Intrastromal Corneal Ring Segments (INTACS)
Richard L. Abbott
V. Nicholas Batra
Refractive surgery is emerging as one of the most innovative areas in ophthalmology. Efforts to achieve a safe, efficacious, and potentially reversible method for the correction of refractive errors has led to the development of new refractive procedures. One of the new keratorefractive techniques is that involving the ICRS or intrastromal corneal ring segments, also called INTACS.
HISTORY
INTACS have been in development for many years. Use of materials placed in the cornea began in 1949 with Barraquer,1 who experimented with various materials for corneal implantation and refractive change. He abandoned the use of alloplastic materials because of the high incidence of extrusion in studies in cat and rabbit eyes. Other investigators continued to research the implantation of alloplastic materials, including polymethylmethacrylate (PMMA).2 In 1978, Fleming and Reynolds3 conceived the idea of a ring-shaped implant (intrastromal corneal ring [ICR]) that could be introduced through a single radial incision to alter the corneal curvature.
Early theoretical and animal work speculated that this ring would alter the corneal curvature through expansion or constriction of the device’s diameter, causing a flattening or steeping for myopia and hyperopia, respectively.4 Further refinement of a model for the refractive effect came from Silvestrin’s group5 postulating an arc shortening effect of the ring. Their model assumed that there are corneal lamellae that stretch from limbus to limbus. In that model, a spacer element such as the ICR separates corneal lamellae, resulting in a shortening of the arc length that is correlated with the device thickness (Fig. 1). Eye bank studies by T.E. Burris and coworkers then demonstrated the effect of varying implant thickness.6 By increasing the thickness of the ICR, an increased change in spherical equivalent was documented in a nearly linear fashion. Pinsky and colleagues7 then refined the model further by using finite element modeling (Fig. 2). A 360-degree ICR was used in initial studies in nonfunctional and myopic eyes in the Brazil and the United States.8 All eyes tolerated the implants well without evidence of extrusion or corneal thinning. Studies in nonfunctional eyes demonstrated the safety of the ICR (KeraVision, Fremont, CA).9 Based on these results, the US Food and Drug Administration (FDA) phase II studies of the intrastromal ring were started.
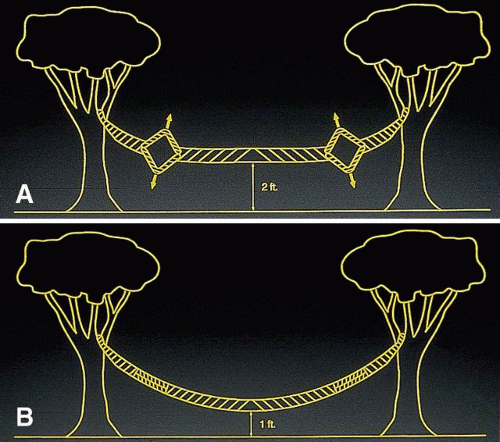 Fig. 1. A spacer element separates the corneal lamellae resulting in a shortening of the arc length and decrease in corneal curvature. |
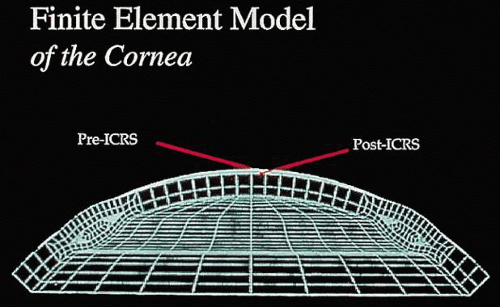 Fig. 2. Finite element model of the intrasomal corneal ring segments showing the change in corneal curvature induced by placement of the ring segments. |
The original ICR was a 360-degree PMMA ring with an external diameter of 8.1 mm, internal diameter of 6.8 mm, and thicknesses of 0.25 to 0.45 mm. Uncorrected visual acuity of 20/40 or better was obtained in 85% of 66 patients observed on a followup basis for 1 year.10 The ring was well tolerated; explants were performed in ten eyes. In all cases, eyes after explantation returned to within 1 diopter (D) of their preoperative refraction, indicating the potential removability of the ICR.11
In the phase II study, wound healing problems were observed with the PMMA ring directly beneath the incision.12 To address this issue, the ring was then redesigned into two 150-degree arc segments, which simplified insertion technique and separated the implant material away from the radial incision. The ring segments were then placed through a 1.8 mm superior incision at two thirds the corneal depth. Studies showed that the ICR segments were similar in refractive effect to those of the ICR.13,14
A phase III study has been completed to show the effects of the ICR segments for mild to moderate degrees of myopia with two 150-degree arc PMMA segments.15 Three segment thicknesses have been evaluated: 0.25, 0.30, and 0.35 mm. The objectives of the study were to rule out major safety risks, to ensure an acceptable outcome in uncorrected visual acuity, to ensure predictability of refractive effect, and to ensure stability of the refractive effect.16
SURGICAL PROTOCOL
The current version of INTACS consists of two 150-degree arc length segments of medical grade PMMA that vary in thickness from 0.25 to 0.35 mm in 0.05-mm increments. The outer diameter of the ring segments is 8.1 mm and that of the inner diameter 6.8 mm. The segments have a hexagonal cross-section and the curvature conforms to that of the cornea. The segments are shown in Figure 3.
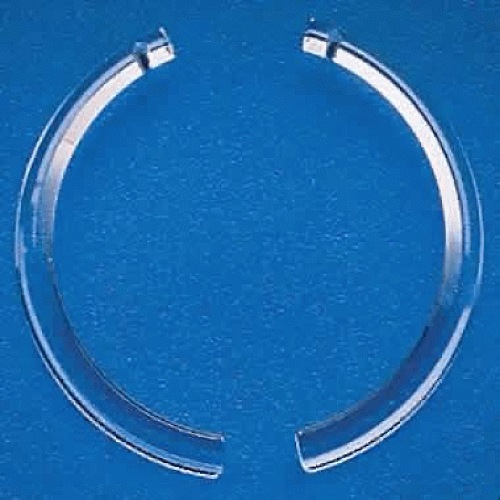 Fig. 3. The polymethylmethacrylate ring segments. |
Before the procedure is begun, patients should be given informed consent that includes the potential risks, benefits, and complications of the INTACS. Patients are typically given an antibiotic drop the day before to surgery to help prevent infection. This procedure may be performed under topical anesthetic or with other types of anesthesia. In the FDA phase II and III trials, 77.3% of patients received topical anesthesia with oral sedation, 8% received topical anesthesia alone, 14.5% received topical anesthesia with conscious IV sedation, and 0.2% received IV conscious sedation with parabulbar anesthesia.
Patients are prepped and draped for anterior segment surgery. Care should be taken to isolate the eyelashes and remove them from the surgical field. The center of the cornea should be marked using horizontal and vertical corneal measurements. A specially designed ICR segment marker is used to identify the correct location of the radial corneal incision (Fig. 4). An ultrasonic pachymeter is used to check the corneal thickness at the incision site. A diamond knife is then set at two thirds of this depth, and a 1.8-mm radial incision is made at the marked location. Then, a lamellar stromal spreader is inserted at the base of the incision and the tissue is separated laterally (Fig. 5). A vacuum guide is centered, and the vacuum is gradually increased to about 20 mm Hg (Fig. 6). The vacuum is used to fixate the globe during lamellar dissection. Specially designed dissecting instruments are then used to create pockets in a clockwise and counterclockwise manner for 190 degrees in each direction (Fig. 7). After these channels have been made, the segments are inserted through the incision and into the intrastromal channel (Fig. 8). The segments are selected using the Keravision nomogram (Table 1). After both segments have been placed, one or two 10-0 or 11-0 nylon sutures are used to close the incision (Fig. 9). The patient is given an antibiotic-steroid combination at the end of the procedure. A shield is placed on the eye at bedtime for up to 6 to 8 weeks.17,18
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


