Type
Power/energy
No. of shots
Extent of area treated (degree)
Avoid 3 and 9 o’clock position
Noncontact TCP (Nd:YAG)
7–8 W for 0.02 s
24–32 (8 per quadrant)
270–360
Yes
Contact TCP (Nd:YAG)
7–9 W for 0.7 s
17–20
270
Yes
Contact TCP (diode)
1–2 W for 1.5–2.5 s
17–20
270
Yes
ECP (diode)
0.3–0.9 W
Not applicable
180–360
No
Indications
Transscleral Cyclophotocoagulation
TCP is an effective procedure for reducing intraocular pressure (IOP). It is usually performed after medications and filtration surgeries have been tried and have failed. TCP is a valuable option in eyes suffering from severe forms of glaucoma, such as neovascular or traumatic, typically with end-stage disease and significant loss of visual acuity. However, diode TCP has been successfully employed as a primary surgical procedure [54–57] and has been used in eyes with good visual acuity [40]. In fact, studies evaluating diode TCP as a primary surgery had good results both in open-angle and in angle-closure glaucomas, with few, if any, serious complications [55–57].
Endoscopic Cyclophotocoagulation
As in TCP, ECP is indicated in glaucomas uncontrolled by medical treatment and/or filtering surgery [44–53]. It has been used in primary open-angle, pseudoexfoliation, neovascular, post-penetrating keratoplasty, pediatric, and angle-closure glaucomas [52]. ECP has been used as a primary glaucoma surgery in conjunction with cataract extraction [43–45] and also with tube shunt [58]. In fact, eyes with relatively intact central visual acuity may be appropriate candidates for ECP [43–45].
However, because the intraocular pressure (IOP) lowering with ECP seems modest, eyes with very elevated pressures may be considered more appropriate for TCP, particularly if potential visual function is limited. In the situation of excessively high IOP with intact vision, filtration surgeries are still the procedures of choice. These recommendations are based, in part, on the experience of the authors, since there are no studies that directly compare ECP to TCP or trabeculectomy in a randomized, controlled fashion. In, summary, the indications for ECP and TCP are evolving as both procedures are being performed in clinical scenarios that traditionally have been treated by filtrating procedures.
Methods for TCP and ECP
Some of the techniques described below reflect the authors’ personal preferences on the basis of their experience.
Transcleral Cyclophotocoagulation (TCP)
Clinically, two types of laser are used for TCP: neodymium/yttrium-aluminum-garnet (Nd:YAG) and diode.
Preoperatively, a retrobulbar injection is provided because the application of laser energy can be painful, and there may be postoperative pain. The anesthetic agent(s) can be 2 % lidocaine only or a 1:1 mixture of 4 % lidocaine and 0.75 % bupivacaine. Topical proparacaine or tetracaine is also applied before laser treatment. A lid speculum is usually placed for optimal exposure, and the patient is in the supine or reclined position. Transscleral illumination may be used to identify ciliary body positioning with respect to the limbus.
Nd:YAG TCP
The Nd:YAG laser (Surgical Laser Technologies Inc., Malvern, PA., USA) was one of the first used to do TCP. The probe is rounded and the energy delivery is through the center. Placement of the center of the probe is 1–2 mm posterior to the limbus, which can be measured by calipers but is often estimated visually. Energy levels are started at about 7 W and 0.7 s and are titrated to avoid an audible “pop” that indicates overtreatment and explosion of the ciliary body tissue. A total of 17–20 spots are usually applied to treat 270° of ciliary processes, avoiding the 3 and 9 o’clock positions (Table 9.1).
After the procedure, atropine and dexamethasone ointments are applied and the eye is patched. The patch may be removed in the evening and glaucoma drops should be reinstituted. Prostaglandin analogs may be excluded in the short term if cystoid macular edema (CME) is a concern, and cholinergics should be temporarily discontinued to avoid increased inflammation. Postoperative prednisolone acetate 1 % is applied 4 times daily for 10–14 days and tapered according to inflammation.
Diode TCP
The diode laser (IRIS Oculight SLx, Iris Medical Inc., Mountain View, CA, USA) (Fig. 9.1a) emits at 810 nm, and the probe has a tip shaped as a footplate (Fig. 9.1b). The heel of the footplate is placed adjacent to the limbus, and the laser tip is positioned 1.2 mm behind to be over the ciliary body. The laser tip, which protrudes 0.7 mm, should be applied firmly against the conjunctiva/sclera to help avoid conjunctival burn. The treatment principles are similar to the Nd:YAG laser. The initial energy settings are often about 1,000 mW with 2 s duration (Table 9.1). Lower energy levels can be used with longer durations. The 3 and 9 o’clock positions are avoided and a total of 17–20 shots are applied over approximately 270°. Energy is titrated to be just below that needed to achieve the “pop” sound. The number of treatment spots and avoidance of the 3 and 9 o’clock positions are similar to that for the Nd:YAG laser.
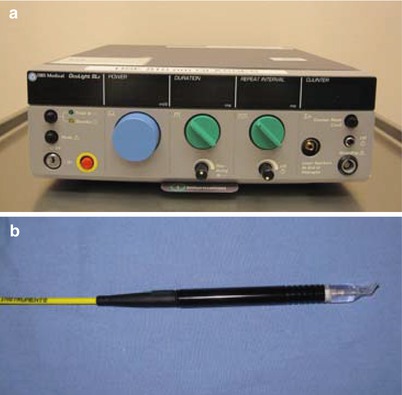
Fig. 9.1
(a) Semiconductor diode laser (IRIS Oculight SLx, Iris Medical Inc., Mountain View, CA) for diode contact TCP. (b) “G-probe” handpiece for contact diode TCP
Endoscopic Cyclophotocoagulation (ECP)
Devices
The laser unit for ECP (Endo Optiks, Little Silver, NJ, USA) incorporates a diode laser that emits pulsed continuous-wave energy at 810 nm, a 175 W xenon light source, a helium-neon laser aiming beam, and video camera imaging, which can be recorded (Fig. 9.2a). All four elements are transmitted via fiber optics to an 18-gauge or 20-gauge probe (Fig. 9.2b), which is inserted intraocularly. The optimum focus for the laser is 0.75 mm from the probe tip, and the endoscope provides a 70° field of view. The main unit is compact and portable, with a maximum power output of 2.0 W. Controls for laser power and duration (up to 9.99 s) are adjustable on the console. The foot pedal controls laser firing with the actual duration of each treatment determined by how long the pedal is depressed.

Fig. 9.2
(a) ECP unit (Uram E2, Endo Optiks, Little Silver, NJ), including laser and monitor. (b) ECP probe (20 gauge)
Techniques
The two main approaches to reach the ciliary processes are via a limbal or a pars plana entry. The limbal approach is preferred because anterior vitrectomy and associated risks for choroidal and retinal detachment are avoided. However, there are some cases that are more safely treated through the pars plana, for example, in aphakic eyes with posterior synechiae limiting access to the ciliary sulcus. In both situations, a retrobulbar block with lidocaine and bupivacaine is performed or general anesthesia can be considered in selective cases.
In the limbal approach, after dilation of the pupil with cyclopentolate 1 % and phenylephrine 2.5 %, a paracentesis is created and the anterior chamber is filled with viscoelastic agent, which is further used to expand the nasal posterior sulcus. This viscoelastic expansion of the posterior chamber allows for easier approach to the pars plicata with the ECP probe. A 2.2-mm or 2.5-mm keratome is then used to enter into the anterior chamber at the temporal limbus. After orientation of the probe image outside of the eye, the 18-gauge or 20-gauge probe is inserted through the incision and into the posterior sulcus. At this time, the ciliary processes are viewed on the monitor and treatment can begin. The laser is set at continuous wave and energy settings are 300–900 mW (Table 9.1). Approximately a 180° span of ciliary processes is photocoagulated (more area can be treated if a curved probe is used). Laser energy is applied to each process until shrinkage and whitening occur. Ciliary processes are treated individually or in a “painting” fashion across multiple processes. If excessive energy is used, the process explodes (or “pops”) with bubble formation, leading to excessive inflammation and breakdown of the blood-aqueous barrier. After the nasal 180° of ciliary processes are treated, a separate incision is created at the nasal limbus in a similar fashion as above. The temporal processes are then photocoagulated for a total of up to 360°, if so desired. Typically, 180–360° are treated [46–48, 57]. The authors’ preference is to treat 270–360° of processes. Before closure of the wounds, viscoelastic is removed from the anterior chamber with irrigation and aspiration.
In all patients, whether under local or general anesthesia, retrobulbar bupivacaine is administered before or at the end of the surgery to minimize postoperative pain. Sub-Tenon’s injection of 1 mL of triamcinolone (40 mg/mL) is also given for inflammation. On postoperative day 1, patients are placed on a regimen of topical antibiotics, steroids, nonsteroidal anti-inflammatory agents, cycloplegics, and their preoperative glaucoma medications except for miotics and prostaglandin analogs because these may exacerbate intraocular inflammation or its sequelae. Antibiotics are discontinued after 1 week, and the steroids, nonsteroidal anti-inflammatory agents, and cycloplegics are tapered as inflammation subsides. Glaucoma medications are removed according to the IOP requirements. Administration of acetazolamide during the evening of surgery may be used to prevent a spike in IOP from underlying glaucoma, inflammation, or possible retained viscoelastic.
Efficacy
TCP
Both contact and noncontact TCP have been shown to be effective surgeries for treating refractory glaucoma in which medications and/or other surgeries have failed. Although definitions of success vary among reports, success rates for IOP control have been between 34 and 94 %, with mean follow-ups of up to 5.85 years [14–41].
The amount of energy used for diode TCP seems to correlate with treatment success without leading to a higher complication or vision loss rate [36–38]. In their meta-analysis of 47 eyes treated with diode TCP, Hauber and Scherer [37] found a direct, linear correlation between the success rate (IOP <22 mmHg) and total energy delivered. The risk of additional complications or vision loss was not increased. Murphy et al. [36] retrospectively examined the dose–response relation and found that there was a linear dose–response for the subset of neovascular glaucoma cases but not for the group as a whole. Although high pretreatment IOP and high mean energy per treatment episode seemed to be associated with hypotony, this was not statistically significant on multivariate analysis. Noureddin et al. [38] prospectively evaluated an aggressive protocol in 36 eyes. The relatively high treatment settings were kept constant (2,250 mW, 2,000 ms, and total of 28 shots), even if pops were achieved. The success rate (IOP <22 mmHg) was good (72 %), and there was relative preservation of vision without permanent complications. However, there are several studies which did not find a direct correlation between energy delivered and IOP outcome.
ECP
One of the largest series on ECP was reported by our group at UCSF and included 68 eyes from 68 patients with refractory glaucoma of various diagnoses including primary open angle (16), congenital (12), chronic angle closure (11), aphakic/pseudophakic (10), uveitic (10), pseudoexfoliation/pigmentary (5), neovascular (2), and traumatic (2) [46]. With the exception of those undergoing combined cataract extraction and ECP, all of these patients had failed maximal medical therapy, and most had undergone one or more prior glaucoma surgeries. Eyes received between 180° and 360° of ciliary body treatment. The majority (56 eyes, 12 had concurrent cataract extraction) were treated through the limbal approach, whereas the others (12 eyes) were treated via pars plana incision. Seven percent had retreatment. The mean follow-up period was 12.9 months and the mean preoperative IOP was 27.7 mmHg. The mean IOP at last follow-up was 17.0 mmHg, yielding a mean reduction of 10.7 mmHg (34 % mean reduction). Glaucoma medication usage was reduced from an average of 3.0 preoperatively to 2.0 postoperatively. Success in controlling IOP <22 was 90 % at last follow-up.
Combined ECP with phacoemulsification cataract surgery has shown some promise in cases that are not refractory to maximal medical therapy [45–48]. Some studies on ECP have targeted childhood glaucomas [50–53]. As expected in pediatric cases, the success rate is not as high as in adult cases, and there is a greater risk for serious complications.
There are no studies directly comparing the results of ECP versus TCP. The lack of randomized trials may be related to the relatively different indications for each procedure.
Complications
The complication rates after TCP varied significantly depending on the laser type, glaucoma diagnosis and severity, treatment protocol, and other factors [14–41]. Side effects include pain, vision loss, hyphema, anterior segment uveitis, cataract progression, hypotony, and phthisis. The outcome is typically less predictable than in other glaucoma surgeries, and there is often a substantial risk for significant vision loss [14–39]. In the more recent studies where TCP has been used as a primary surgery, the rates of serious complications seem to be none to few in number [40, 41, 54–57]. This may be related to the lower energy settings and the relatively higher proportion of primary open-angle glaucoma and less severe forms of glaucoma than in prior studies. In numerous studies, TCP has had significant rates of hypotony and/or phthisis, which may relate to its external approach. Greater energy is generally required to penetrate the sclera as compared with the endoscopic approach, which is a more selective ablation of the ciliary processes under direct visualization. Often there is overtreatment of the ciliary tissues and surrounding structures including the vasculature, the pars plana, and the iris root, all of which may potentially predispose to phthisis or hypotony. In addition, there have been several published reports of sympathetic ophthalmia (SO) after TCP [59–61]. Lam et al. [61] reported that the incidence of SO at their institution was 5.8 % (4 of 69) and 0.67 % (1 of 150) after noncontact and contact Nd:YAG CPC, respectively. Malignant glaucoma has also been reported after diode TCP [62, 63]. Recently, necrotizing scleritis has been reported after diode TCP [64, 65].
Complications associated with ECP included the following in the largest series [46] to date: fibrin exudate in 24 %, hyphema in 12 %, CME in 10 %, vision loss of 2 lines or greater in 6 %, and choroidal detachment in 4 %. Other reported serious complications include retinal detachment and hypotony, although most of these were in pediatric cases [50]. Although not reported in the literature, endophthalmitis and choroidal hemorrhage are potential severe complications, owing to the intraocular nature of the surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


