Global goals, targets, and indicators for TB control 1
Millennium Development Goals set for 2015
Goal 6: Combat HIV/AIDS, malaria, and other diseases
Target 6c: Halt and begin to reverse the incidence of malaria and other major diseases
Indicator 6.9: Incidence, prevalence, and death rates associated with TB
Indicator 6.10: Proportion of TB cases detected and cured under DOTS
Stop TB Partnership targets set for 2015 and 2050
By 2015: Reduce prevalence and death rates by 50 %, compared with their levels in 1990
By 2050: Reduce the global incidence of active TB cases to <1 case per 1 million population per year
Pathogenesis
TB is primarily an airborne infection which spreads via inhalation of aerosolized droplets when infected patients cough or sneeze. Ingested organisms are either destroyed by the resident alveolar macrophages or may continue to survive and multiply causing necrosis. The ability to replicate within cells, particularly the macrophages and monocytes, is critical to the ability of M. tuberculosis to cause disease. Transformation of monocytes to epithelioid cells and multinucleated giant cells results in the formation of an epithelioid cell granuloma with central area of necrosis containing the acid-fast bacilli. Interferon-γ (gamma) has been shown to be capable of modifying macrophage capabilities with regard to immunity against TB [3].
Ocular Tuberculosis
Ocular TB represents extrapulmonary dissemination of the bacilli from the lungs. It can be primary ocular TB where the eye is the initial port of entry and includes conjunctival, corneal, and scleral disease. Secondary ocular TB implies hematogenous spread of the organism to the eye and includes tubercular uveitis, among others.
Incidence of ocular TB among patients with active systemic TB varies widely. Incidence of ocular TB was 1.46 % among 10 524 patients in a tuberculosis sanatorium [4]. In 1997, a prospective study [5] found 18 patients of ocular TB among 100 randomly chosen patients with systemic TB. In 2002, a study [6] in Africa found an incidence of 2.8 % among 109 patients with TB and HIV infection. The incidence of ocular TB among uveitis patients was 0.6 % in India [7], 7.9 % in Japan [8], and 10.5 % in Saudi Arabia [9]. In the period 1982–1992, in Boston, 0.6 % of patients with uveitis were believed to have ocular TB [10].
Because of the lack of uniformity in the diagnostic criteria for intraocular TB and the difficulty of confirming the diagnosis by laboratory methods, there are no reliable data to indicate its true prevalence.
In India, where pulmonary tuberculosis is endemic, the incidence of ocular involvement is variable. In 1995, Biswas and associates did a complete clinical ocular examination using slit-lamp biomicroscopy and indirect ophthalmoscopy and systemic examination, radiologic evaluation, Mantoux skin test, and sputum test for acid-fast bacilli in 1,005 patients from South India with active pulmonary and extrapulmonary tuberculosis and reported an ocular morbidity of 1.39 % [11]. In another study from the same center, tuberculosis was reported to constitute in 0.39 % of 1,273 uveitis patients [12].
Clinical Features
Ocular TB has protean manifestations and can involve any part of the eye or adnexa. Tubercular uveitis is the most common presentation and occurs due to hematogenous spread. It can also occur due to reactivation of dormant ocular lesions as is the case with other extrapulmonary lesions.
Anterior segment | Uveal tract and posterior segment |
|---|---|
1. Conjunctiva Primary – exogenous infection Secondary – contiguous infection Phlyctenulosis 2. Cornea Sclerokeratitis TB interstitial keratitis Deep central keratitis TB infiltrates TB corneal ulcers 3. Sclera Episcleritis Anterior scleritis Posterior scleritis | 1. Anterior uveitis Granulomatous anterior uveitis Nodular tuberculous iritis Conglomerate tubercle of the iris 2. Intermediate uveitis 3. Posterior uveitis Disseminated choroiditis Focal choroiditis – tubercle Subretinal abscess Serpiginoid choroiditis Retinal detachment 4. Retinal vasculitis 5. Optic nerve: Optic neuritis Optic disc granuloma |
Anterior Uveitis
Anterior uveitis in ocular tuberculosis presents with a smoldering, insidious, progressive form of granulomatous uveitis [13]. Non-granulomatous uveitis is also known to occur. Patients may present with unilateral or bilateral disease. The cornea shows mutton-fat keratic precipitates and the anterior chamber reveals cells and flare [14]. Fibrinoid reaction may occur with localized nodules on the iris surface (Fig. 15.1). Inferior corneal edema secondary to the mutton-fat keratic precipitates may occur. Old mutton-fat keratic precipitates may become pigmented. The anterior chamber angle may show localized nodules with peripheral anterior synechiae. The granuloma over the iris may occur over the surface of the iris or at the pupillary borders or in the angle [15]. Posterior synechiae occur frequently and the lens may show cataractous changes with formation of a papillary membrane. Iris bombe and displacement of the iris diaphragm toward the cornea may occur and result in pupillary block angle closure glaucoma. Cyclitis is frequently seen in tuberculosis and may cause caseating granuloma [13]. The surface of iris may show multiple nodules, especially near the pupillary border or the iris root [16, 17].
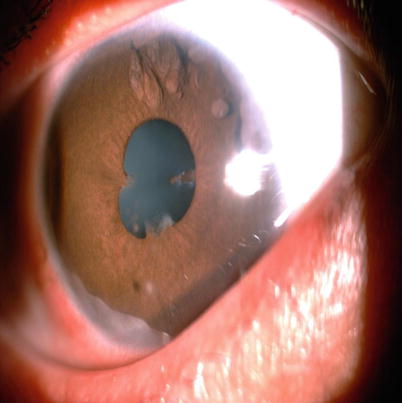
Fig. 15.1
A 21 year old female with active pulmonary tuberculosis presented with granulomatous keratic precipitates, iris nodules, peripheral anterior synechiae and posterior synechiae
In the acute, miliary form of tuberculosis, patients may present with anterior chamber inflammation; tissues stimulate an immune-mediated delayed hypersensitivity Th1 cell-driven reaction leading to the formation of granulomatous reaction [18] associated with small grayish-yellow or reddish nodules near the iris root.
Intermediate Uveitis
Posterior Uveitis
Choroidal Tubercles
They can be unilateral or bilateral, up to five in number although there may be as many as 50–60 in the same eye. They usually range from 0.5 to 3 mm in diameter and may be associated with an overlying serous retinal detachment. These tubercles heal within 12–14 weeks and leave behind pale atrophic areas with variable pigmentation. Active choroidal tubercles usually respond well to antitubercular treatment (ATT).
Tuberculoma
These tuberculomas may be located anywhere in the choroid, in the macula, the posterior pole, the equator, or in a juxtapapillary location. The tuberculomas generally present as a large solitary mass and may mimic a tumor. Hemorrhages and retinal folds may be seen on the tuberculoma surface, and in later stages, the overlying retina may detach. The tuberculoma may measure up to 14 mm in diameter. They may give the classical “ring of fire” appearance in fundus fluorescein angiogram. Large tuberculomas may present as yellowish subretinal mass lesions accompanied by exudative retinal detachment that shows good resolution with antitubercular treatment and steroids.
Subretinal Abscess
Multiplication of the bacilli in the caseous material of the granulomas can lead to liquefaction necrosis and abscess formation. Patients with disseminated tuberculosis may present with subretinal abscess with little overlying vitreous inflammation [21]. These necrotizing granulomas may be seen in isolation in the eye, with no evidence of tuberculosis in any other part of the body [22]. These abscesses are more yellowish in color indicating liquefaction necrosis and overlying retinal hemorrhages. These lesions usually heal with antitubercular therapy and healed lesions may show pigmentation and atrophy with chances of good visual recovery [7]. It may be seen in both immunocompetent and immunocompromised patients. Although uncommon, these may rupture into the vitreous cavity, resulting in the development of endophthalmitis/panophthalmitis leading to removal of the eye.
Serpiginous-Like Choroiditis
Serpiginous-like choroiditis is a rare, usually bilateral, chronic, progressive, recurrent inflammation of the retinal pigment epithelium, choriocapillaris, and choroid of unknown etiology. The earliest description of the condition, known as “peripapillary retinochoroiditis,” was coined in 1932 by Junius. Laatikainen and Erkkila were the first to describe the association of serpiginous choroiditis with TB [23]. Presumed tubercular serpiginous-like choroiditis has been classified into three morphologic variants (Fig. 15.2): multifocal choroiditis progressing to diffuse lesions resembling serpiginous choroiditis, diffuse choroiditis resembling serpiginous at initial presentation, and mixed variants in which opposite eyes had features of multifocal and diffuse lesions [24]. Although the precise cause of serpiginous choroiditis is thought to arise on an autoimmune basis and treatment classically mandates multiple systemic immunosuppressive medications or alkylating agents in some cases [25], presumed tubercular serpiginous-like choroiditis requires an anti-TB strategy sometimes in combination with corticosteroids (Fig. 15.3). Therefore, distinction between these two entities, which may be quite similar in appearance, is of paramount importance. Clinical features that may help to clinically distinguish tubercular serpiginous-like choroidopathy from serpiginous choroidopathy include the country of origin of the patient (i.e., patients from areas where TB is endemic), significant vitritis, and the presence of multifocal lesions in the posterior pole and periphery or juxtapapillary lesions sparing the periphery in serpiginous. The lesions appear as gray-white to yellow with ill-defined edges, classically begin in a peripapillary location, and spread centrifugally with multiple recurrences. The fluorescein angiographic appearance is distinctive, with the acute lesions showing early hypofluorescence and progressive late staining [26, 27].

Fig. 15.2
Active serpiginous choroiditis threatening the fovea in the left eye of a 37 year old male patient who had a positive mantoux and a positive quantiferon Tb gold test. Laser marks are seen tempora to the macula
Fig. 15.3
Post treatment with oral corticosteroids and a 4 drug ATT regimen, the fovea-threatening lesions show resolution
Retinal Vasculitis (Fig. 15.4)
Tubercular vasculitis presents with vitreous infiltrates (vitritis), retinal hemorrhages, neovascularization, and neuroretinitis. The presenting features are often similar to another common vasculitis, Eales’ disease, which by definition is idiopathic in nature and presents with recurrent vitreous hemorrhage in young patients. The eye usually does not show other signs of intraocular inflammation, for instance, the active or healed patches of focal choroiditis which are seen in patients with tubercular retinal vasculitis. Both diseases share the extensive capillary closure which may require laser photocoagulation. Tubercular vasculitis responds well to a combination of ATT and oral corticosteroids [28, 29].

Fig. 15.4
A young male patient presented with features of active peripheral vasculitis suggestive of Eale’s disease
Panophthalmitis/Endophthalmitis
Ocular TB can present as acute-onset endogenous endophthalmitis, due to rapidly progressive disease, which does not respond to ATT. This may occur due to rapid multiplication of bacilli or in patients who receive corticosteroid therapy without concomitant antitubercular drugs.
Differential Diagnosis
Infectious | Noninfectious |
|---|---|
Syphilis | Sarcoidosis |
Leprosy | Serpiginous choroiditis |
Toxoplasmosis | Sympathetic ophthalmia |
Histoplasmosis | Vogt–Koyanagi–Harada disease |
Borreliosis | Acute posterior multifocal placoid pigment epitheliopathy |
Brucellosis | Punctate inner choroidopathy |
Herpetic retinochoroiditis | Multifocal choroiditis and panuveitis |
HIV and Ocular Tuberculosis
TB and HIV act in deadly synergy. HIV infection increases the risk of TB infection on exposure, progression from latent infection to active TB, risk of death if not timely treated for both TB and HIV, and risk of recurrence even if successfully treated. Correspondingly, TB is the most common opportunistic infection and cause of mortality among people living with HIV (PLHIV) and difficult to diagnose and treat owing to challenges related to comorbidity, pill burden, co-toxicity, and drug interactions. Though only 5 % of TB patients are HIV infected, in absolute terms it ranks 2nd in the world and accounts for about 10 % of the global burden of HIV-associated TB [1].
Global estimation of burden of HIV-positive incident TB cases is 10,00,000 (11,00,000–12,00,000), while the estimates of HIV-positive incident TB cases in India is 75,000 (1,10,000–1,60,000). As per WHO’s Global TB Report of 2011, HIV prevalence among incident TB cases is estimated to be 3.3 % (5–7.1 %).
Because of the high co-occurrence of these two diseases, WHO has called for a joint action “Two diseases – one patient,” to deliver effective and comprehensive care targeted against HIV infection and tuberculosis [1].
Ocular TB most commonly occurs after primary pulmonary infection attributable to direct hematogenous spread or by hypersensitivity responses. It can present with protean manifestations including choroiditis, choroidal granulomas, chorioretinitis, endophthalmitis, subretinal abscess, and panophthalmitis [6, 21, 30–36].
In a large study in Chennai, India, from 1993 to 2005 by Biswas et al., they found the incidence of ocular TB in HIV patients to be 1.95 %. A study from the same population reported that 1.39 % of patients with active pulmonary TB and extrapulmonary TB had ocular TB, suggesting that HIV coinfection does not dramatically increase the rate of ocular TB [37]. The relatively high prevalence of EPTB and disseminated TB in HIV patients does not seem to be reflected in increased cases of ocular TB. Like non-HIV patients, among HIV-infected patients with ocular TB, choroidal granulomas were the most common presentation. They also reported that tuberculosis is unusual in that it can occur over a wide range of CD4 counts, although it is more frequent at CD4 counts <300 cells/_l. There was no correlation with CD4 cell counts. This also indicates that there is no typical presenting feature of ocular TB in patients with AIDS. As a result of this fact, clinicians in India, where tuberculosis is endemic, should be aware of various clinical presentations of ocular TB. Regular screening, follow-up, early diagnosis, and treatment of ocular TB in patients with AIDS become more imperative irrespective of the CD4 counts.
Ancillary Investigations
FFA and ICG
Fundus Fluorescein Angiography (FFA) is useful in cases of multifocal choroiditis, serpiginous-like choroiditis, retinal vasculitis, neuroretinitis, and subretinal abscess. Active choroiditis lesions present with hypofluorescence in early phases with hyperfluorescence in the late phases (Fig. Fig. 15.5a, b). The presence of areas of capillary nonperfusion and neovascularization can be picked up on FFA in cases of vasculitis.
Fig. 15.5
(a, b) Fundus fluorescein angiography images of the patient-early phases show hypofluorescence of the lesions near the fovea followed by hyperfluorescence in the late phases suggestive of active choroiditis lesions
Indocyanine Green Angiography (ICGA) has been proven useful in picking up subclinical lesions which might not be visible clinically or on FFA. Choroiditis lesions can be visualized as hypofluorescent spots in early and intermediate phases which become iso-or hypofluorescent in late phases.
OCT
Optical Cohenence Tomography (OCT) is useful in differentiating choroidal tubercles from other noninflammatory causes like central serous chorioretinopathy, choroidal tumors, exudative ARMD, etc. It is also helpful in assessing macular complications like cystoid macular edema or the presence of a choroidal neovascular membrane.
Newer diagnostic modalities like SD-OCT (spectral domain OCT) and enhanced depth imaging (EDI) are being used in the diagnosis and management of choroidal diseases like tuberculosis. EDI-OCT is being used to characterize these choroidal disorders and to evaluate efficacy of treatment [38].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


