13
Language Development in Children with Cochlear Implants
Amy McConkey Robbins
“Language is the light of the mind.” John Stuart Mill
This chapter addresses issues related to language development in children with cochlear implants. Language is more than the words we speak. It is a complex enabler. It allows us to participate, to understand, and to interact with the world around us. In short, it enables us to communicate (Froehlinger, 1981). Because language skills are essential for learning almost anything, those who are deficient in such skills face difficult challenges in many other aspects of achievement. Conversely, a well-developed language foundation provides the potential for success in other achievement areas. It is this potential for enhanced life achievement that cochlear implants offer to children with profound deafness.
A cochlear implant (CI) is not a cure for deafness, but it is a powerful technology that allows many profoundly deaf children to function as well as hard-of-hearing children (Blamey et al, 2001; Boothroyd and Eran, 1994; Boothroyd-Turner and Boothroyd, 1998; Eisenberg et al, 2004). Such a transformation greatly improves the chances of achieving high levels of speech perception, good language competence, intelligible speech, and the ability to succeed in a mainstream educational setting, to name a few. This transformation also allows a deaf child the possibility of developmental equivalences with hearing individuals, the outcome measure that health agencies seek as evidence for effectiveness of an intervention (Yoshinaga-Itano et al, 2004).
♦ Effects of Profound Deafness on Language Development
Early-onset profound hearing loss has been shown to have devastating consequences for the development of language. [For the purposes of this chapter, we confine our discussion to the development of English-language skills in spoken and signed forms. Although the issues regarding development of American Sign Language within a deaf culture context are important ones, they are beyond the scope of this chapter. The reader is referred to Curtiss (1989) for a review of this topic.] During the critical period for language learning, falling between birth and about 7 years of age, children with normal hearing master almost all of the essential elements required for being a competent communicator in their language. The presence of profound hearing loss dramatically alters children’s ability to extract linguistic cues from the auditory language models around them (Carney and Moeller, 1998). These children are also deprived of one of the primary sources of language information; that is, the linguistic models that are available during “overhearing” language via various sources in the environment are drastically reduced.
English-Language Achievement of Profoundly Deaf Children
Children with prelingual onset of profound deafness have been shown to experience substantial delays and deviances in their mastery of all aspects of communication including vocabulary (Boothroyd et al, 1991; Osberger et al, 1986) grammar (Geers and Moog, 1994; Power and Quigley, 1973), concepts (Davis, 1974), and pragmatics (Kretschmer and Kretschmer, 1994), in both the receptive and expressive domains. Over the past several decades, substantial advances in traditional hearing aid technology, tactile aid development, and teaching methodologies for children with profound hearing loss have taken place. Unfortunately, these advances have not translated into dramatic improvements in the overall language or academic attainment levels of deaf children. Remarkably similar language achievement levels have been documented by researchers studying children from a variety of educational settings and using different communication methodologies (Levitt et al, 1987; Moog and Geers, 1985; Osberger, 1986). Although much variability is seen across students, the average profoundly deaf child without a CI has been shown to acquire language at a rate that is approximately half of that expected from normal hearing children (Carney and Moeller, 1998; Osberger, 1986; Robbins et al, 1997).
The ability to read and write is based strongly on the foundation of language. Thus, delays in language resulting from hearing loss typically interfere with the child’s development of literacy skills. Many profoundly deaf children reach the end of high school having attained only third-grade reading levels (Holt et al, 1997), a factor that severely limits their options for postsecondary education and job placement. An economic analysis (Mohr et al, 2000) estimated that the average cost to society of an individual with prelingual severe to profound hearing loss exceeded $1 million over the lifetime of that individual. The authors concluded that “interventions aimed at children, such as early identification and/or aggressive medical intervention may have a substantial payback.”
The Cognitive-Linguistic Gap
Normally developing children acquire cognitive and linguistic skills concurrently wherein language milestones are intimately tied to cognitive ones. Deaf children typically acquire cognitive skills at a normal rate but are delayed in their acquisition of language, a phenomenon known as the cognitive-linguistic gap. This gap reflects the developmental asynchrony between nonverbal cognitive skills and linguistic skills in deaf children (Boothroyd, 1982). When a significant hearing loss exists, nonverbal cognitive skills emerge normally but linguistic development lags behind because of the sensory impairment. In other words, deaf children (excluding those with intellectual impairment) have the cognitive readiness to understand and use linguistic constructs, but the sensory deficit interferes with access to these constructs. This gap may actually work to the deaf child’s benefit in the following way. These children, although delayed in language, have more sophisticated nonverbal comprehension strategies and means of organizing their experiences than their language level indicates (Moeller and McConkey, 1984) (i.e., their language skills are more like those of younger children with normal hearing, whereas their cognitive skills are age-appropriate). This means that the deaf child can capitalize upon underlying knowledge of the world to accelerate language learning, provided the child gains access to the linguistic code. It is this linguistic access, and the best way to provide it, that is at the heart of the controversy surrounding communication methodologies for deaf children. Cochlear implants are allowing such linguistic access to many prelingually deaf children, providing a growing body of compelling evidence regarding the usefulness of these devices in the pediatric population.
♦ Benefits of Cochlear Implants for Language Development
Measuring Language Benefit in Children with Cochlear Implants
Aspects of Language Assessed
Language is a complex entity made up of two domains, comprehension and production; and many components, such as vocabulary, syntax, morphology, and pragmatics. Most research studies have investigated only one component at a time. Depending on the component(s) assessed, children with CIs may compare more or less favorably to their age peers with normal hearing. The component that has been studied most often in children with cochlear implants is single-word vocabulary comprehension. In normal-hearing children, vocabulary comprehension correlates strongly with verbal IQ. However, it is well documented that in children with hearing loss, an imperfect relationship exists between single-word vocabulary and overall language competence and that receptive vocabulary scores may over-or underestimate overall language skills in this population (Moeller et al, 1983). Moreover, single-word identification tasks give no insights into the child’s lexical organization or knowledge in context, both of which are skills essential to reading comprehension (Johnson et al, 1982). Assessments should include tests that more closely resemble real-world communication, most notably tests of connected language, not only single words.
In addition, some aspects of language, such as everyday use of grammatical elements, can only be judged adequately using a spontaneous language sample. Grammatical elements, such as finite morphemes (e.g., third person singular,–s; past tense,–ed,) are highly vulnerable in hearing children and persist longer than deficits in other language areas in children with specific language impairment (Goffman and Leonard, 2000; Rice et al, 1998). The same appears to be true for children with cochlear implants. Assessment of language competence can be best accomplished using a battery of language tests that sample many aspects of communication. If a single component of language has been tested, statements pertaining to performance should be limited to the skill actually assessed (i.e., vocabulary comprehension) and not extended to overall language competence.
Methods of Analysis
One of three measurements is generally employed in studies of language development. First, performance may be expressed as an age-equivalent score (or language age) if a test standardized on children with normal hearing is used to assess language skills. Second, language quotients are often utilized as the measurement technique. Age-equivalent scores are used to obtain this measurement. A language quotient is determined by dividing a child’s language age by his or her chronological age and multiplying by 100. A “normal” language quotient of 100 is obtained if language age is equivalent to chronological age. An advantage of using language quotients with implanted children is that one may observe the size of the gap between language and chronological age. Studies of implanted children utilizing language quotients measure this gap and assess if it is stable or closes over time.
A third approach to quantifying language development involves measurement of the rate of language change that occurs over a specified period of time following implantation. This approach provides information about the change measured in language skills relative to the period of time during which the change occurred. The absolute language levels of the children are not considered in this type of analysis. Rather, the goal is to observe the rate of language learning over time (Fig. 13–1). Some studies have utilized a combination of these analysis methods as a way of viewing the data from several perspectives.
Evidence from the Literature
In the last 5 years, there has been a dramatic increase in published investigations regarding the language of children using a CI. Variables often studied include effect of age at implantation, effect of communication mode, and comparison of the language of children with CIs to that of children with either normal hearing (NH) or hearing loss. A representative sample of studies is reviewed below.
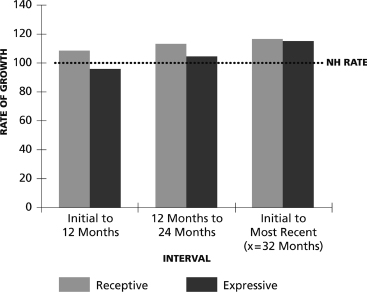
Figure 13–1 Average language learning rates on the Reynell Developmental Language Scales for 18 prelingually deafened children with Clarion (Advanced Bionics, Sylmar, CA) implants at three time intervals. Learning rate was calculated by dividing the change in language age equivalent scores at two intervals by the time between intervals and multiplying by 100. Calculations from the initial period were made from the time of initial stimulation. A normal-hearing child would make 12 months of progress in 12 months’ time, yielding a learning rate of 100, as noted by the horizontal line.
In the most comprehensive study to date, the performance of 181 prelingually deaf 8-and 9-year-olds who received a CI by age 5 was evaluated (Geers et al, 2003); 157 of the children had performance IQs within the average range and therefore were administered a battery of language measures. On several measures including those of verbal reasoning and narratives, more than half of the children exhibited language skills that were similar to age-matched peers with normal hearing. This proportion of profoundly deaf children scoring within the average range is a landmark finding and far exceeds those reported in previous studies of similar children using hearing aids. When language measures were examined separately for expressive and receptive tasks, there was no difference between students using oral communication (OC) and those using total communication (TC) on the receptive syntax measure, but a significant expressive language advantage for children from OC settings. A similar finding was reported by Kirk et al (2002), who evaluated language skills in 73 implanted children and compared results in: (1) children implanted before 3 years of age to those implanted at 3 years or older, and (2) children using OC to those using TC. The children who received implants before 3 years of age had significantly faster rates of language development than did the children with later implantation. In addition, among the early-implanted children, OC children were acquiring age-appropriate expressive language skills whereas TC children were not. Even after 4 years of CI use, the early-implanted TC children’s expressive language lagged behind their chronological age.
Hammes et al (2002) compared language development in 47 children implanted by 48 months of age. They found that children implanted under 18 months of age had substantially better language outcomes than those implanted after 18 months of age. The majority of the subjects used TC prior to implantation, yet a strong shift to spoken language was observed after implantation, depending on age at CI. All of the children implanted under 18 months of age made successful transitions to spoken language. As age at implantation increased, fewer and fewer children became competent users of spoken language. In fact, of 22 children who received their CI between 31 and 48 months, more than half remained dependent on sign language, even after 9 years of implant use. This study also looked at the differential effects of early identification/intervention and early implantation. Even among children identified, aided, and enrolled in intervention prior to 6 months of age, those who received implants earlier out-performed the early-identified, later-implanted children. This important finding suggests that although early identification and intervention are necessary, they are probably insufficient alone in producing children with age-appropriate, intelligible spoken language.
Blamey et al (2001) studied a group of 87 children with hearing loss, including 47 with cochlear implants, using single-word vocabulary Peabody Picture Vocabulary Test (PPVT) and Clinical Evaluation of Language Fundamentals (CELF) tests. The average rate of language improvement (0.56 to 0.63) was considerably less than the rate reported by several other investigators (Bollard et al, 1999; Dawson et al, 1995; Miyamoto et al, 1997; Robbins et al, 1997). Some children in the Blamey et al (2001) study had received their CI at ages as late as 8 years, a factor that likely accounts for the slower rate of language growth.
Connor and Zwolan (2004) found that in 91 children who had received cochlear implants, earlier age at implantation was positively correlated with higher reading scores when the children were school-aged. Preimplant mode of communication (OC or TC) was not correlated with reading outcomes in this study.
Superior grammatical skill development was documented in children implanted by age 3 versus at age 4 years or older by Nikolopoulos et al (2004). Svirsky et al (2004) found that implantation before the age of 2 resulted in higher speech perception and language scores. Using a single-subject design, Miyamoto et al (2003) obtained language scores from a subject implanted at 6 months of age. The child’s language scores at 2 years of age were nearly equivalent to those achieved at the age of 5.5 years by children implanted at later ages.
Studies have found a positive effect of early implantation even on prelinguistic communication behaviors. Houston et al (2003) used the Preferential Looking Paradigm (PLP) to assess the pre–word-learning skills of infants and toddlers who either had normal hearing or a cochlear implant. Children implanted between 7 and 15 months of age performed similarly to the children with normal hearing after 2 to 6 months of CI experience. In contrast, children who received their implants at later ages (16 to 25 months of age) did not demonstrate learning of the associations within the context of the study. The authors emphasize the possible role of intersensory redundancy, that is, that babies with normal hearing are exposed to language from birth, receiving combined auditory and visual input. Evidence suggests that early auditory deprivation impairs the development of neural pathways connecting the auditory cortex to other cortices (Kral et al, 2000; Ponton & Eggermont, 2001). Later age at implantation delays the onset of auditory input and, therefore, of neural pathway development.
Another study of early communication behaviors compared infants and toddlers who received a CI at the age of 12 to 18 months, 19 to 23 months, or 24 to 36 months (Robbins et al, 2004c). The children also were divided into three groups based on age at CI: 12 to 18 months (n = 45), 19 to 23 months (n = 23), and 24 to 36 months (n = 30). Scores from the Infant-Toddler Meaningful Auditory Integration Scale (IT-MAIS), a parent interview schedule (Zimmerman-Phillips et al, 2001), were compared with the normative IT-MAIS scores reported by Kishon-Rabin et al (2001). The most impressive gains were demonstrated by the children implanted between 12 and 18 months of age. Over half of the children in the youngest age group achieved auditory milestones approximating those of hearing peers after only 6 months of device use. For the children implanted between 19 and 23 months, only about one fourth attained scores within the broad normal range after 6 months of device use. Although they showed impressive progress with their CI, only a handful of children implanted between 24 and 36 months achieved scores comparable to their peers with normal hearing at the 6-month follow-up visit. Based on these data, a child’s IT-MAIS score may be assigned a NH age equivalent score (Table 13–1).
| IT-MAIS Score (% correct) | NH Age Equivalent |
| 10% | 1 month |
| 20% | 2 months |
| 30% | 3 months |
| 40% | 4.5 months |
| 50% | 6 months |
| 60% | 7.5 months |
| 70% | 10 months |
| 80% | 13 months |
| 90% | 17 months |
| 100% | 26 months |
The studies cited above provide research evidence regarding the effects of cochlear implants on communication development in children. Several findings characterize the results of these studies.
Earlier Age at Implantation Results in Superior Language Benefit
The trend for better performance in children implanted younger also has been documented in speech perception and speech production studies (see Chapters 12 and 14). Many factors favor early age at implantation, including neural plasticity and the notion of critical periods. Researchers have used the latency of the P1 cortical auditory evoked potential as a measure of the maturity and function of central auditory pathways (Sharma et al, 2002) and found that children implanted at 3.5 years or younger show age-appropriate latency responses within 6 months of implantation. The authors concluded, “In the absence of normal stimulation there is a sensitive period of about 3.5 years during which the human central auditory system remains maximally plastic.”
There is also an additive effect of early implantation and superior speech processing strategies. In one study that failed to find a significant advantage for children implanted at age 3 or younger (Geers, 2004), the author acknowledged the possibility that less sophisticated speech processing schemes used by the earliest implanted children may have provided insufficient auditory input during the early period of device use. When two powerful influences come together, that is, state-of-the-art technology and early age at implantation, the language benefit derived by deaf children is unparalleled. Another potent force that must be factored in is the ability of younger children to learn language incidentally, a topic addressed later in this chapter.
Children with Cochlear Implants Outperform Their Profoundly Deaf Peers Who Use Hearing Aids
In studies comparing the language performance of implanted children to that of their nonimplanted peers with profound hearing loss, faster rates of language learning and higher overall language achievement levels have been seen in the implant subjects (Geers and Moog, 1994; Robbins et al, 1997; Tomblin et al, 1999). The average profoundly deaf child learns language at about half the rate of normal-hearing children (i.e., 6 months of language in 1 year’s time) (Svirsky et al, 2000).
Cochlear Implants Allow Many Deaf Children to Begin to Learn Language at a Rate Equivalent to that of Normal-Hearing Children
Several studies, including Robbins (2003b), have demonstrated that the average child who receives a CI learns approximately 1 year of language in 1 year’s time (Fig. 13–1). This effect seems to be particularly true for those implanted in the first 2 years of life. Recall that, while the average child with CI demonstrates a normal learning rate, some children with CI demonstrate more than 1 year of growth in a year’s time, whereas others demonstrate a considerably slower rate of language growth.
Many Children Remain Delayed in Their Language Skills Even After Implantation
This finding appears to be the case largely because of the significant delays that already exist in children’s language at the time they receive their implants, as shown in (Fig. 13–2) (Robbins, 2003b). To avoid this continued delay, children must either learn language at a faster-than-normal rate after implantation to “catch up” to their hearing peers (Bollard et al, 1999), as some appear to be doing (see Fig. 13–3 for one subject’s data from Robbins, 2003b), or must receive their implants early enough to prevent a unclosable gap from forming between language age and chronological age. In addition, up to 40% of deaf children have additional developmental or learning disabilities (Parrish & Roush, 2004; Yoshinaga-Itano et al, 1998). Among that group, a rate of language development equivalent to that of NH children would be the exception, rather than the rule.
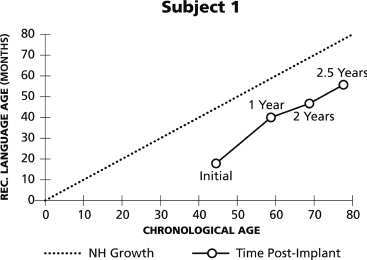
Figure 13–2 Individual Reynell data for one subject wearing the Clarion implant. Chronological age is plotted against receptive (Rec.) language age at each test interval. The dotted diagonal line represents language growth expected from a normal-hearing (NH) child; that is, the change in chronological age equals the change in language age. The gap between this child’s language and that of normal-hearing peers has not closed over time.
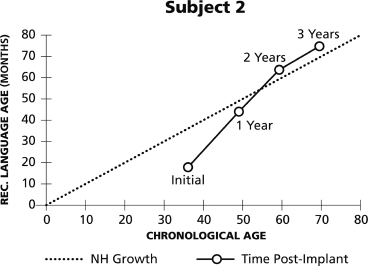
Figure 13–3 Individual Reynell data for one subject wearing the Clarion implant. Chronological age is plotted against receptive (Rec.) language age at each test interval. The dotted diagonal line represents language growth expected from a normal-hearing child; that is, the change in chronological age equals the change in language age. This child has learned language at a faster-than-normal rate since implantation, allowing the gap between his language and that of normal-hearing peers to close.
A Wide Range of Language Benefit Is Observed Across Children
Virtually every study of the performance of implanted patients, whether adults or children, has yielded a wide range of performance outcomes. The studies of language enhancement in this population are no exception (Spencer et al, 2003). The attempt to tease out what factors might account for this variability is ongoing. It is important to keep this large performance variance in mind, especially when reviewing data that have been averaged across subjects.
Morphosyntactic Development, Particularly in Expressive Language, Lags Behind Other Language Skills in Children with Cochlear Implants
Even in children with CIs whose comprehension of language is age-appropriate, expressive use of morphological markers is often delayed (Geers et al, 2003; Kirk et al, 2002; Nikolopoulos et al, 2004; Tomblin et al, 1999). Difficulties with these markers also persist longer than deficits in other language areas in NH children with specific language impairment (Goffman and Leonard, 2000; Rice et al, 1998).
Both Oral-and Total-Communication Children Improve in Their Language Skills After Implantation, but Oral-Communication Children Outperform Total-Communication Children on Most Expressive Language Skills
When some aspects of language are assessed, OC and TC children have demonstrated equivalent language benefit from the CI (Connor et al, 2000; Robbins et al, 2000). However, enhanced benefit to OC children becomes apparent when certain aspects of language are assessed. Many implanted children who use OC separate from their TC counterparts when morphosyntactic aspects of language are assessed, including use of bound morphemes, utterance length, and narrative form. Geers et al (2003) found no significant differences in language comprehension or verbal reasoning between the scores of children who were in OC educational programs and those in TC programs. Implanted children in OC programs outperformed their TC counterparts when spontaneous language samples were analyzed for lexical diversity, use of bound morphemes, utterance length, syntactic complexity, and use of the narrative form. These advantages were apparent whether or not the children were credited with signed productions in addition to spoken language.
♦ Mechanisms by Which Cochlear Implants Improve Language in Prelingually Deaf Children
The investigations cited before confirm that cochlear implants provide measurable language enhancement to children, particularly young children, who receive them. What is less certain is the mechanism by which this enhancement takes place. At the present time, one can only hypothesize about the nature of these mechanisms.
Access to the Spoken Language Code
For a profoundly deaf child with limited hearing aid (HA) benefit, more of the cues necessary to interpret the spoken language code are available via a CI than via HAs. Even the best CI users, however, do not hear normally; the signal they receive is degraded. Still, state-of-the-art CIs provide a rich enough signal to give “linguistic access” in many of the children who receive them. Data from studies cited earlier confirm that congenitally deaf children are able to learn spoken language via information from their CI.
Use of Audition to Monitor One’s Environment
Most profoundly deaf children without a CI do not have adequate residual hearing to use audition as a way of monitoring their environment. This means they must periodically look up from the task at hand to monitor their surroundings. For a student in a classroom, this means that his attention to the book in front of him or the arithmetic problem on the board is interrupted as the child looks around, then returns to the task at hand. If the CI allowed the child to develop a listening mechanism for monitoring his environment, the child could concentrate on his work while processing auditory signals around him (i.e., “That is the sound of the water fountain at the back of the room; that is the sound of someone throwing paper in the wastebasket. I can ignore those sounds”).
Ability to Cue into a Speaker
Children with hearing loss who use speech reading often miss the first parts of sentences spoken by others in conversation. This occurs because they are not visually cued into the speaker as he or she begins to talk. Anecdotal reports suggest that the CI ameliorates this problem because listeners are immediately aware when someone is speaking and can direct visual attention to that speaker. This means that, rather than processing only the second half of a message, the CI user has full access to the whole conversation, even if the user relies heavily on speech reading for language comprehension.
Potential for Incidental Language Learning
Incidental language learning is the avenue by which a child with normal hearing learns language. It occurs when (1) the child has adequate (not necessarily perfect) access to the speech code of the language and (2) what is heard takes on meaning. Traditionally, auditory language learning in deaf children was viewed as a process of auditory training. The approach mandated that the child be didactically trained to achieve each of the listening skills along the hierarchy of auditory development. This approach was based on the assumption that whatever the child needed to learn would have to be directly taught. This was not an unreasonable assumption prior to the advent of CIs, because many profoundly deaf children received only minimal auditory cues or patterns through their hearing aids. These pattern perceivers did not hear enough of the auditory code to use listening as their primary source of linguistic input. In order for these children to learn spoken language a direct, systematic approach to training was required. As one textbook advised, “It is important to remember as we work with hearing-impaired children that language skills need to be overtly learned” (Froehlinger, 1981). Deaf children were, in large part, unable to make use of incidental learning, such as through the overhearing of conversation, as a means of acquiring language. Incidental learning is the most efficient and perhaps the only way to truly master a spoken language code.
Even with the improved signal provided by the CI, children require intervention to develop age-appropriate language skills, but the focus of that intervention must take into account the child’s enormous potential for learning language incidentally. If teachers assume that a CI child’s learning is completely dependent on didactic instruction, many opportunities for incidental learning will be lost. In addition, failure to adopt an emphasis on incidental learning lessens the effectiveness of parents to utilize “teachable moments” at home to foster their child’s communication development.
A child’s potential for incidental learning and generalization is greatest in the early years and slowly decreases with age. All things being equal, the younger the child at the time of implantation, the greater the influence of incidental language learning. Conversely, the older the child at the time of implantation, the greater the need for didactic instruction to foster language development. Although children who are older at the time of implantation may still benefit from incidental learning, it is likely that their curriculum will need to be heavily weighted with didactic instruction if they are to learn new skills at an adequate rate.
♦ Clinical Management of Language Skills in Children with Cochlear Implants
Four issues regarding the clinical management of language skills in children with CIs are presented in this section. These are the selection of assessment tools, principles for developing language, birth-to-age-3 interventions in natural environments, and special populations of implanted children.
Selecting Tools for Measuring Language Skills
Establishing a baseline of English-language skills preoperatively and monitoring ongoing development after implantation are vital to assessing implant benefit and making appropriate educational recommendations for implanted children. The purpose of assessing language is to reveal the child’s underlying competence in abstract linguistic knowledge (in our case, English). For this reason, it is typical to assess a child’s language in his or her preferred communication mode, which may include spoken English alone, simultaneous spoken and signed English, or spoken English and cued speech. For a child using total communication, such an assessment yields information about underlying language abilities, not necessarily spoken language. It is also important to assess spoken language in every child with a CI, even those who typically communicate with signs, because spoken language skills are predictors of device benefit and impact decisions such as educational inclusion. Both formal and informal assessment procedures are useful when evaluating the language skills of implanted children. Recommended procedures and rationales for their use are found in the following subsection. Clinicians may also use the criterion-referenced red flag procedure to identify children who are making slower-than-average progress after implantation (Table 13–2). These red flags are based on data from published studies and reflect average performance for three different groups of children based on preimplant characteristics (Robbins, 2005).
Formal Assessment Procedures
A battery of language tests is recommended that sample communication behaviors across several subskills in the most time-efficient way. Receptive and expressive language skills should be evaluated independently, rather than inferred from one another. Tests should sample the broad areas of vocabulary, connected language, grammar, concepts, and pragmatics. The tests listed in (Table 13–3) meet several important assessment criteria: (1) they provide normative data for comparison to hearing peers; (2) they are relatively brief to administer; (3) they can be used with a broad age range of children, an important factor when performing longitudinal assessments; and (4) they have all been used with deaf children and found to be appropriate for this population (Moeller et al, 1983; Osberger, 1986; Waltzman et al, 2003). A spontaneous language sample has always been an important part of a test battery and recent studies of children with CIs (Geers et al, 2003), which suggests that spontaneous samples identify morpho-syntactic weaknesses that are not revealed by other tests.
| Full-time implant use not accomplished 1 month after initial activation |
| No change in quality or quantity of vocalizations after 3 months of device use |
| Child not spontaneously alerting to own name 25% of time after 3 months of device use |
| Child not spontaneously alerting to own name 50% of time after 6 months of device use |
| Lack of spontaneous alerting to some environmental sounds 6 months postactivation |
| Skills from audiological testing not observed in everyday settings after 9 months of use |
| No evidence of meaning being derived from sound after 12 months of device use |
| Major improvement in language not observed after 12 months of device use |
As infants and toddlers receive CIs with greater frequency, communication assessment remains vital for children at the prelinguistic stage, as revealed in findings by Kane et al (2004). These investigators correlated preimplant Communication and Symbolic Behavior Scales (CSBS) scores with postimplant Reynell scores in a group of early-implanted children. Results suggested that very low performance on the CSBS preimplant was a red flag for low Reynell scores after 2 years of device use. Preliminary results suggest that if children lack appropriate prelinguistic behaviors, the development of age-appropriate formal language is at risk.
If time permits, an assessment of pragmatics and verbal problem solving reveals how the child uses language to “put it all together.” Suggestions include the Test of Problem Solving and the Preschool Language Assessment Instrument, both for problem solving and conversational pragmatics.
Informal Assessment Procedures
Informal testing allows the clinician to vary the difficulty, length, and complexity of language input to assess the child’s ability to handle linguistic information. In this regard, informal procedures are akin to diagnostic teaching, which allows the clinician not just to assign a “pass” or “fail” to a test item, but to determine what methods work best with a child. Some formal tests identify primarily what the child cannot do, whereas informal procedures permit the flexibility to explore what the child can do, and under what conditions. Both are needed to paint a complete picture of the child’s communicative competence. Robbins (2000) provides suggestions for informal procedures with children wearing a CI.
| Test Instrument | Skill Assessed |
| Receptive Language | |
| CSBS | Pre- and early-communication behaviors |
| MacArthur Communicative Inventories | Single-word vocabulary and word combinations |
| Peabody Picture Vocabulary Test (PPVT) | Single-word vocabulary |
| Reynell Developmental Language Scales (RDLS) | Connected language |
| Test of Language Development (TOLD-P) | |
| Grammatic Understanding subtest | Syntax and morphology |
| Oral and Written Language Scales (OWLS) | Concepts and grammar; connected language |
| Expressive Language | |
| CSBS | Pre- and early-communication behaviors |
| MacArthur Communicative Inventories | Expressive vocabulary and word combinations |
| Woodcock-Johnson Psychoeducational Battery | |
| Picture Vocabulary subtest | Single-word vocabulary |
| Antonyms-Synonyms subtest | Concepts; “thinking with language” |
| Analogies subtest | |
| Reynell Developmental Language Scales | Connected language |
| Spontaneous Language Sample* | Syntax and morphology |
| Oral and Written Language Scales (OWLS) | Grammar, vocabulary, idioms, pragmatics |
*Analyzed formally using D.S.S., LARSP, IPSyn, etc., to evaluate structural complexity. Continuum of Auditory Skill Development
Principles for Developing Language in Children with Cochlear Implants
This section contains suggestions for the design of language learning programs for implanted children. Rather than being a prescribed curriculum, the following principles may be incorporated into an existing language program.
Establish a Foundation for Generalization Learning in the Early Stages of Implant Use
The foundation for establishing generalization and utilizing incidental learning should be built from the earliest days of cochlear implant use and embedded in the therapy program. The first weeks and months of device use are critical in establishing either a pattern that encourages generalization or one that emphasizes isolated training that may lead to “greenhoused” communication skills (Robbins, 2000). A model for building such a foundation is found in Robbins and Kirk (1996). The model includes using communication sabotage, teaching the child to recognize and label the absence of sound, and emphasizing name recognition. Even at the earliest stages of implant use, the emphasis is placed on behaviors that have relevance to real-world communication.
Emphasize the Suprasegmental Patterns of Spoken Language
Most children are delayed in language at the time they receive their CI, creating a sense of urgency to make up for lost time and close the language gap. Some parents and clinicians concentrate too heavily on single-word productions to close the gap, ignoring the vital role that suprasegmentals play in language development. “But affect is information and prosody conveys” (Locke, 1993). During the first year of life, an NH infant latches onto suprasegmental features in the parents’ speech: the prosody and intonation that communicate feelings and intentions. Via cues from a human voice, the listener knows the speaker’s identity (we are revealed through our voiceprint), his emotional state (is the speaker happy, worried, angry?), and the speaker’s intent (is he telling me something, asking me something, commanding that I do something?) all before factoring in the linguistic content of the words and grammar. Cues about speaker identity, emotional state, and speaker intent are well transmitted by the CI, meaning that the early-implanted child can learn communication intent and linguistic correctness as a gestalt, just as NH babies do (Robbins, 2003a).
Help All Implanted Children, Whether Oral-or Total-Communication, Move as Far Along the Auditory Continuum as Possible
The way language is organized and processed by deaf children falls along a continuum from fully visual to fully auditory. Most CI children are somewhere in between these two, relying both on auditory and visual cues during communication interaction. Our goal in language instruction with CI children is to move each child as far down the auditory continuum as possible for that child. How far down the continuum a given child moves is dependent on many factors, including age at implantation; etiology of deafness; presence of additional handicaps; parental support; educational environment; and x-factors (Head, 1983), which are the characteristics unique to each child, including temperament, tolerance for frustration, personality traits, and internal motivation to master tasks. Many of these factors, perhaps most of them, might be internally operating and not amenable to change. After implantation, some children may become almost completely auditory, relying on visual cues only in extremely noisy situations, whereas others remain highly dependent on vision to augment what they hear.
It should not be assumed that every child who uses TC prior to implantation will remain a visual learner after implantation. TC children can move far down the auditory continuum, but generally require radical changes in their educational programs and in parent expectations for listening and speaking skills to do so (Robbins, 1998a). Even if a TC child remains primarily a visual learner following implantation, the contributions that auditory input can make to his language development are profoundly important, provided the child learns to derive meaning from this input. There is ample clinical evidence to suggest that a child who is given an implant and then placed in a home or school environment where audition and speech are not valued, worked on, or naturally reinforced will demonstrate very little benefit from his implant in real-world communication situations. Successful children with implants may be found in both OC and TC settings. However, it is clear that an environment that emphasizes listening and speaking development is mandatory if children are to receive maximum benefit from the device. Cochlear implants have the potential to dramatically improve a deaf child’s ability to perceive spoken language and to speak intelligibly. If those two skills are not essential goals within an educational program, it is considered an inappropriate placement for an implanted child. For teaching suggestions related to language development in children using TC, see Robbins (1998a).
Set Both Spontaneous and Structured Language Goals
The tendency is to set goals only for behaviors that the child must demonstrate during structured learning times. Goals for spontaneous use of language define specific communication behaviors that the clinician expects to observe when the child is not in a structured setting, but rather is conversing with the teacher or with a peer. It is important to give parents homework activities that emphasize carryover of language skills learned at school to everyday situations at home.
Comment to Children as Much as You Question
Analyses of language interactions between adults and children with hearing loss reveal an overuse of commands and questions directed at children. Blank and Marquis (1987), in their conversational training program for young children, urge clinicians to recognize the vital importance of comments in conversation. The clinician who makes relevant comments that are at the child’s language level provides natural language models to the child, teaches the child about facts (“pumpkins are orange”) versus opinions (“pumpkin ice cream is better than vanilla ice cream”), and demonstrates one of the most important functions of language: sharing thoughts and feelings. By their very nature, comments leave a conversational space for communication turn-taking and elicit longer responses than “Yes-No” or “Wh” questions do. These skills, falling under the rubric of pragmatics, are sometimes mentioned by parents and teachers as being underdeveloped in children with CIs.
Use “Thinking While Listening” Techniques to Interweave Auditory and Language Activities
Auditory and language activities may be interwoven to “double your money” during lessons. Listening and language are not viewed as separate tasks but as interrelated components of communication. The “thinking while listening” approach (Robbins, 1998b) uses many traditional auditory techniques but introduces a twist to make them more meaningful and less predictable.
Monitor Children’s Progress in Language
A program should establish milestones for language behaviors that are expected to emerge in children at specific postimplant intervals. Noticeable changes in communication should be seen after 3 months of CI use. In children implanted by 36 months of age, data have been used to establish first-year auditory milestones that are precursors to spoken language proficiency (Table 13–3). Extensive post-CI communication benchmarks are also found in McClatchie and Therres (2003). Although children vary in the patterns of development, programs should have preestablished “red flags” for children who are not progressing appropriately. The clinician should keep a watchful eye on how well the chosen methodology works for a given child. If progress is not occurring, the teachers and parents should meet and discuss strategies. Given the research results that show the average implanted child learning 1 year of language in 1 year’s time, clinicians and teachers must be concerned about a child whose language progress is significantly slower than this. If limited progress is made after 6 months, something different should be tried. This may mean a host of different things for different children, but the goal is to explore other avenues for accelerating language learning.
Clinicians should record the positive changes occurring in a child’s language by using videotaping, testing, or spontaneous language sampling. It is helpful to document instances in which the child repeats something he has overheard in conversation, uses a new word without being directly taught it, or re-auditorizes by “thinking aloud” with language to problem-solve. All of these suggest that the forces of generalization and incidental learning are actively present in the child with a cochlear implant.
Early Intervention (Birth to Age 3) in “Natural Environments”
Implantation within the first months or years of life provides the baby with auditory access to the world at a point in development that is relatively close to that experienced by the normal-hearing infant. This, theoretically, could prevent the effects of developmental asynchrony and the often-seen gap between chronological age and language age observed in children with profound hearing loss.
We approach intervention with implanted babies with the assumption that a significant part of their language will be acquired incidentally, via natural interactions with their parents in a reinforcing environment, overhearing of conversations not spoken directly to them, and in playtime with other children. When working with implanted infants and toddlers who have no additional handicaps, the therapist’s job is largely one of facilitation rather than rehabilitation of language. This facilitation is not conducted haphazardly, however, but with a purposeful, goal-oriented approach. The notion of “natural environments” for CI children has been misinterpreted to mean therapy that always occurs in the child’s home. In fact, children with CIs, whose intervention focus is highly auditory, often should receive intervention in a clinic setting for the following reasons: (1) the clinician must be able to control the auditory environment during intervention, an unattainable task in many homes; (2) equipment (karaoke machine, piano, doorbell) that is essential for intervention is impractical or impossible to transport; (3) only a small number of clinicians are trained to work with this population and time spent traveling results in fewer children having access to a specialized therapist; and (4) a “natural environment” for babies is wherever their parents are, not a specific physical location. That being said, intervention should always be directed at helping parents facilitate communication in everyday settings, as outlined by Estabrooks (1998), Robbins (2003a), Rossi (2003), and Sindrey (2002).
Special Populations of Children with Cochlear Implants
As the criteria for implantation have expanded broadly over the past decade, more children with special needs are receiving these devices and require special considerations. Three such populations are multiply disabled deaf children (MD/D), children exposed to multiple languages, and children with auditory neuropathy/dyssynchrony (AN/AD).
Children with Multiple Disabilities
It has been estimated that ˜40% of deaf children have one or more additional disabilities (Parrish & Roush, 2004). In the Colorado statewide population of deaf children ages birth to 3 years (Yoshinaga-Itano et al, 1998), between 41% and 47% were reported to have one or more additional disabilities. It is possible that the number of MD/D children is increasing, due largely to higher rates of premature babies from the neonatal intensive care unit (NICU) who survive but are left with significant impairments. Recent studies (Donaldson et al, 2004; Holt and Kirk, 2005; Waltzman et al, 2000) suggest that many MD/D children show benefit from the cochlear implant, although progress is delayed relative to that of typical deaf children. The severity of the delay is typically consistent with the severity of the additional disability. Not every child with MD/D benefits from a CI.
Some clinical guidelines when working with the MD/D population include the following. Evaluate each child individually in the CI candidacy phase. The team should consider what environmental, cognitive, and social value a CI might have for the child, even if the benefit is less than expected. The team also should consider the cost to the family and child if the implant does not enhance the child’s quality of life. Exploring parental expectations is critical.
Determine to what degree the child makes use of the sensory information he already has. To the extent that the child uses touch, taste, vision, and other sensory systems to figure out the world, this bodes well for his ability to utilize auditory information from the implant.
For a significantly disabled child, consider a trial diagnostic period with a tactile aid to determine if the child will accept wearing a device and can make associations between sensory input and meaning. Post-CI, evaluate the progress of CI children with severe disabilities in comparison to themselves and from the standpoint of improved quality of life.
A team approach for the MD/D child is essential. Learn from and educate the other specialists working with the child. They have expertise in areas that can be of great value to the implant clinician. Often, other specialists’ knowledge of the benefit of auditory input is limited, and they require modeling to see how to incorporate listening and speaking into developmental activities. In addition, implant teams should not consider implanting MD/D children until the team gains experience with a large number of typically developing deaf children.
Multilingual (ML) and English as a Second Language (ESL) Families
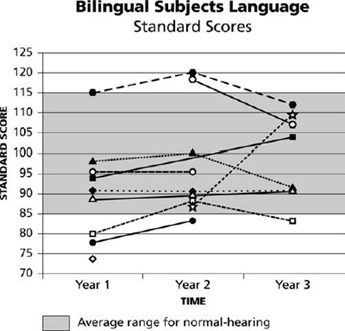
Children exposed to multiple spoken languages fall into one of two subgroups, ML or ESL, that require very different clinical management techniques. The ML group is made up of families in which parents are fluent in both English and another language. Children from such homes who have implants are exposed to fluent and sophisticated models of two languages and often attend schools, social events, and houses of worship where the second language is spoken fluently. Recent studies have yielded encouraging outcomes in both languages for children in this subgroup (Robbins et al, 2004a; Waltzman et al, 2003). It should be noted that the children in these studies were all implanted early (usually before age 2), and had excellent speech perception scores and no other significant disabilities (Fig. 13–4).
The high language proficiency of CI children from ML families is also related to two important factors: the rich and complex models of language provided by fluent speakers and the ability of ML parents to navigate the medical and educational systems, serving as informed advocates for their children. These factors are not present in the second group of CI children, those from ESL families. The clinical management of children from ESL families, therefore, is more complex and requires a concerted effort on the part of the CI team. It is widely acknowledged that a parent’s English-language proficiency by itself is not considered a selection criterion for a deaf child. On the other hand, family support is still considered an essential component of successful implantation for ESL children, as it is for any CI candidate. As always, the CI team must ensure that the family has appropriate expectations from the implant, can secure the child’s full-time use of the device, is comfortable with and able to troubleshoot the equipment, and can learn home carryover of speech, auditory, and language goals. In fact, the latter is absolutely essential for ESL families. For parents with limited English ability, an interpreter ideally should be available during clinic visits. At minimum, an interpreter must be present during preimplant candidacy discussions to ensure that the family has reasonable understanding of and expectations for the implant and to translate parent questions and concerns posed to clinicians. The team should also advise the family members that they play the most important role in their child’s success with the implant and must learn language stimulation techniques to use at home in their first language. Parents who speak limited English should not be advised to speak English to their deaf child, as the parents will be unable to provide rich, natural, and intelligible models of language in English (Sussman & Lopez-Holzman, 2001). Parent–child therapy time should be spent modeling techniques to the parent using English so that the parents may replicate the techniques in their first language.