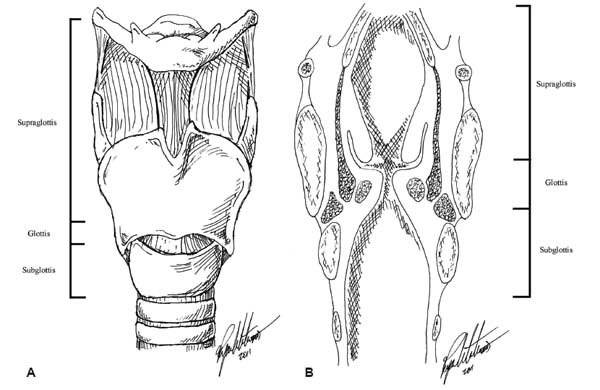
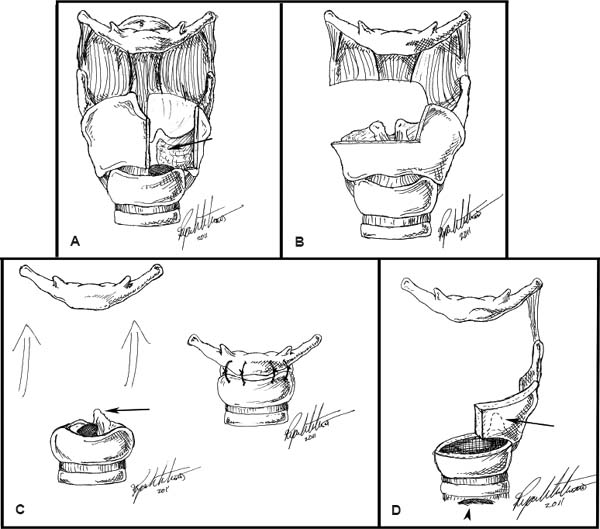
14 Core Messages • Most true neoplasms in the adult larynx represent malignancy. • Hoarseness persisting beyond 2 weeks is a “warning sign,” particularly in patients with risk factors for laryngeal carcinoma, and warrants prompt referral for evaluation by an otolaryngologist. • Smoking, especially when combined with alcohol consumption, is the most important risk factor for laryngeal cancer. • Early-stage laryngeal cancer can be treated with single modality therapy, while late-stage laryngeal cancer fares best with combined modality therapy. The larynx is a complex structure with multiple functions connecting the pharynx with the trachea and is divided into three sections for oncologic descriptive purposes: the supraglottis, glottis, and subglottis (Fig. 14.1). The supraglottis extends from the tip of the epiglottis superiorly to the true vocal cords (TVCs) inferiorly; this area encompasses both the laryngeal vestibule and the ventricle. The glottis comprises the TVC proper and the space between them—the rima glottidis. The subglottis extends from the undersurface of the TVCs superiorly to the inferior margin of the cricoid cartilage inferiorly. Laterally, the larynx extends to the lateral aspect of the thyroid and cricoid cartilages, and the posterior margin is defined by the posterior aspect of the arytenoid cartilages and interarytenoid space in the supraglottis, while the “party wall”—that is, the common wall shared by the posterior larynx/trachea and the cervical esophagus—defines the posterior aspect of the glottis and subglottis. The anterior boundaries of the larynx are the vallecula and preepiglottic space, the anterior surfaces of the thyroid cartilage, cricothyroid membrane, and cricoid cartilage, as well as the paraglottic space more laterally (Fig. 14.2). While there are many different neoplasms that can arise in the larynx, in adults the vast majority are malignant. Of these, greater than 90% are squamous cell carcinoma (SCC) and greater than 75% of these arise initially in the TVCs.1,2 SCC of the larynx is strongly associated with smoking tobacco; greater than 95% of laryngeal SCC is diagnosed in smokers or former smokers.1 A synergistic effect between tobacco use and alcohol consumption has been described; thus, patients who are both smokers and heavy drinkers are among the highest risk for cancers of the upper aerodigestive tract. A recent discovery is that of the role of human papillomavirus (HPV) in certain subtypes of SCC in the head and neck. While HPV appears to be more actively involved in the pathogenesis of tumors of the pharynx, rather than the larynx, precise mechanisms and risk factors are an area of active ongoing research. Many laryngeal neoplasms present at an advanced stage owing to a combination of vague early symptoms and patient denial. The most common presenting symptom of laryngeal cancer is hoarseness, though other common symptoms are globus sensation, hemoptysis, weight loss, odynophagia or sore throat, persistent cough, or earache.2,3 There are many neoplasms that can arise in the adult larynx, and the majority of these are malignant. As mentioned above, the most common malignant neoplasm is SCC, though others are possible and will be discussed in further detail. Of the rarer benign neoplasms, papilloma deserves special mention. Benign neoplasms present in much the same way as malignancy; however, weight loss may not be present. A history of childhood recurrent respiratory papillomatosis (RRP) may portend adult benign papillomatosis, but these may arise de novo as well in the absence of a childhood history. There are a multitude of subtypes of HPV, and the most common causative subtypes of RRP are HPV 6 and 11 compared with those associated with aerodigestive malignancy, where HPV 16 dominates.4 Verrucous or cauliflower-like lesions are traditionally thought to occur at areas of squamociliary junctions, such as the TVCs, but can be extensive. RRP is classically described as a disease of childhood that may persist into adulthood, with a significant subset of patients clearing the recurrent infections by puberty. Those whose infections do not spontaneously regress tend to have a heavier burden of disease, and these benign papillomas may spread throughout the aerodigestive tract to involve the oral and nasal cavities and bronchi, and may eventually undergo malignant degeneration. As the same HPV subtype responsible for RRP has also been described in genital papillomatosis, a vertical transmission model has been proposed. Indeed, half of all patients with RRP are born to mothers with active papillomatosis in the vaginal canal.5 These lesions may arise de novo in adulthood as well, and in those who do tend to have milder disease, but with less risk of malignant transformation. Surgical debulking remains the mainstay of treatment, with adjunct therapy such as local injection of cidofovir, or other antivirals, representing an area of ongoing clinical research as to the long-term effects on recurrence and severity. Figure 14.1 (A) Anterior and (B) coronal views of the larynx defining the supraglottis, glottis, and subglottis. SCC accounts for the great majority of laryngeal malignancies (> 90%), but there are other rare malignant tumors that can occur as well. While the bulk of the remainder of this chapter is devoted to the diagnosis and management of SCC, several of these rare, non-SCC tumors that deserve mention as well. Rests of minor salivary gland tumors exist throughout the upper aerodigestive tract. While the bulk of these lie in the oropharynx and hypopharynx, a small number of these exist in the larynx, particularly the supraglottis and subglottis. Ganly et al reviewed their experience of 33 years at Memorial Sloan-Kettering Cancer Center, a major international tertiary referral center, and identified 12 patients with such tumors6; of these, 10 had adenoid cystic carcinoma and 2 had myoepithelial carcinoma. Tumor site was 48% supraglottis and 52% subglottis, and most (10 patients) were treated with combined surgery and radiation therapy (XRT). Fifty-eight percent developed recurrent disease; of these, 50% locoregional and 50% distant recurrence were observed. The authors advocate aggressive surgical treatment, usually requiring total laryngectomy, based on the propensity for perineural and submucosal spread, as well as high recurrence rates. Neuroendocrine neoplasms in the larynx can be classified into two distinct groups: those of neural origin and those of epithelial origin. Laryngeal tumors of neural origin are paragangliomas, while those of epithelial origin are either carcinoid tumors or neuroendocrine carcinoma. Each of these tumor groups warrants a different management strategy. Paragangliomas display a female preponderance of nearly 3:1 and respond well to conservative surgical resection, with larynx preservation as appropriate. Carcinoid tumors, of which typical and atypical variants exist, are another treatment dilemma in themselves. Typical carcinoid tumor is exceedingly rare, but warrants only local resection as lymphatic spread has not been described. Likewise, chemotherapy and XRT have not been successful in reported cases. Atypical carcinoid tumor, the distinction being based on histologic criteria, has a high likelihood of locoregional lymphatic spread, and therefore elective neck dissection is necessary. The mainstay of treatment remains surgical, as results with chemotherapeutic agents and XRT have been disappointing. Primary neuroendocrine carcinoma of the larynx is a rare, aggressive tumor, and the surgical results are not satisfactory. Surgery is reserved for salvage situations, and chemotherapy remains the modality of choice for treatment. Despite this, long-term survival is poor, with 16% survival at 5-year posttreatment reported.7 Figure 14.2 (A) Anterior view of the larynx after left vertical partial laryngectomy. Arrow denotes the cut surface where left true vocal cord (TVC) was removed, but ipsilateral arytenoid was spared. (B) Anterior view after supraglottic laryngectomy. Note preservation of both TVCs and arytenoids. (C) Anterior view of the larynx after supracricoid laryngectomy before (left) and after (right) cricohyoidopexy. Arrow denotes preservation of left arytenoid. (D) Anterior view of the larynx after near-total laryngectomy. Arrow denotes preserved left arytenoids (dotted line), and arrowhead denotes permanent tracheostomy necessary for respiration. This group of carcinomas denotes those of glandular origin, but the most common subtype, “adenocarcinoma, not otherwise specified,” prohibits further histologic classification. These tumors are exceedingly rare, comprising far less than 1% of all laryngeal malignancies.8 So rare are these lesions that there are no agreed upon staging or treatment algorithms available. Primarily the realm of case reports in the literature, treatment often includes wide local excision, sparing as much of the larynx as possible, with adjuvant XRT after surgery. Survival of several years after such treatment has been reported. As with many non-SCC malignancies of the larynx, these lesions often present as submucosal masses, rather than the mucosal lesions often associated with SCC and its subtypes. Chondrosarcoma is a mesenchymal tumor, very rare in the head and neck, and classically presents as a tumor of the posterior cricoid cartilage, though described from the skull base to the cervical spine. These tumors are slow growing but ultimately locally aggressive and are treated primarily surgically, with larynx preservation when oncologically possible. XRT can be used in a salvage or adjunct fashion, but primary surgical resection remains the treatment of choice. Overall disease-free survival has been reported to be 73% at 5 years.9 Greater than 90% of laryngeal malignancies are SCC, and from a treatment perspective, these are classified as early-stage (T1 and T2) and late-stage (T3 and T4) tumors. The glottis represents the most common primary subsite for laryngeal SCC, accounting for 75% of tumors, followed by the supraglottis (approximately 20%) and subglottis (≤ 5%).2 Historically, all laryngeal SCCs were treated surgically via total laryngectomy. As advances were made in tumor biology, anatomy, surgical technique, XRT, chemotherapy, and immunotherapy, efforts in laryngeal preservation increased. Currently, early-stage (T1 and T2) tumors are typically treated with single modality therapy, often primary XRT. Primary surgical resection may be an option for some patients in the form of partial laryngectomy, and this will be discussed in greater detail later. Until the mid-1980, second-advanced laryngeal cancers were treated primarily with surgery (often total laryngectomy and adjuvant XRT). An interest in combined modality therapy (chemotherapy and XRT) began in mid-1980s. The landmark Veterans Affairs cooperative trial established combined chemotherapy and XRT as an acceptable alternative for patients with advanced laryngeal carcinoma who traditionally would require total laryngectomy.10 Recent data from the National Cancer Database (NCDB) have challenged the shift of advanced laryngeal cancer treatment to nonsurgical therapy. Investigators demonstrated for late-stage glottic, early-stage supraglottic, and T3N0M0 supraglottic SCC 5-year survival rates of only 59.2% for patients treated with combined chemotherapy and XRT and 42.7% for patients treated with XRT alone, as compared with 65.2% for patients treated with surgery plus XRT and 63.3% for those treated with surgery alone.11 These, and other, data suggest that surgery may provide a survival advantage, particularly in late-stage SCC. Whichever treatment modalities are chosen, it is imperative to treat not only the primary tumor but also the local and regional lymphatics as appropriate. Most of the larynx, with the exception of the glottis, is served by a rich lymphatic network with predictable drainage patterns. When describing these lymphatics, the neck is divided into five levels. The supraglottis drains primarily to levels II, III, and IV and may drain bilaterally. Thus in supraglottic SCC, both sides of the neck may harbor metastasis, either clinically/radiographically evident or occult. It is necessary to address these bilateral lymphatic beds in the treatment of supraglottic tumors, via either surgical neck dissection or XRT. The overall rate of occult metastasis is significant, being 16% in early-stage tumors and up to 62% in late-stage supraglottic SCC.12 Glottic SCC is somewhat unique. The glottis itself has a paucity of lymphatics; therefore, the rate of metastasis to the lymph nodes of the neck is significantly lower (< 10% of the patients with tumors confined to the glottis) than that observed in supra- or subglottic SCC. Tumors of the glottis may grow to be quite large and locally invasive (T3), but still may not metastasize to the lymphatics of the neck. Indeed, this subset of T3N0M0 glottic SCC, that is, large locally advanced tumors without regional or distant metastasis, was the only subset of patients that showed equal 5-year survival with either primary surgery plus XRT or primary chemotherapy plus XRT (65.6%) in the NCDB study.11 Elective neck dissection or irradiation is not routinely recommended for early-stage glottic SCC. In late-stage glottic SCC, some authors recommend treatment of the ipsilateral neck, particularly levels II and III, even if the patient is clinically and radiographically N0.13 It is important to note, however, that if a glottic SCC extends into the supraglottis or subglottis, the relevant lymphatics of these areas must be addressed as if the primary tumor were supraglottic or subglottic. Subglottic SCC represents approximately 1% of all laryngeal tumors, and it often presents at an advanced stage with airway obstruction. These tumors have a much poorer prognosis than either glottic or supraglottic SCC, and they frequently present with metastatic disease in the neck. Garas and McGuirt reported a 25-year experience with subglottic SCC; 80% of the patients presented with either T3 or T4 disease, and the 5-year survival rate was 25%.14 As in the supraglottis, lymphatic drainage can be bilateral, chiefly involving levels III and IV, but also frequently involving the central compartment of the neck, sometimes known as level VI, which is a space containing the Delphian lymph nodes extending from the cricoid cartilage superiorly to the sterna notch inferiorly and laterally bordered by the common carotid arteries. Further drainage along this lymphatic pathway allows metastatic disease entry into the pretracheal lymph nodes and the lymph nodes of the mediastinum. When considering surgical treatment of SCC of the larynx, total laryngectomy is the historical standard against which other surgical modalities are compared. It allows oncologically sound resection of the intact tumor plus a surrounding cuff of normal tissue at all margins. Removal of the entire larynx, however, carries with it real morbidity not only from the loss of natural voice but also from the loss of the sense of smell and much of the sense of taste, as well as a decrease in the ability to cough effectively. Such sequelae are the driving force behind the development of partial laryngectomy, also called organ-preservation surgery, where portions of the larynx are left intact, hoping for more natural function and improved quality of life. When considering organ-preservation surgery, it is important to determine whether the larynx is “competent” or not. A competent larynx is one that, despite the tumor, is able to perform the most basic of laryngeal functions of protecting the trachea and lower airways from oropharyngeal contents and subsequent aspiration, while allowing for adequate respiration. Vocal cord function plays a large role in laryngeal competence. Vocal cords may become paralyzed or weakened by tumor involvement of the cord or the recurrent laryngeal nerves that control them. If the vocal cords cannot close completely because of paralysis or tumor, oropharyngeal contents and secretions may pass through them and into the trachea, potentiating aspiration pneumonia. If the vocal cords cannot open fully because of paralysis or bulky tumor burden, there will not be an adequate airway for the patient to breathe comfortably. In either of these situations, careful consideration should be given to total laryngectomy as the safest surgical treatment option. Organ-preservation surgery makes sense only if the preserved organ is going to be functional for the patient. It is also crucial to counsel any patient undergoing a partial laryngectomy that findings at surgery may require conversion to total laryngectomy, and they must be amenable to this possibility before entering the operating room. First performed by Billroth in 1873, it was not until the mid-20th century that total laryngectomy was recognized as a safe, oncologically sound operation. Modern indications for total laryngectomy include late-stage tumors, specifically, T3 SCC, where supracricoid or supraglottic laryngectomy is not possible; T4 SCC, where supracricoid or near-total laryngectomy is not possible; and any tumor with invasion into the surrounding soft tissue of the neck, extensive involvement of the thyroid or cricoid cartilage, or extending beyond the posterior one-third of the tongue base. Also, it is indicated for patients with late-stage tumors in whom XRT alone or chemotherapy plus XRT are not possible for any reason.15 To perform a total laryngectomy, the surgeon removes the hyoid bone, thyroid and cricoid cartilages, and upper tracheal rings. The opening of the trachea is diverted to the skin of the neck, creating a permanent stoma for respiration. The arytenoid cartilages and interarytenoid tissue are removed, and the party wall is dissected free. The resulting pharyngeal defect is sutured closed in a layered fashion, thus completely separating the oropharynx from the airway. With removal of the entire larynx, the ability to produce the native voice is lost; however, vocal rehabilitation is possible and can allow for speech. Handheld devices such as the electrolarynx, learning the technique of esophageal speech wherein air is swallowed and expelled via the esophagus, neopharynx, and mouth to create sound, or surgical insertion of a tracheoesophageal prosthesis to allow for speech with the tracheostoma occluded are all possible. Patients may also choose to use writing for communication. Indications for vertical partial laryngectomy include early-stage SCC (T1 and T2) with a mobile contralateral cord, no cartilaginous involvement by tumor, no involvement of the body of the arytenoid by tumor, and maximum subglottic extension of 5 mm. This procedure can be performed via traditional open approach, or endoscopically for smaller lesions in a procedure termed endoscopic cordectomy using an operating microscope. In an open procedure, the thyroid cartilage is exposed and the perichondrium overlying the affected side of the larynx is elevated and preserved for use in closure. Using an oscillating saw, a vertical cut is made in the cartilage at the midline if there is no anterior commissure involvement by the tumor to be resected or on the contralateral side of the thyroid cartilage to allow for a 5 to 7 mm margin of uninvolved tissue if anterior commissure involvement is present. The entire ipsilateral supraglottis, excepting the epiglottis, is removed, and the ipsilateral arytenoid may be spared if uninvolved. The involved TVC, and anterior commissure, if uninvolved, is taken. If there is anterior commissure involvement, up to one-third of the contralateral TVC may be resected and good outcomes still achieved. The ipsilateral cricothyroid membrane and even a small amount of upper ipsilateral cricoid cartilage may also be resected if warranted (Fig. 14.2). Reconstruction of the tissue defect can be achieved by using local strap muscles or the epiglottis, and it often ultimately heals into a scarred band resembling a rudimentary vocal fold, sometimes referred to as a “neo-cord.” For endoscopic cordectomy, an operating laryngoscope is placed into the mouth to expose the larynx. Using the operating microscope and microlaryngeal instruments or a laser, the affected TVC is excised under direct visualization, taking with it a 5-mm cuff of normal surrounding mucosa. The specimen is then freed from the underlying cartilage, taking perichondrium. Ultimate outcomes include normal swallowing function, though many patients require some rehabilitation under the auspices of a speech and language pathologist for swallowing techniques. Vocal rehabilitation typically proceeds well, with most patients satisfied with their voice, which does tend to have a “breathy” quality. Indications for a supraglottic laryngectomy include tumors confined to the supraglottis, with no extension onto the TVCs and minimal medial pyriform sinus involvement above the TVCs. Indications also include supraglottic tumors that are T3 by way of preepiglottic space involvement only. Typically, both arytenoid cartilages are left in situ in supraglottic laryngectomy; however, select patients may tolerate resection of one arytenoid cartilage. All patients considered for this procedure must have good pulmonary reserve and cough reflex, as aspiration is frequent, and the ability to cough to clear secretions is paramount. Tissue removed in supraglottic laryngectomy includes the epiglottis, preepiglottic space, and upper portion of the thyroid cartilage down to the midpoint of the laryngeal ventricle, truly removing the entire supraglottis. The arytenoids and both TVCs are left intact (Fig. 14.2), allowing for normal voice postoperatively. The patient will need to be evaluated by a speech and language pathologist for safe swallowing techniques to minimize the risk of aspiration. This is an extension of the supraglottic laryngectomy, removing all the same structures as by that procedure, as well as one arytenoid cartilage and possibly some of the upper ipsilateral cridoid cartilage. One arytenoid and vocal cord must be left unresected (Fig. 14.2). This procedure is nearly always performed with concomitant cricohyoidopexy, wherein the cricoid cartilage is tethered to and suspended from the hyoid bone, elevating it for further protection from aspiration during deglutition. Indications for supracricoid laryngectomy are the same as for supraglottic laryngectomy, but also include T3 SCC because of unilateral TVC fixation, or very minimal invasion of the thyroid cartilage. As with supraglottic laryngectomy, patients need good pulmonary function and reserve to tolerate this procedure well, and they will likely require prolonged postoperative rehabilitation for speech and swallowing. Ultimate outcomes that can be expected are normal swallowing function and recovery of laryngeal speech, though voice quality may be poor. These patients often require prolonged tracheostomy, but they can be decannulated as rehabilitation progresses. Indications for this procedure include T3 and T4 SCC not amenable to supraglottic or supracricoid laryngectomy but with one uninvolved arytenoid and laryngeal ventricle, unilateral transglottic SCC with TVC fixation, or patients who would otherwise be candidates for supraglottic or supracricoid laryngectomy but have poor pulmonary reserve. Important contraindications are subglottic extension below the cricoids or salvage situations after XRT failure. In near-total laryngectomy, the entire supraglottis is removed bilaterally, together with the ipsilateral glottis and arytenoid cartilage, and resection can also include a portion of the ipsilateral upper cricoid cartilage. Patients are left with a single arytenoid and TVC and ultimately speak via a surgically created laryngoesophageal fistula. A permanent tracheostomy is left in place for respiration. Ultimately these patients can be expected to recover normal deglutition after rehabilitation in conjunction with a speech and language pathologist. In practice, this is a rarely performed procedure that is technically difficult and best reserved for those few practitioners with extensive experience in its use. XRT is a very important part of the treatment of head and neck cancers, including laryngeal SCC. There are a variety of methods to deliver ionizing radiation to tumors, but in the head and neck, external beam therapy predominates. In this technique, an externally located radiation source delivers a beam of radiation to a precise area of tissue, this being determined before treatment is begun based on clinical examination and radiographic imaging. XRT can be used as a solo treatment modality or can be combined with surgery or with chemotherapy, which will be discussed in further detail later in the chapter. When using XRT as a solo treatment of laryngeal SCC, it is necessary to define not only the precise areas to be irradiated that contain the primary tumor but also if the neck needs to be irradiated as well to control known or occult metastasis. As discussed previously, early-stage laryngeal SCC (T1 and T2) may be amenable to single modality treatment. Typically, the neck is included in the irradiated field if clinical evidence of metastasis is evident or if the risk of occult metastasis is felt to be 15% or greater. The total dose of radiation given is measured in Gray (Gy) and is based on the size of the tumor, as well as the tolerance of surrounding normal tissues to radiation exposure. Doses of 60 to 65 Gy are used for small, early-stage tumors of the larynx with control rates of greater than 90% reported, while 70 to 75 Gy are necessary for larger, T3 to T4 laryngeal SCC to achieve 90 to 100% local control rates.16 These doses are typically given in daily sessions over a period of 6 to 7 weeks, and complications such as mucositis or dermatitis may necessitate breaks in therapy, though too long a hiatus from treatment leads to a decrease in efficacy and ultimately poorer tumor control. More advanced, late-stage tumors are best treated with combined modality therapy, such as XRT plus surgery or XRT plus chemotherapy (discussed later). Local surgical failures in laryngeal SCC are often the result of microscopic residual disease intentionally (to avoid morbidity or mortality) or inadvertently left behind after primary surgical resection. XRT plays a role in eliminating such microscopic disease. Primary surgery with postoperative XRT facilitates the surgical resection and postoperative healing, as nonirradiated tissue heals far more effectively than does irradiated tissue. A larger total dose of radiation can be given postoperatively, and this dose can be adjusted based on the amount (if any) of obvious residual disease postresection. Disadvantages to this algorithm include the possibility of delay in commencing XRT if wound healing is slow or if surgical site infection occurs. Results of postoperative XRT are not as favorable if treatment is delayed 6 weeks or more postoperatively.17,18 Historically, chemotherapy was used for palliation in cases of unresectable or metastatic advanced laryngeal cancer. Currently, chemotherapy in laryngeal SCC is not used as a single-treatment modality when a cure of the disease is intended but is always combined with XRT. Indications for chemotherapy are locoregionally advanced, late-stage (T3 and T4) SCC. The most widely used chemotherapeutic agents are cisplatin and carboplatin, with cisplatin perhaps being slightly more efficacious but having a more severe side-effect profile as well. Schema for the use of chemotherapy broadly fall into three categories: (1) induction chemotherapy, wherein chemotherapy is given before definitive XRT or surgery, which is performed later; (2) concurrent chemotherapy plus XRT, wherein chemotherapy cycles are given during the patient’s ongoing XRT; and (3) adjuvant chemotherapy, wherein surgical resection is first performed and concurrent chemotherapy plus XRT are begun postoperatively. In 1991, the U.S. Department of Veterans Affairs Study Group conducted a large, randomized controlled trial (RCT) of 332 patients to determine whether induction chemotherapy with definitive XRT was more effective than total laryngectomy with postoperative XRT for stages 3 and 4 laryngeal SCC. Overall, survival rates between the control and experimental arms of the surgery were comparable, and 64% of the patients in the experimental arm of the study retained their larynx at 2-year posttreatment, the remaining 36% required salvage laryngectomy for residual or recurrent SCC.10 Factors associated with treatment failure were T4 disease and supraglottic primary site. Of note, the authors did mention in their study that chemotherapy plus XRT was not compared with XRT alone; therefore, some questions remained unanswered about the actual benefit of the chemotherapy. A similarly designed study sponsored by the European Organization for Research and Treatment of Cancer (EORTC) Cooperative Group, conducted in 1996, gave similar results. There was no difference in the overall 5-year survival between the two groups, and no direct comparison between chemotherapy plus XRT and XRT alone was made; the precise benefit of the induction chemotherapy remained somewhat in question.19 Of note, both these studies did suggest that the rate of distant metastasis may be slowed or decreased with the addition of chemotherapy, and further studies using other treatment schemes for chemotherapy were conducted. Based on the data described in the Veterans Affairs Laryngeal Study and the EORTC study, a prospective RCT was conducted in 2003 to compare XRT, induction chemotherapy plus XRT, and concurrent chemotherapy plus XRT in patients with stage 3 or 4 laryngeal SCC. The rate of larynx preservation was higher (84%) in patients receiving concurrent chemotherapy plus XRT than in either of the other two arms of the study.20 There was no significant difference in overall 5-year survival between any of the treatment groups, though rates of locoregional recurrence were lower at 2 years in the concurrent chemotherapy plus XRT group, as well as a decrease in the rate of distant metastasis in this same group at 5-year posttreatment. Other authors have reported similar findings, improving disease-free survival, not to be confused with overall survival, by 15 to 20% using concurrent chemotherapy plus XRT.21,22 Indications for adjuvant chemotherapy plus XRT after primary surgical resection in laryngeal SCC include positive surgical margins, perineural or perivascular invasion, extracapsular extension in cervical lymph node metastasis, or cervical nodal disease in level IV or V of the neck. All these are associated with higher local and locoregional recurrence rates. Two prospective RCTs addressed the efficacy of adjuvant chemotherapy plus XRT in locally advanced head and neck SCC, the Radiation Therapy Oncology Group Trial 9501 and the EORTC Trial 22931 in 2004. Subsequent combined analysis of the two similar trials found advantages in both locoregional control and overall survival in patients receiving adjuvant therapy.23 Adjuvant therapy is best used in patients with adverse clinical or histologic features and improves local control and disease-free survival, and it may improve overall survival as well. Clinical Pearls • Most true neoplasms of the adult larynx are malignant, and most of these are squamous cell carcinomas (SCCs). • Including surgical resection in the treatment of laryngeal SCC may increase long-term (> 5 years) survival. • Concurrent chemotherapy with radiation therapy (XRT) and adjuvant chemotherapy with XRT after surgical resection both improve overall survival. • Multiple options for voice rehabilitation exist after total laryngectomy.
Larynx and Laryngeal Neoplasms
Neoplasms
Benign
Papilloma
Malignant
Minor Salivary Gland Tumors
Neuroendocrine Tumors
Adenocarcinoma
Chondrosarcoma
Squamous Cell Carcinoma
Surgical Approaches
Total Laryngectomy
Vertical Partial Laryngectomy
Supraglottic Laryngectomy
Supracricoid Laryngectomy
Near-Total Laryngectomy
Radiation Therapy
Radiation Therapy as Solo Treatment
Radiation Therapy Combined with Surgery
Chemotherapy
Induction Chemotherapy
Concurrent Chemotherapy
Adjuvant Chemotherapy
Larynx and Laryngeal Neoplasms
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


