Intraocular Triamcinolone in Pediatric Cataract Surgery
Abhay R. Vasavada
Sajani K. Shah
Mamidipudi R. Praveen
Rupal H. Trivedi
M. Edward Wilson
Posterior capsulectomy with or without vitrectomy is an essential surgical step in the management of pediatric cataract surgery. Pediatric cataract surgeons are more likely to encounter vitreous as compared with adult cataract surgeons. When the surgical plan is manual primary posterior continuous curvilinear capsulorhexis (PCCC) without vitrectomy, it is important to detect if the anterior vitreous face (AVF) is intact or disturbed. If the AVF is disturbed, an anterior vitrectomy is a necessary surgical step. When the surgical strategy is posterior capsulectomy with vitrectomy, it is vital to visualize vitreous to perform a thorough vitrectomy and to identify residual vitreous fibers. Any residual vitreous strands need to be removed as they can lead to retinal traction as well as irregularities in the pupil, intraocular lens (IOL) displacement, and visual axis opacification (VAO). This may lead to complications such as glaucoma, and retinal detachment. Thus, identification of vitreous plays a crucial role in ensuring the successful outcome of pediatric cataract surgery.
Although partial removal of the posterior capsule and anterior vitreous is commonly performed during pediatric cataract surgery, surgeons often find it difficult to visualize vitreous and define the end point of vitrectomy. Vitreous gel, transparent by design, is virtually invisible under the operating microscope. Vitreoretinal surgeons have used intravitreal injections of triamcinolone acetonide (TA) to visualize the vitreous. TA is a synthetic insoluble corticosteroid. In ocular surgery, TA functions like a dye to stain the vitreous, mainly because of crystal deposition.1 During pediatric cataract surgery, intracameral TA can be used to highlight vitreous known to be present (e.g., ectopia lentis), to check for suspected vitreous (e.g., ectopia lentis, history of ocular trauma, AVF disturbance), to confirm that all the vitreous has been cleared (e.g., after vitrectomy) from the anterior chamber, or as therapeutic agent to decrease inflammation. We have reported TA-assisted pediatric cataract surgery describing TA intraoperatively for better visualization of vitreous2,3 and suggesting its beneficial effect on postoperative inflammation.4 In addition, use of intracameral TA is also reported for both adult5 and pediatric cataract surgery to help decrease postoperative inflammation.6
TECHNIQUE
TA is commercially available under various brand names— for example, Triesence® (Alcon Labs, Fort Worth, TX, 40 mg/mL); Kenalog (Bristol-Myers-Squibb, Peapack, NJ, 40 mg/mL); Trivaris (Allergan, Irvine, CA, 80 mg/mL); Aurocort (Aurolab, India, 40 mg/mL), etc.1,2 Triesence® is US FDA approved for intraocular use. It is indicated for the treatment of uveitis and ocular inflammatory conditions unresponsive to topical corticosteroids. Triesence® suspension is also indicated for visualization during vitrectomy (package insert, Triesence®). It is preservative free (does not contain benzyl alcohol). Recommended dose for visualization is 1 to 4 mg (25-100 gL of 40 mg/mL suspension) administered intravitreally. It is provided as a single-use 1-mL vial containing 40 mg/mL of TA suspension.
We recommend using preservative-free TA suspension. If preservative-free suspension is not available, a method of removing the preservative has been reported in the literature.7 However, it is a tedious technique. Alternatively, some surgeons simply dilute 40 mg/mL TA 1:10 with balanced salt solution (BSS). However, the final product will contain 0.01% of benzyl alcohol preservative. Other surgeons prefer a sedimentation-resuspension-dilution technique. The technique involves leaving a Kenalog 40 mg/mL vial sitting undisturbed in the operating room. When TA is needed, the supernatant
is drawn off and replaced with an equal volume of BSS. The TA is typically then diluted 1:10 in BSS. Assuming supernatant removal of 90% or greater, the final product will contain 0.001% benzyl alcohol or less.8
is drawn off and replaced with an equal volume of BSS. The TA is typically then diluted 1:10 in BSS. Assuming supernatant removal of 90% or greater, the final product will contain 0.001% benzyl alcohol or less.8
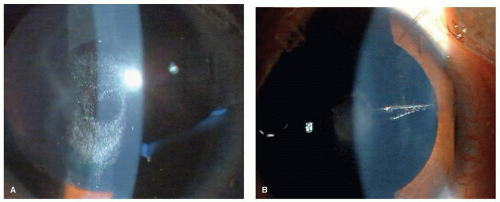 Figure 22.1. A: Disruption in the AVF, clearly visualized by the triamcinolone staining. B: Vitreous strands extending toward the incision. |
In the United States, most operating rooms now prefer to stock Triesence since it is approved for intraocular use and does not contain preservative. The lead authors of this chapter (ARV, SKS, MRP) use preservative-free Aurocort (Aurolab), which is similar to Triesence and available in India.2,3,4 These authors describe their use of TA during pediatric surgery below.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


