FIGURE 7.1 Three-Dimensional Effects of Posterior Cricoarytenoid Muscle Contraction.
(A) Sagittal view. (B) Posterior view. (From Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology—Head and Neck Surgery. 6th ed. Philadelphia, PA: Saunders; 2015, fig. 54-3.)
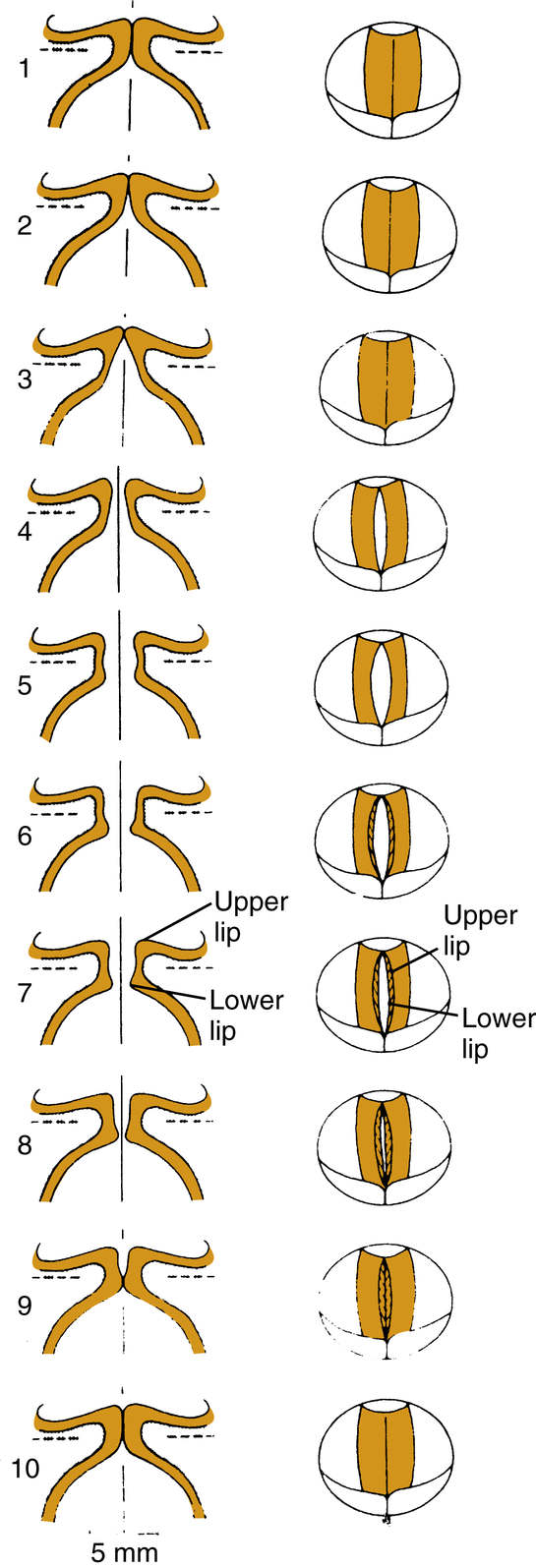
FIGURE 7.2 Movements of different portions of vocal folds during one cycle of vibration shown schematically in the coronal plane (left) and from above (right). Mucosal upheaval begins caudally (1) and then moves rostrally. The lower portion is closing as the upper margin is opening (5). (From Hirano M. Clinical Examination of Voice. New York, NY: Springer-Verlag; 1981; and Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology—Head and Neck Surgery. 6th ed. Philadelphia, PA: Saunders; 2015, fig. 54-11.)
• Thyroarytenoid muscle
• Perichondrium and thyroid cartilage provides the lateral boundary of the vocal fold (Fig. 7.3)
Visualization of the Larynx
Indirect Methods of Visualize the Larynx
1. Mirror laryngoscopy
2. Rigid indirect laryngoscopy
3. Flexible indirect laryngoscopy
Benefits of Rigid Indirect Laryngoscopy
1. Higher resolution
2. Brighter, clearer picture
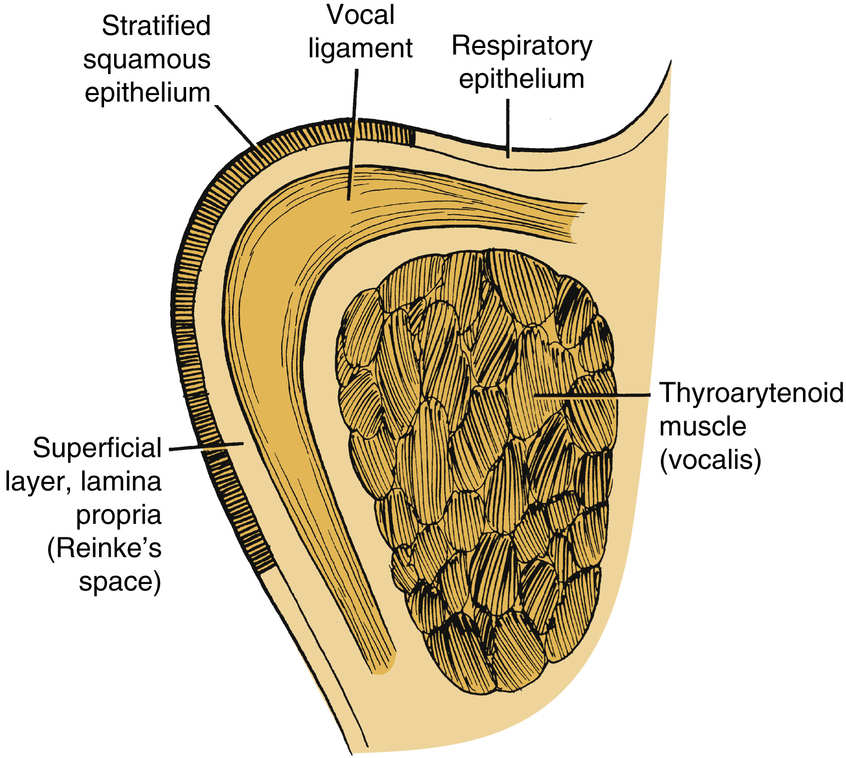
FIGURE 7.3 Cross Section of the Vocal Fold.
(From Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology—Head and Neck Surgery. 6th ed. Philadelphia, PA: Saunders; 2015, fig. 61-1.)
3. Image is more accurately magnified
4. Generally does not require topical anesthesia
Drawbacks of Rigid Indirect Laryngoscopy
1. Cannot visualize the larynx while patient performs complex speaking tasks
2. May be difficult to visualize arytenoid abduction/adduction in certain patients
Benefits of Flexible Indirect Laryngoscopy
1. Can visualize the larynx during speaking/singing tasks
2. The larynx is in a more natural configuration for neurological evaluation
Drawbacks of Flexible Indirect Laryngoscopy
1. Generally requires topical anesthesia
2. Distortion at the periphery of the image
3. Inferior light transport/magnification versus rigid
Key Structures and Finding to Be Evaluated with Laryngopharyngeal Endoscopy
1. Overall structure of vocal folds
• Bowed (atrophy)
• Scar/sulcus deformity
2. Masses or lesions
3. Abduction and adduction of true vocal folds
• Vocal fold paresis/paralysis
• Cricoarytenoid joint fixation
• Posterior glottic stenosis
4. Supraglottic configuration
• Relaxed: can see the whole vocal fold
• Asymmetric: may imply paresis or be seen with paralysis
• Symmetric: may be a normal variant or muscle tension dysphonia (MTD)
5. Pooling of secretions
• Vallecula: consider tongue-base weakness
• Piriform sinuses/postcricoid region
• Pharyngeal weakness
• Lack of sensation/neurologic deficit
• Esophageal obstruction: see the dysphagia/esophageal section
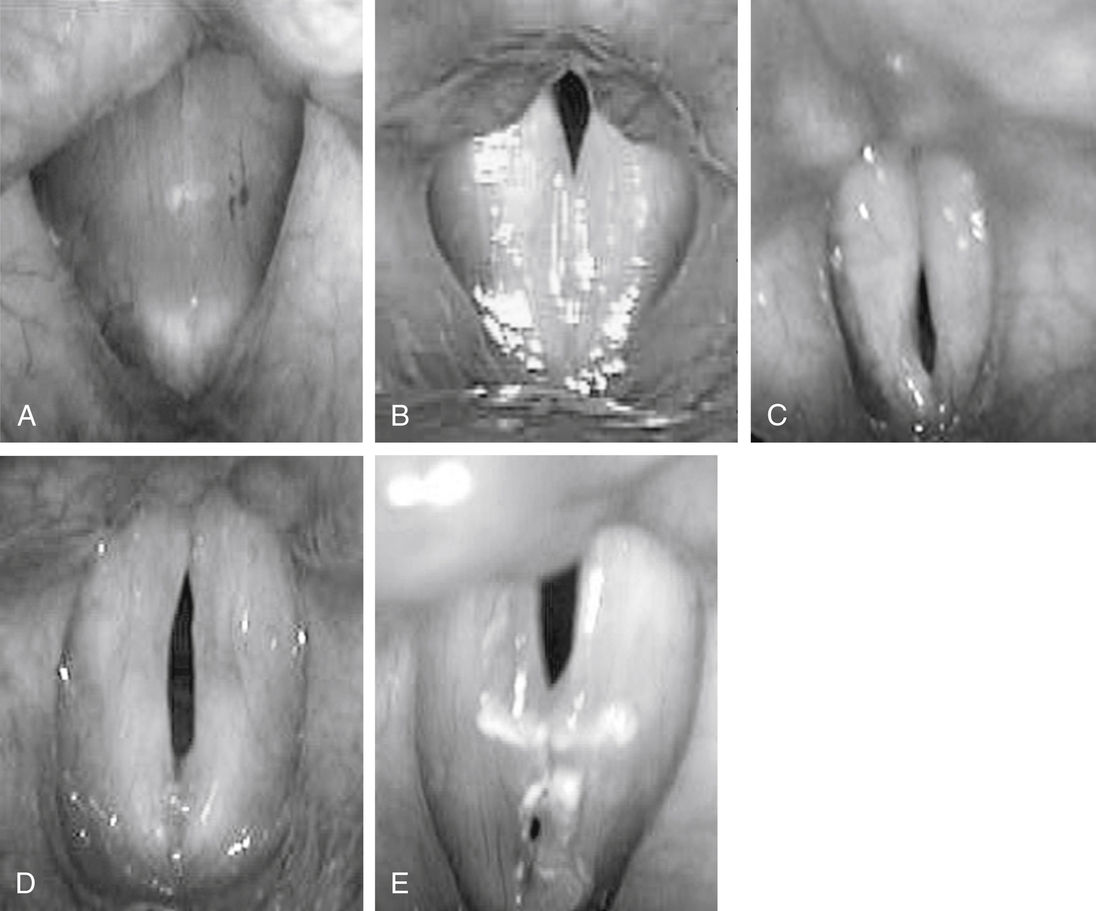
FIGURE 7.4 Glottal Closure and Gap Patterns.
(A) Complete closure. (B) Posterior glottal gap. (C) Anterior glottal gap. (D) Spindle-shaped gap. (E) Hourglass-shaped gap. (From Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology—Head and Neck Surgery. 6th ed. Philadelphia, PA: Saunders; 2015, fig. 55-3.)
Videostroboscopy Basics
• Used to assess vocal fold vibration
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


