows extensive pooling of dye in cystoid spaces in not only the macular area but also in other areas of the posterior pole (visual acuity 20/60).
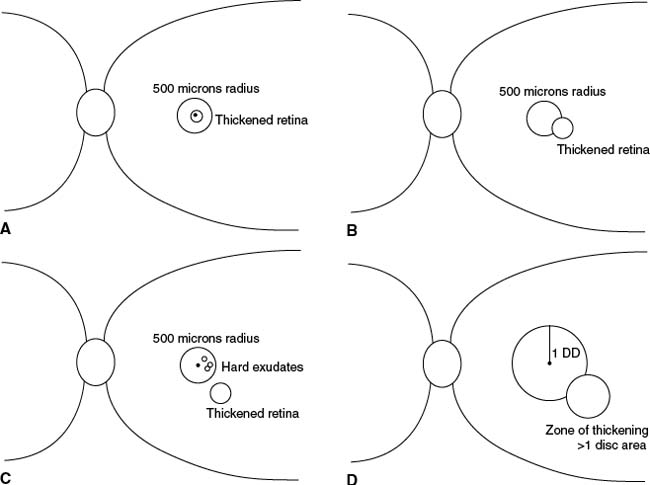
Figure 21-3. Definition of clinically significant macular edema. A: Thickening of the retina at the center of the macula. B: Thickening of the retina within 500 mm of the center of the macula. C: Hard exudates at or within 500 mm of the center of the macula with thickening of adjacent retina. D: A zone of retinal thickening one disc area or larger, located less than one disc diameter from the center of the macula.
For scatter (panretinal) photocoagulation, eyes were further randomized to either “mild” scatter (400–650 burns) or “full” scatter (1200–1600 burns).
EYES WITH MACULAR EDEMA AND LESS SEVERE RETINOPATHY
Early (immediate) photocoagulation for eyes with macular edema and less severe retinopathy consisted of 1) immediate focal macular photocoagulation, with delayed scatter photocoagulation (mild or full) added if more severe retinopathy developed during follow-up; and 2) immediate scatter photocoagulation (mild or full), with focal macular photocoagulation delayed at least 4 months.
RESULTS OF EARLY TREATMENT DIABETIC RETINOPATHY STUDY REPORT NUMBER 1
The first ETDRS report (5) compared the results of immediate focal macular photocoagulation (754 eyes) with the results of deferred photocoagulation (1490 eyes) (Fig. 21-4). The results of the comparison were as follows:
 At 3-year follow-up, 12% of the eyes undergoing immediate treatment and 24% of those undergoing deferred treatment had significant loss of visual acuity.
At 3-year follow-up, 12% of the eyes undergoing immediate treatment and 24% of those undergoing deferred treatment had significant loss of visual acuity.
 Of eyes with a pretreatment visual acuity of 20/40 or worse, 40% of those undergoing immediate treatment and 20% of those undergoing deferred treatment had gained more than one line of visual improvement on the ETDRS visual acuity chart after 2 years’ follow-up. Improvement of three or more lines, however, was uncommon (<3%) in either group.
Of eyes with a pretreatment visual acuity of 20/40 or worse, 40% of those undergoing immediate treatment and 20% of those undergoing deferred treatment had gained more than one line of visual improvement on the ETDRS visual acuity chart after 2 years’ follow-up. Improvement of three or more lines, however, was uncommon (<3%) in either group.
TABLE 21-2 CHARACTERISTICS OF TREATABLE LESIONS
1. Discrete points of retinal hyperfluorescence or leakage (most of these are microaneurysms)
2. Areas of diffuse leakage within the retina
Microaneurysms
Intraretinal microvascular abnormalities
Diffuse leaking retinal capillary bed
3. Retinal avascular zones
From Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema: Early Treatment Diabetic Retinopathy Study report number 1. Arch Ophthalmol 1985;103:1746–1806.
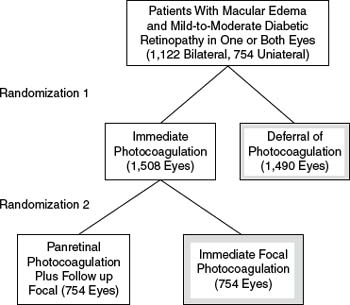
Figure 21-4. The Early Treatment Diabetic Retinopathy Study treatment schedule for patients with macular edema and less severe retinopathy in one or both eyes. Randomization 1: All study patients had one eye randomly assigned to immediate photocoagulation, and the other eye to deferral of photocoagulation. Randomization 2: Eyes assigned to immediate photocoagulation were further randomized to either a combination of initial panretinal photocoagulation and follow-up focal macular photocoagulation or immediate focal photocoagulation. Hatched boxes indicate those groups compared in this report. (From Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema: Early Treatment Diabetic Retinopathy Study report number 1. Arch Ophthalmol 1985;103:1796–1806).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


