Chapter 16 Laser and Radiofrequency Treatment of Thyroid Nodules and Parathyroid Adenoma
 Please go to expertconsult.com to view related video Laser and Radiofrequency Treatment of Thyroid Nodules and Parathyroid Adenoma.
Please go to expertconsult.com to view related video Laser and Radiofrequency Treatment of Thyroid Nodules and Parathyroid Adenoma.
 This chapter contains additional online-only content, including exclusive video Laser and Radiofrequency Treatment of Thyroid Nodules and Parathyroid Adenoma, available on expertconsult.com.
This chapter contains additional online-only content, including exclusive video Laser and Radiofrequency Treatment of Thyroid Nodules and Parathyroid Adenoma, available on expertconsult.com.Introduction
Thermal energy sources such as laser, radiofrequency (RF), or microwave (MW) make the destruction of tumors possible without surgical removal (see also Chapter 54, Ablative Percutaneous Ultrasound-Guided Ethanol Injection for Neck Nodal Metastases in Papillary and Sporadic Medullary Thyroid Carcinoma). The potential advantages of in situ tumor ablation include decreased costs, reduced morbidity, the possibility of performing procedures on outpatients, and the possibility of treating patients who are poor candidates for surgery because of age, comorbidity, or extent of disease. The main disadvantages of in situ ablation procedures, instead, concern the difficulty of evaluating the extent of disease and of the irreversible tissue damage induced by image-guided thermal ablation. Ultrasound (US) is the imaging technique most frequently used for the thyroid gland and thyroid ablation procedures.
Image-Guided Tumor Ablation
The term image-guided tumor ablation is defined as the direct application of chemical or thermal therapies to a specific focal tumor(s) in an attempt to achieve eradication or substantial tumor destruction.1 Since the mid-1980s, several methods for chemical or thermal tumor destruction have been developed and clinically tested.2 Image guidance is critical to the success of these therapies.3–12
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
Thermal Ablation
The thermal ablation therapies involved in clinical practice can be classified as either hyperthermic treatments, including RF ablation (RFA), laser ablation (LA or percutaneous PLA), microwave ablation (MWA), and high-intensity focused ultrasound (HI-FU), or cryoablation (CA). The thermal damage caused by heating depends both on the tissue temperature reached and on the duration of heating. For example, heating tissue at 50° C to 55° C for 4 to 6 minutes produces irreversible cellular damage; at temperatures between 60° C and 100° C, near-immediate coagulation of tissue is induced; and at over 100° C to 110° C, tissue vaporizes and carbonizes.13,14 On the other hand, freezing tissue at temperatures between −20° C and − 60° C, followed by rapid thawing, disrupts cell membranes and induces cell death.15–20 To adequately destroy tumor tissue, the entire target volume must be subjected to cytotoxic temperatures.
Laser Ablation
The term laser ablation refers to ablation with light energy applied via fibers directly inserted into the tissue.21–29 LASER is the acronym for light amplification by stimulated emission of radiation.
 Please see the Expert Consult website for more discussion of this topic, including Figure 16-1.
Please see the Expert Consult website for more discussion of this topic, including Figure 16-1.
Figure 16-1 illustrates the basic principles of laser radiation. The pumping system stimulates emission of photons by a gain medium, which is typically a gas, a crystal, or a semiconductor. These photons are reflected between two mirrors (a sort of resonant cavity), stimulating the emission of other photons as a chain reaction. Laser light escapes from resonant cavity through one of the mirrors, which is partially transparent. An optical connector conveys the laser beam into an optic fiber. Unlike normal light, laser light is collimated, monochromatic, coherent, and powerful. Laser technology directs high-level energy to a well-delineated area of tissue in a predictable, precise, and controlled way. A number of laser sources and wavelengths are currently available, and different types of laser fibers, modified tips, and applicators can be used. For example, the neodymiun:yttrium aluminum garnet lasers (Nd:YAG) with a wavelength of 1064 nm are used for percutaneous laser ablation (PLA) because penetration of light is optimal in the near-infrared spectrum.
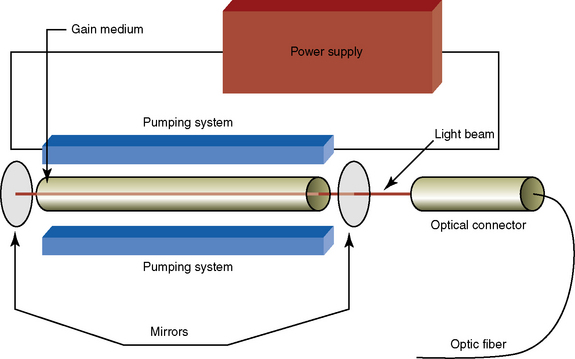
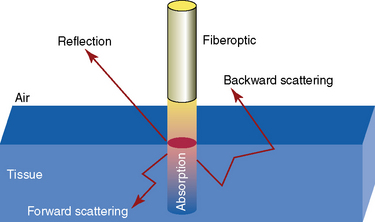
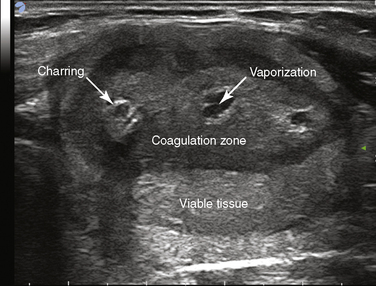
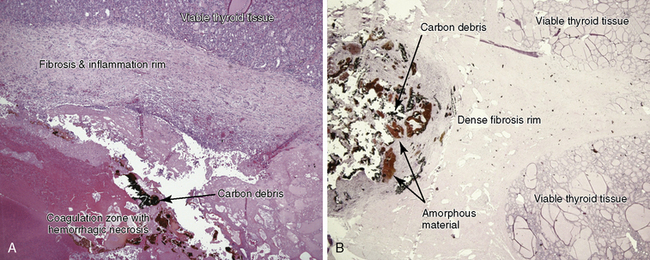
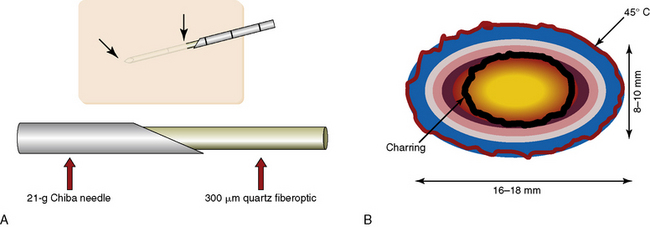
Figure 16-2 shows laser-light/tissue interaction. Laser light penetrates only a few millimeters as a result of backward and forward scattering and reflection. Scattering results in a relatively uniform distribution of absorbed energy, and heat is produced by the conversion of light absorption. Farther away from the point of application, the tissue is heated by conduction.22,24,25 Tissue is destroyed primarily through absorption (about 80%), which is a function of the attenuation coefficient (determined by tissue structure and wavelength), fiber tip shape, and delivered energy (determined by exposure time and output power). High power destroys tissue by means of vaporization, charring around the fiber tip surrounded by a coagulation zone, as seen on ultrasound images (Figure 16-3). Heat deposition is greatest near the thermal source, with a rapid energy decay.30,31 Cell death may continue up to 72 hours after the procedure because of the coagulation of microvessels and ischemic injury.32 Microscopically, the coagulation zone is surrounded by a rim of reversible damage that separates necrotic from viable tissue.31,33 Figure 16-4 shows microscopic changes occurring in thyroid nodules resected 1 month and 2 years after PLA, respectively. Charring is the main cause of decreased energy transmission, which in turn limits the coagulation zone. In addition, coagulation necrosis itself reduces optical penetration by about 20% in both normal and tumor tissue.28,34 Using a bare tip, almost spherical lesions with a maximum diameter of 12 to 16 mm can be produced.35 Lesion size can be increased by using beam splitters for simultaneous use of multiple fibers in an array around the tumor.27,36
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
This avoids the problem of repositioning single fibers and the difficulties associated with treatment-induced imaging artifacts. In vitro studies have shown that simultaneous treatment with four fibers at a 1- to 2-cm separation produces lesions that are 11 times larger than those produced with a single fiber, creating a lesion cylinder 4 cm in diameter and 3 cm in height.37,38 Simultaneous multifiber treatment produces lesions averaging 3.6 × 3.1 × 2.8 cm in normal canine liver.36 This multiple fiber technique has been employed in recent years both in a single institution and in multicentric studies in patients with focal primary and metastatic liver lesions.39–41 Bare fibers are now often being replaced by specially designed fibers equipped with diffuser endings that emit light up to a distance of 10 to 30 mm and with liquid cooling that increases lesion size by allowing higher power while avoiding charring.42–44
By simultaneously inserting four fibers and using fiber cooling, tumors with a diameter of 5 cm can be safely eradicated in a single treatment session, as reported in the largest series of local ablation in a single institution.45 Using a 980-nm diode laser ablation system in an in vivo tumor model with an internally cooled applicator, large ellipsoid thermal ablation with sharp boundaries was obtained in less than 3 minutes.46 Sophisticated systems for controlling lesion characteristics and lesion size using feedback systems and dose-planning are available with laser technology.6,37,47–49 An important practical advantage over other thermal sources is that the thin and flexible laser fibers make it possible to reach tumors more easily and safely.39
Laser Ablation in the Thyroid Gland
Outpatient US-guided (US-g) interventional procedures have been proposed to treat benign solid thyroid nodules without open surgery. This new approach is possible thanks to the combined use of ultrasonography (US) and fine-needle aspiration biopsy (FNA), which greatly reduces the need for diagnostic thyroidectomy.50 The 2009 American Thyroid Association (ATA) management guidelines for patients with thyroid nodules and differentiated thyroid cancer suggest either no treatment or partial/total thyroid surgery for patients with benign solid thyroid nodular disease, depending on nodule size, growth, and symptoms,51 and the 2010 American Association of Clinical Endocrinologists–Associazione Medici Endocrinologi (Italian Association of Clinical Endocrinologists)–European Thyroid Association (AACE-AME-ETA) thyroid nodule guidelines have for the first time introduced US-guided interventional approaches as a possible choice for thyroid nodule clinical management.52 The basic principle of locoregional treatment is to induce shrinkage of solid thyroid nodules using physical means for tissue destruction. Although US-guided percutaneous ethanol injection (PEI) is the treatment of choice for cystic nodules, it is no longer recommended for solid nodules,51–53 and high-intensity focused ultrasound (HI-FU), successfully experimented in ewes,54,55 has been used to treat an autonomous thyroid nodule in humans in a single case.56 PLA, the first thermal ablation technique, was introduced by Pacella et al.57 in 2000. Since then several studies have been published on its effects on thyroid cold,58–61 cystic,62 and hot nodules,59,62–68 including controlled trials,69–72 demonstrating that this new technique is effective and safe. Indeed, we have been using PLA in patients with benign thyroid cold nodules in Reggio Emilia, Italy, since 2002.
Technique
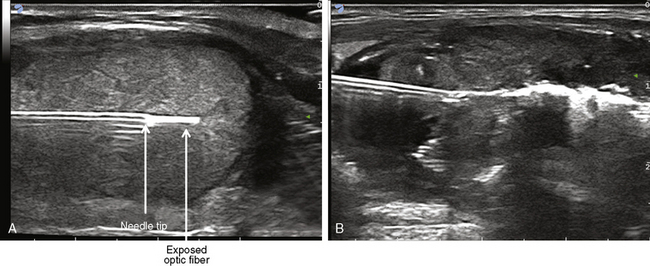
PLA is an outpatient procedure carried out on fasting subjects. The flat tip technique, proposed and developed by Pacella et al.,57 is based on the insertion of a 300-μm plane-cut optic fiber through the sheath a 21-g Chiba needle, exposing the bare fiber in direct contact with thyroid tissue for a length of 5 to 7 mm, based on the size of the lesion (Figure 16-5).
 Please see the Expert Consult website for more discussion of this topic, including Figure 16-6.
Please see the Expert Consult website for more discussion of this topic, including Figure 16-6.
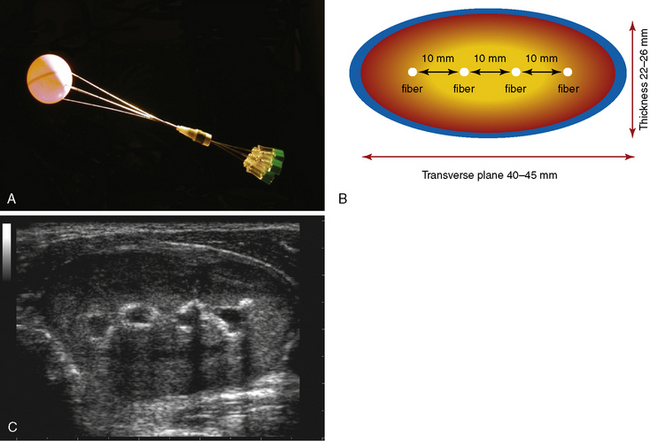
Fiber lockers avoid exposing the tip of the fiber within the lesion beyond the appropriate length. In the thyroid gland, multiple fibers are inserted parallel to each other to obtain an ellipsoid ablation that matches the ellipsoid shape of most thyroid nodules (Figure 16-6).61
Procedure
 Please see the Expert Consult website for more discussion of this topic, including Figure 16-7.
Please see the Expert Consult website for more discussion of this topic, including Figure 16-7.
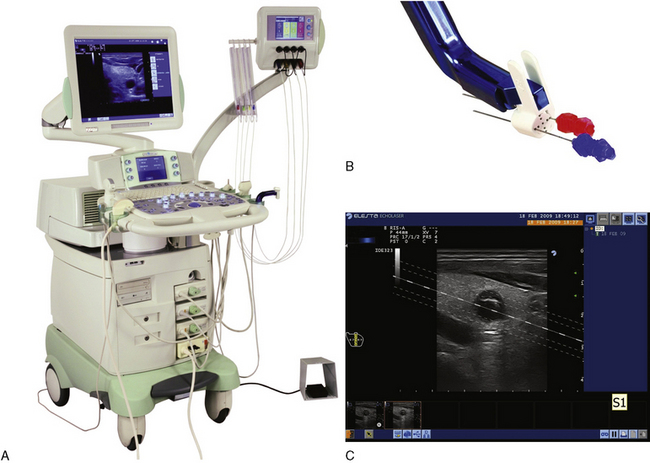
In Reggio Emilia, Italy, from 2002 to 2008 we used an Nd:YAG laser with a 1064-μm near-infrared wavelength emission, equipped with a four-source beam splitter (DEKA M.E.L.A., Florence, Italy). In 2009, we substituted this with new equipment composed of an ultrasound device and a laser unit (EcholaserX4, Elesta, Florence, Italy). The EcholaserX4 permits the operator to use up to four laser sources, each with its own energy emission setting and independent activation. This helps match the ablation zone to nodule size and shape. Our equipment also features software and a guidance system, which facilitates small thyroid nodule targeting (Figure 16-7).
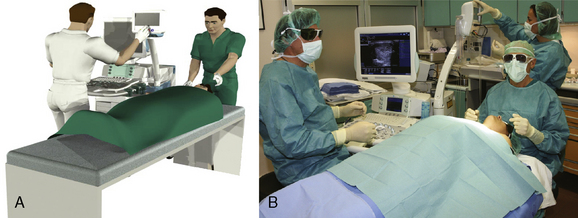
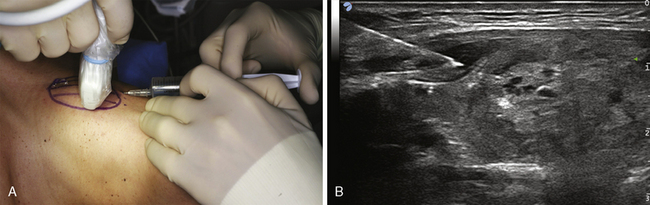
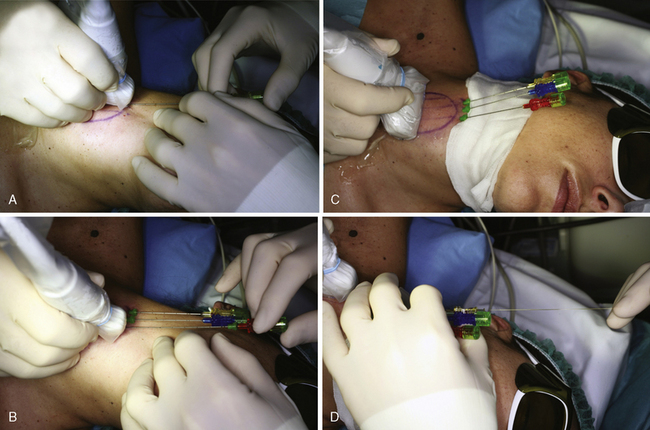
The patient is placed on an operating table in the supine position with hyperextended neck. The operator, seated behind patient’s head, watches real time US images on an auxiliary monitor placed on a tower at the patient’s feet. An assistant sitting to the right of the patient uses the US equipment (Figure 16-8). Light conscious sedation is obtained with i.v. midazolam. Emergency care drugs and equipment, including a defibrillator, are in the interventional suite. Although an anesthesiologist is not present during PLA sessions, we recommend performing PLA in a health care facility where an anesthesiologist and otolaryngology head and neck surgeons are available. Local anesthesia with 2% lidocaine subcutaneous and subcapsular infiltration (2 to 5 mL) is performed under US assistance with a thin (29 to 30 g) needle  (see Figure 16-9, available on expertconsult.com). Chiba G-21 needles (1 to 4) are placed manually along the longitudinal, craniocaudal, major nodule axis at a distance of 10 mm from each other, matching the anatomy of the nodule as closely as possible
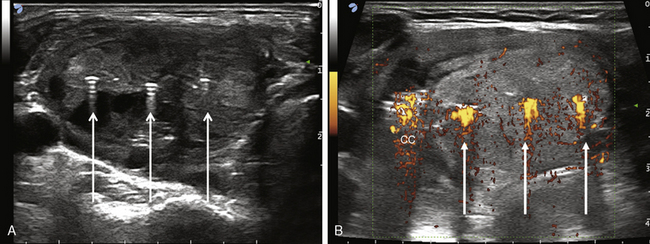
(see Figure 16-9, available on expertconsult.com). Chiba G-21 needles (1 to 4) are placed manually along the longitudinal, craniocaudal, major nodule axis at a distance of 10 mm from each other, matching the anatomy of the nodule as closely as possible  (see Figure 16-10, available on expertconsult.com). The assistant/sonographer performs multiplanar US images on axial and longitudinal scans throughout laser illumination, allowing real-time visual control of each source (Figure 16-11). An initial energy of 1200 to 1800 Joules (J) per fiber with an output power of 2 to 4 watts (W) is delivered starting 1 cm from the bottom of the lesion. A highly echogenic area resulting from tissue heating and vaporization gradually increases over time until coalescence between fibers is observed (Figure 16-12). Additional needle insertion of up to 1 cm and additional doses of laser energy are administered until a distance of 5 mm from the cranial portion of the nodule is reached.
(see Figure 16-10, available on expertconsult.com). The assistant/sonographer performs multiplanar US images on axial and longitudinal scans throughout laser illumination, allowing real-time visual control of each source (Figure 16-11). An initial energy of 1200 to 1800 Joules (J) per fiber with an output power of 2 to 4 watts (W) is delivered starting 1 cm from the bottom of the lesion. A highly echogenic area resulting from tissue heating and vaporization gradually increases over time until coalescence between fibers is observed (Figure 16-12). Additional needle insertion of up to 1 cm and additional doses of laser energy are administered until a distance of 5 mm from the cranial portion of the nodule is reached.
 Please see the Expert Consult website for more discussion of this topic, including Figure 16-13.
Please see the Expert Consult website for more discussion of this topic, including Figure 16-13.
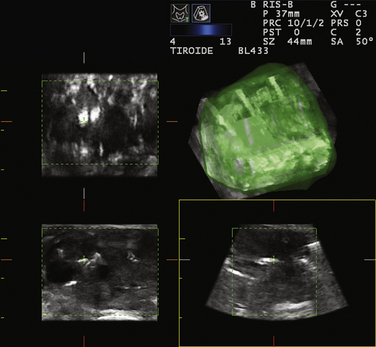
Three-dimensional ultrasound imaging may help in multiple needle fitting (Figure 16-13).
Although nodules as small as 5 mm may be ablated using a single optic fiber, nodules up to 40 to 50 mm in width, 30 to 35 mm in thickness, and 50 to 70 mm in length (i.e., up to 30 to 60 mL) may be treated in a single PLA session by combining multiple fiber placement, multiple needle advancements, and high energies. The number of fibers, number of advancements, and total energy delivered are tailored to nodule volume. The duration of laser illuminations ranges from 6 to 30 minutes, depending on nodule size.61 Light irradiation is continuous; it is suspended for fiber repositioning only in the event of severe pain, cough, or other side effects.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


