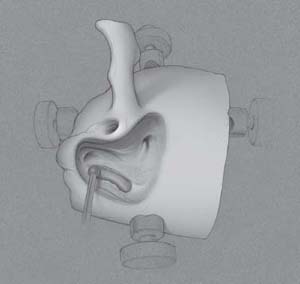
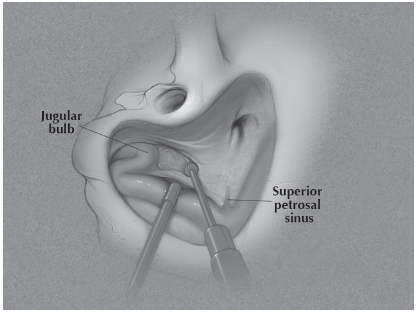
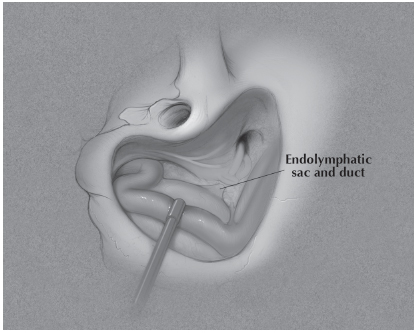
4 Persistent episodic vertigo due to Meniere’s disease despite maximal medical and intratympanic therapy may be addressed using surgical approaches. The labyrinthectomy provides a surgical gold standard for successful management of Meniere’s disease without serviceable hearing. The retrolabyrinthine dissection also provides intracranial access to the vestibular nerve just medial to the porus acusticus where it can be selectively sectioned preserving cochlear nerve integrity and hearing. Retrolabyrinthine surgery limited to the decompression of posterior fossa dura, particularly the endolymphatic sac,represents a controversial surgical therapy for Meniere’s disease. Fig. 4.1 Remove bone from posterior fossa dura and sigmoid. Using long strokes with a large burr, expose the lateral sinus and 1 cm of posterior fossa dura behind the sinus from the sinodural angle to the mastoid tip (Fig. 4.1). While decompressing the sinus with your suction, drill away the bone anterior and medial to the sinus, exposing the posterior fossa dura. Fig. 4.2 Expose pre-sigmoid dura and identify the jugular bulb. Expose the superior petrosal sinus starting at the sinodural angle, following this medially as the presigmoid bone is removed (Fig. 4.2). Extend your dissection medially through retrofacial cells (deep to the vertical segment of the facial nerve) to locate the jugular bulb. Follow the lateral sinus distally along the bend of the sigmoid segment to the bulb.
Labyrinthectomy
 Retrolabyrinthine Dissection
Retrolabyrinthine Dissection
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


