Intraocular Lens: Experimental Studies and Clinical Applications
Suresh K. Pandey
M. Edward Wilson
Intraocular lens (IOL) implantation at the time of cataract surgery has become the most common means of optical correction for children beyond infancy. A growing number of case series and a survey of practice styles and preferences of American Society of Cataract and Refractive Surgery (ASCRS) and American Association for Pediatric Ophthalmology and Strabismus (AAPOS) members support the safety and effectiveness of IOLs for children.1,2,3,4,5,6,7,8,9,10,11 An IOL can provide a full-time correction with optics that closely simulate those of the crystalline lens, with the exception of accommodation. However, some concern still remains about the unknown long-term risks of an IOL over the lifespan of a child. In addition, predicting the refractive change of even older children is difficult since individual variation in eye growth is common.
An IOL provides permanent continuous correction as opposed to aphakic glasses or aphakic contact lenses that can easily be removed by the child. This may be important in preventing amblyopia and encouraging normal visual development. Although glasses are usually necessary to obtain the best vision, uncorrected pseudophakic vision is probably less amblyogenic than is uncorrected aphakic vision.
IOL IMPLANTATION IN PEDIATRIC CATARACT SURGERY
Intraocular lenses manufactured from various rigid and foldable biomaterials have been used for pediatric cataract surgery for decades. Rigid implants manufactured from polymethyl methacrylate (PMMA) have been implanted in humans (adults and children) beginning more than 50 years ago. An IOL implanted in a child’s eye must stay there for several decades without biodegrading. PMMA has the longest safety record in both adults and children.
From the 1990s on, IOL implantation has been the standard method for correcting aphakia beyond infancy and when there is sufficient capsular support. The three most important reasons for increased use of IOLs in children are as follows.
Appropriately sized and more flexible implants can be inserted much more easily into the capsular bag of the child. Despite their increased flexibility, newer lens designs retain enough “memory” to resist the intense equatorial capsular fibrosis seen in children after implantation. PMMA as an implant material proved to be very biocompatible. In addition, copoly-merization of different acrylate and methacrylate acids resulted in foldable lenses with many of the same biocompatibility features as PMMA. As an example, foldable hydrophobic acrylic lenses, such as the AcrySof® (Alcon, Inc., Fort Worth, TX), are being implanted in the eyes of children of all ages. The biocompatibility of the hydrophobic acrylic lenses may equal or exceed that of the tried and true PMMA lenses. The foldable acrylic lenses are easier to insert in a small eye, and the squared edge of many of the optic designs now on the market may result in delayed posterior capsule opacification in young eyes. Pavlovic et al.5 reported that foldable silicone IOL implantation in children is also a safe procedure with stable short-term anatomic results.
Refined surgical techniques can more predictably ensure capsular fixation of the IOL. Surgeons have gained more confidence in the safety of “in-the-bag” implantation even over the extended lifespan of a child. Capsular fixation provides sequestration of the implant away from vascularized tissues. Although ciliary sulcus fixation of the IOL may also be safe, uveal contact for a lifetime is not as desirable. In addition, complications such as pupillary capture and IOL decentration are more common with ciliary sulcus fixation. The confidence in the safety of capsular fixation has resulted in more IOLs being implanted in children at the time of cataract extraction.
Finally, customized management of the anterior and posterior capsules for pediatric eyes at the time of implantation has improved outcomes and decreased complications. These improvements have provided for long-term centration of the IOL and a reduction in opacification of the visual axis after implantation.
IOL SIZING FOR PEDIATRIC CATARACT SURGERY
The mean axial length of a newborn’s eye is 17.0 mm compared to 23 to 24 mm in an adult. The pediatric eye, especially in the first 1 to 3 years of life, is significantly smaller than the adult eye.12 This has led to concerns about implantation of adult-sized IOLs in these eyes. In an effort to determine the size of the pediatric lens, Bluestein et al.12 examined 50 fresh, nonpreserved autopsy eyes from patients ranging in age from 1 day to 16 years. A variety of measurements were made, including the anterior-posterior, vertical, and horizontal lengths of the globe, corneal diameter, lens diameter, and diameter of the zonular free zone. The most rapid growth of the globe, the lens (Fig. 24.1), and the capsular bag occurred from birth to 2 years of age.
Currently available adult-sized IOLs are slightly oversized in relation to capsular bag measurements but may actually fit into eyes in the first 2 years of life, although possibly not into very small infantile eyes. The small capsular bag may become misshaped into an oval with these adult-sized IOLs. The ovality may vary from minimal to severe, depending on the design, type, and overall diameter of the implanted IOL (Fig. 24.2). There are several possible consequences of implantation of adult-sized IOLs into the relatively small capsular bag of infants and young children. First, in contrast to adult cataract surgery, dialing of the IOL haptics into the capsular bag can be difficult in infants and children. The combination of a small soft eye with vitreous upthrust and an oversized IOL will increase the risk of asymmetric (bag-sulcus) IOL fixation, which can lead to decentration of the IOL. Second, implantation of an oversized IOL in the capsular bag of a child may cause marked capsular bag stretching, resulting in posterior capsular folds and striae. The lens epithelial cells may migrate toward the visual axis, through the capsular folds, leading to opacification of the posterior capsule. Third, implantation of an oversized IOL in the capsular bag of a small child may cause zonular stress in the direction parallel to the IOL haptics. The long-term sequelae of the capsular bag stretching (and also the zonular stress) on the axial growth of the globe remains to be further investigated.
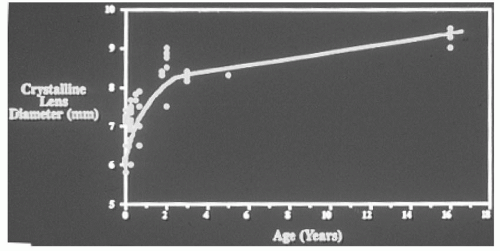 Figure 24.1. Graph showing the growth of the crystal-line lens. The most rapid growth occurs from birth to 2 years of age, and the growth of the crystalline lens is almost completed by the age of 2 years. (Reprinted from Bluestein EC, Wilson ME, Wang XH, et al. Dimensions of the pediatric crystalline lens: implications for intraocular lenses in children. J Pediatr Ophthalmol Strabismus 1996;33:18-20, with permission.) |
Pandey et al.13 compared the amount of capsulorhexis ovaling and capsular bag stretch produced by various rigid and foldable IOLs when implanted into pediatric human eyes obtained postmortem. In this study, 16 pediatric human eyes obtained postmortem were divided into two groups: Eight eyes were obtained from children <2 years of age (group A) and eight eyes were obtained from children >2 years of age (group B). All eyes were prepared according to the Miyake-Apple posterior video technique.14,15
Six IOL types (listed below), manufactured from rigid and foldable biomaterials, were implanted to determine the IOL design best suited for implantation in pediatric eyes.
Single-piece hydrophobic acrylic IOL (AcrySof®, SA30AL; 5.5-mm optic, 12.5-mm overall diameter; Alcon Inc., Fort Worth, TX).
Three-piece hydrophobic acrylic optic-PMMA haptic (AcrySof®, MA60BM; 6-mm optic, 13-mm overall diameter; Alcon Inc.)
Three-piece silicone optic-PMMA haptic (SI40NB; 6-mm optic, 13-mm overall diameter; AMO Inc., Santa Ana, CA).
Three-piece silicone optic-polyimide haptic (elastimide; 6-mm optic, 12.5-mm overall diameter; Staar Surgical Co., Monrovia, CA).
One-piece silicone plate IOL (AA-4203VF; 6-mm optic, 10.5-mm overall diameter; Staar Surgical Co.).
One-piece PMMA optic-PMMA haptic (809 P; 5-mm optic, 12-mm overall diameter; Pfizer Ophthalmics [formerly Pharmacia Inc.], New York).
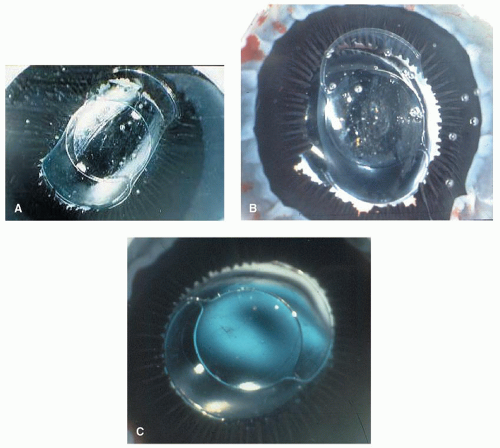 Figure 24.2. The small capsular bag may ovalize with these adult-sized IOLs; the ovality may vary from minimal to severe, depending on the design, type, and overall diameter of the implanted IOL. A: Miyake-Apple view after in-the-bag implantation of a one-piece, flexible open-loop, all-PMMA IOL, 13.75 mm in overall length, into an eye obtained postmortem from a 2-year-old child. Note the severe capsular bag stretch and ovaling between 1 o’clock and 7 o’clock. These indicate marked oversizing of the IOL in relation to the size of the capsular bag. B: Miyake-Apple view after in-the-bag implantation of a one-piece PMMA, flexible open-loop, modified C-loop capsular IOL, 12.5 mm in diameter, into an eye obtained postmortem from a 5-year-old child. Note the marked ovaling and elongation of the bag between 12 o’clock and 6 o’clock, indicating the slightly oversized IOL. C: Miyake-Apple posterior photographic view showing a one-piece, all-PMMA, 12.0-mm-diameter, modified C-loop IOL experimentally placed into the capsular bag in a cadaver eye of a 2-year-old child. Note the very optimum “fit” of the implanted IOL. (Reprinted from Wilson ME, Bluestein EC, Wang XH. Current trends in the use of intraocular lenses in children. J Cataract Refract Surg 1994;20:579-583, with permission.) |
The capsulorhexis opening and the capsular bag diameters were measured before IOL implantation and subsequently after in-the-bag IOL fixation with the haptics (or the main axis) of the lens at the 3 o’clock to 9 o’clock meridian. The percentage ovaling of the capsulorhexis opening was calculated by noting the difference in its horizontal diameter before and after IOL implantation. The percentage of capsular bag stretch was also calculated by noting the difference in the horizontal capsular bag diameter before and after IOL implantation.
All of the IOLs produced ovaling of the capsulorhexis opening, and stretching of the capsular bag, parallel to the IOL haptics. Figures 24.3 and 24.4 illustrate ovaling of the capsulorhexis opening and capsular bag stretch after implantation of rigid and foldable lenses in postmortem human eyes obtained from both group A and group B. Comparison of all six lens types within each group of eyes revealed significant differences in capsulorhexis ovaling and capsular bag stretch (P < 0.001, analysis of variance). However, the postcomparison difference was found to be significant only between the single-piece hydrophobic acrylic (AcrySof®) lens and the other lenses. The singlepiece hydrophobic acrylic lens was associated with significantly less capsulorhexis ovaling and capsular bag stretch in both group A and group B (12.06% ± 0.59% and 7.6% ± 1.47%, respectively).
Our study using postmortem human eyes suggests that IOLs, designed for the adult population, can be implanted in the capsular bag of infants and children. However, a variable degree of ovaling of the capsulorhexis opening and capsular bag stretch was seen after implantation of the adult-sized IOLs. Miyake-Apple posterior video technique confirmed the well-maintained configuration of the capsular bag (with minimal ovaling) after implantation of
the single-piece hydrophobic acrylic lens in both groups due to its flexible haptic design.
the single-piece hydrophobic acrylic lens in both groups due to its flexible haptic design.
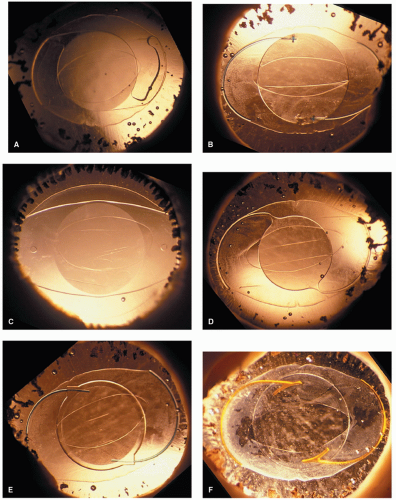 Figure 24.3. Gross photographs from the left eye of a 5-month-old child (anterior view with retroillumination). Note the variable degree of capsulorhexis ovaling and capsular bag stretch after implantation of the following rigid and foldable lens designs. Minimal capsulorhexis ovaling and capsular bag stretch were documented after implantation of a single-piece hydrophobic acrylic lens design. A: Single-piece hydrophobic acrylic (AcrySof®) IOL. B:
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|