Purpose
To investigate the role of intravitreal injection of triamcinolone acetonide (IVTA) in preventing photoreceptor apoptosis in eyes with rhegmatogenous retinal detachment (RRD) by measuring cytokine levels in the aqueous humor before and after IVTA.
Design
Prospective, nonrandomized, interventional case series.
Methods
setting : Institutional. patients : Nineteen eyes of 19 consecutive patients with RRD. intervention : All 19 eyes underwent IVTA 1 day before 25-gauge vitrectomy. Seventeen eyes free of retinal vascular disease served as controls. main outcome measure: Both baseline and 1 day post-IVTA measurements were made of the relative concentrations of 15 soluble factors (3 cytokines, 7 chemokines, and 5 growth factors). The associations with clinical findings, including macular status, were then analyzed.
Results
Elevated monocyte chemotactic protein 1 (MCP-1), macrophage inflammatory protein 1β (MIP-1β), and interferon γ–induced protein 10 (IP-10) in eyes with RRD were significantly reduced after IVTA. MCP-1 levels were significantly correlated with MIP-1β and IP-10 before and after IVTA. The decreases in MCP-1, MIP-1β, and IP-10 were also closely correlated to each other. Both before and after IVTA, MCP-1 was higher in eyes with macula-off RRD than in eyes with macula-on RRD.
Conclusions
IVTA suppressed elevated levels of intraocular MCP-1, MIP-1β, and IP-10 in eyes with RRD. The decrease in the aqueous levels of each of these factors was significantly correlated with the others. In addition to MCP-1, MIP-1β and IP-10 might potentially be additional target molecules for RRD therapy.
Rhegmatogenous retinal detachment (RRD) is a common retinal disease that causes visual field defects and severe visual disturbance. Newly developed surgical interventions, particularly 25-gauge microincision vitrectomy surgery (25GMIVS), have led to a very high initial reattachment rate for eyes with RRD, currently about 95%. Even after successful reattachment, however, degeneration of the photoreceptors in the detached area of the retina often prevents complete recovery of visual function.
Vitreous samples from eyes with RRD have shown significantly elevated levels of monocyte chemotactic protein 1 (MCP-1) compared to controls. Previous research by our team, performed with an experimental animal model, showed that MCP-1, along with tumor necrosis factor α (TNF-α), is implicated in the pathogenesis of photoreceptor degeneration and apoptosis following retinal detachment. Furthermore, the administration of antibodies and corticosteroid suppressed photoreceptor degeneration and apoptosis in our animal model and lowered the intraocular expression of both MCP-1 and TNF-α. The current study examines the specific effects of corticosteroid in human subjects with RRD. Corticosteroid is already in wide use for a variety of ocular diseases, and triamcinolone acetonide (TA) in particular is well recognized for its anti-inflammatory properties. There are many reports on the successful use of intravitreal injection of triamcinolone acetonide (IVTA) as a treatment for exudative conditions of the posterior segment.
In this prospective study, therefore, we hypothesized that in the preoperative period, IVTA would suppress inflammation and photoreceptor apoptosis in human eyes with RRD. To evaluate our hypothesis, we measured levels of intraocular mediators including chemokines and cytokines, such as MCP-1 and TNF-α, and analyzed their response to IVTA in eyes with RRD. Thus, the purpose of this report is to evaluate the effect of IVTA on the intraocular concentration of mediators in eyes with RRD.
Materials and Methods
Setting and Design
This was an institutional, prospective, nonrandomized, interventional case series. Subjects were recruited from patients referred to the Surgical Retina Service of Tohoku University Hospital. Surgical intervention and follow-up were both performed at this clinic. Informed consent for both the treatment and participation in the research for this prospective study (University Hospital Medical Information Network; UMIN Study ID N.: UMIN000009418) was approved by the institutional review board of Tohoku University Graduate School of Medicine (Prot. N.2006-262, November 20, 2006). Informed consent for both the treatment and participation in the research was obtained from each patient and the research was conducted according to the provisions of the Declaration of Helsinki, 1995 (as revised in Edinburgh, 2000).
Patients
All patients had RRD and were studied in the period before 25GMIVS. The inclusion criterion was clinically detectable RRD. The exclusion criteria were prior vitreous surgery or IVTA, intravitreal anti–vascular endothelial growth factor (VEGF), ocular inflammation, and vitreoretinal or optic nerve diseases. Clinical and demographic characteristics were collected, including age, macular status, extent of RRD, number of retinal breaks, preoperative best-corrected visual acuity (BCVA), 1-month-postoperative BCVA, 6-month-postoperative BCVA, 1-month-postoperative foveal thickness (FT), and 6-month-postoperative FT. BCVA was measured with the Landolt C visual acuity chart, and the decimal acuities were converted to logarithms of the minimal angle of resolution (logMAR) units. The extent of the RRD was graded 1 to 4 according to the number of quadrants it covered.
Intervention
IVTA was performed in all patients 1 day before 25GMIVS. The TA (Kenacort-A; Bristol-Meyers Squibb, Tokyo, Japan) diluent was replaced with a balanced salt solution (BSS Plus; Alcon Laboratories, Fort Worth, Texas, USA) after Millipore filtration (Millex GS Filter Unit with MF-Millipore MCE Membrane, 0.22 μm; Merck Millipore Ltd., Tullagreen, Carrigtwohill, County Cork, Ireland), and the volume was adjusted so that 0.1 mL contained 4 mg TA. The TA was injected using a 27-gauge needle and a standard pars plana approach (3.5 mm posterior to the limbus). Before performing IVTA, samples of the aqueous humor were collected and the levels of mediators in the anterior chamber were measured. We next performed IVTA, and a day later collected a second aqueous humor sample, before beginning 25GMIVS. During 25GMIVS, we also collected samples of the vitreous. Patients undergoing 25GMIVS for epiretinal membrane (ERM) or macular hole (MH) served as controls.
Main Outcome Measure
We investigated mediator levels in the pre- and post-IVTA aqueous humor, as well as the relationship between mediator levels and clinical findings including age, macular status, size of RRD, number of retinal tears, preoperative BCVA, 1-month-postoperative BCVA, 6-month-postoperative BCVA, 1-month-postoperative FT, and 6-month-postoperative FT. We also measured mediator levels in the post-IVTA vitreous.
Measurement of Inflammatory Mediators
We withdrew aqueous humor samples before IVTA with a 30-gauge needle, to prevent increasing intraocular pressure later on, after IVTA. We next collected aqueous humor samples 1 day after IVTA, just before 25GMIVS. Special care was taken to avoid touching intraocular tissues (ie, the cornea, the iris, and the lens) and to prevent mixing intraocular samples with other fluids. The samples of aqueous humor (about 100 μL) were collected in sterile tubes and were immediately frozen at −80 C. Control samples of the aqueous humor from eyes undergoing vitreous surgery for ERM or MH were collected as controls and were also immediately frozen. The inflammatory mediators we investigated fell into 3 groups: (1) 3 cytokines: interleukin 6 (IL-6), interferon γ (IFN-γ), and TNF-α; (2) 7 chemokines: MCP-1/CCL2; macrophage inflammatory protein 1α (MIP-1α)/CCL3; macrophage inflammatory protein 1β (MIP-1β)/CCL4; regulated on activation, normal T cell expressed and secreted (RANTES)/CCL5; eotaxin/CCL11; interferon γ–induced protein 10 (IP-10)/CXCL10; and IL-8/CXCL8; and (3) 5 growth factors: VEGF, basic fibroblast growth factor (bFGF), granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), and platelet-derived growth factor BB (PDGF-BB). Samples were analyzed using a multiplex bead analysis system, the Bio-Plex system (Bio-Rad Laboratories, Hercules, California, USA). A custom-made kit (Bio-Plex Human Cytokine Assay; Bio-Rad Laboratories) was used to detect the mediators. For the experiment, aqueous humor and vitreous samples were diluted 4 times with sample diluent (Bio-Rad Laboratories). A total volume of 50 μL from each sample was used for the assay. The kits were used according to the manufacturer’s instructions.
Statistical Analyses
All analyses were performed with Ekuseru-Toukei 2006 software (Social Survey Research Information Co Ltd, Tokyo, Japan). The data are presented as means ± standard deviation. The significance of the difference between the pre- and post-IVTA data was assessed by the Wilcoxon signed rank test. The significance of the difference in the concentration of cytokines between eyes with an RRD and control subjects was assessed by the Mann-Whitney U test. The Spearman coefficient of correlation by rank was calculated to determine the correlation between aqueous humor and vitreous levels of the mediators. The Spearman coefficient of correlation by rank was also calculated to determine the correlation between the cytokine levels in the aqueous humor and clinical findings. The significance of the difference in the concentration of the cytokines between eyes with a macula-off RRD and macula-on RRD was assessed by the Mann-Whitney U test. A P value of less than .05 was considered to be statistically significant.
Results
Nineteen eyes of 19 patients (15 men and 4 women) with RRD were included in this study. The ages of the patients ranged from 40 to 71 years with a mean of 56.9 ± 8.0 years. Preoperative BCVA was 0.50 ± 0.75 logMAR units and ranged from −0.08 to 2.00 logMAR units. One-month-postoperative BCVA was 0.27 ± 0.40 logMAR units and ranged from −0.08 to 1.22 logMAR units. Six-month-postoperative BCVA was 0.11 ± 0.23 logMAR units and ranged from −0.08 to 0.70 logMAR units. One-month-postoperative BCVA and 6-month-postoperative BCVA were better than preoperative BCVA ( P = .06 and P = .04, respectively). One-month-postoperative FT was 232.7 ± 42.4 μm and ranged from 156 to 306 μm. Six-month-postoperative FT was 246.1 ± 37.1 μm and ranged from 170 to 300 μm. The mean follow-up period was 7.3 ± 3.5 months with a range of 2 to 13 months. There were 11 eyes with macula-off RRD and 8 eyes with macula-on RRD. The extent of the RRD was 1.8 ± 0.5 and ranged from 1 to 3. The mean number of retinal tears was 2.1 ± 1.8. Complete reattachment was finally obtained in all 19 eyes with RRD after surgical intervention following IVTA. No severe adverse events such as endophthalmitis or any systemic side effects were observed in the study. Seventeen patients, including 9 with an ERM and 8 with an MH, were studied as controls.
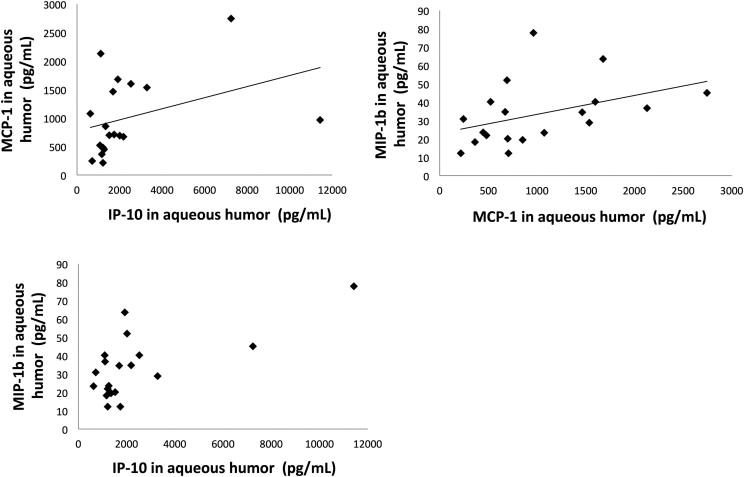
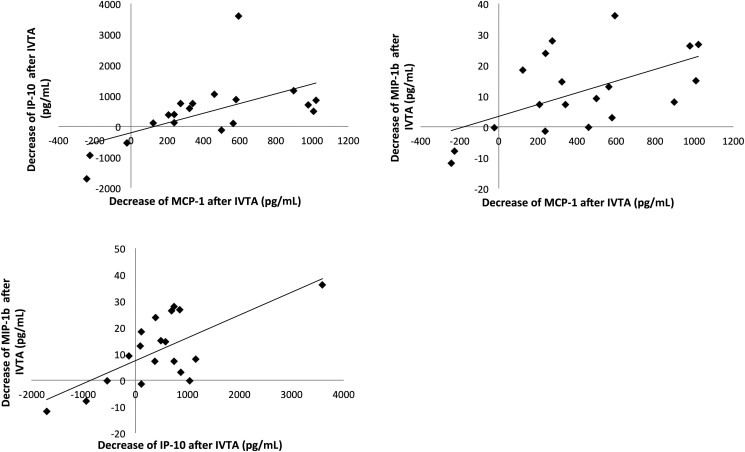
At baseline, IL-6, IFN-γ, MCP-1, MIP-1β, eotaxin, IP-10, IL-8, VEGF, and G-CSF were detected in the aqueous and were significantly higher in eyes with an RRD than in controls ( P < .001, P = .003, P < .001, P < .001, P < .001, P < .001, P < .001, P = .003, P < .001, respectively) ( Table ). Before IVTA, the aqueous humor level of MCP-1 was significantly correlated with that of IP-10 ( r = 0.48, P = .04) ( Figure 1 , Top left). In addition, the aqueous humor level of MCP-1 was also significantly correlated with that of MIP-1β ( r = 0.50, P = .03) ( Figure 1 , Top right). The aqueous humor level of IP-10 was likely correlated with that of MIP-1β, but not significantly ( r = 0.44, P = .06) ( Figure 1 , Bottom). After IVTA, the levels of MCP-1, MIP-1β, and IP-10 were significantly reduced ( P < .001, P = .004, and P = .04, respectively) ( Table ). Each mediator showed a correlated decrease with the others, (MCP-1 and IP-10: r = 0.69, P = .001; MCP-1 and MIP-1β: r = 0.57, P = .01; IP-10 and MIP-1β: r = 0.47, P = .04) ( Figure 2 ; Top left, Top right, and Bottom, respectively). After IVTA, the aqueous humor level of MCP-1 was significantly correlated with that of IP-10 ( r = 0.55, P = .01) ( Figure 3 , Top left). In addition, the aqueous humor level of MCP-1 was significantly correlated with that of MIP-1β ( r = 0.56, P = .01) ( Figure 3 , Top right). The aqueous humor level of IP-10 was also significantly correlated with that of MIP-1β ( r = 0.49, P = .03) ( Figure 3 , Bottom). After IVTA, the vitreous level of MCP-1 was significantly correlated with the aqueous humor level of MCP-1 ( r = 0.52, P = .03) ( Figure 4 , Top left). In addition, the vitreous level of IP-10 was significantly correlated with the aqueous humor level of IP-10 ( r = 0.78, P < .001) ( Figure 4 , Top right). The vitreous level of MIP-1β was significantly correlated with the aqueous humor level of MIP-1β ( r = 0.86, P < .001) ( Figure 4 , Bottom). After IVTA, the vitreous level of MCP-1 was significantly correlated with that of IP-10 ( r = 0.71, P = .001) ( Figure 5 , Top left). In addition, the vitreous level of IP-10 was significantly correlated with that of MIP-1β ( r = 0.58, P = .01) ( Figure 5 , Top right). The vitreous level of MCP-1 was likely correlated with that of MIP-1β, but not significantly ( r = 0.41, P = .09) ( Figure 5 , Bottom).
| Groups | Mediators | Control (n = 17) (pg/mL) | RRD (n = 19) | P Value | ||
|---|---|---|---|---|---|---|
| Baseline (pg/mL) | After IVTA (pg/mL) | C vs B | B vs I | |||
| Cytokines | IL-6 | 21 ± 23 | 261 ± 674 | 277 ± 617 | <.001 a | .27 |
| IFN-γ | 5.4 ± 8.2 | 16.8 ± 12.7 | 22.9 ± 9.6 | .003 a | .04 b | |
| TNF-α | 4.0 ± 7.3 | 3.6 ± 2.9 | 4.9 ± 2.8 | .02 a | .02 b | |
| Chemokines | MCP-1 | 177 ± 26 | 1004 ± 667 | 591 ± 515 | <.001 a | <.001 b |
| MIP-1α | 1.3 ± 2.9 | 0.14 ± 0.28 | 0.22 ± 0.28 | .77 | .21 | |
| MIP-1β | 11 ± 3.7 | 33.4 ± 16.7 | 22.2 ± 10.3 | <.001 a | .004 b | |
| RANTES | 2.8 ± 3.4 | 3.0 ± 2.4 | 5.9 ± 3.2 | .48 | .008 b | |
| Eotaxin | 0.0 ± 0.0 | 22.6 ± 18.7 | 35.0 ± 21.0 | <.001 a | .11 | |
| IP-10 | 485 ± 491 | 2384 ± 2553 | 1936 ± 1856 | <.001 a | .04 b | |
| IL-8 | 4.5 ± 2.9 | 21.6 ± 11.6 | 26.7 ± 16.8 | <.001 a | .20 | |
| Growth factors | VEGF | 61 ± 25 | 123 ± 67 | 206 ± 117 | .003 a | <.001 b |
| bFGF | 9.5 ± 8.8 | 11.9 ± 11.5 | 20.3 ± 11.5 | .35 | .009 b | |
| G-CSF | 1.9 ± 3.4 | 19.7 ± 38.9 | 97.2 ± 107.8 | <.001 a | <.001 b | |
| GM-CSF | 191 ± 37 | 212 ± 68 | 275 ± 59 | .23 | .001 b | |
| PDGF-BB | 3.8 ± 5.3 | 5.3 ± 3.9 | 9.4 ± 4.1 | .06 | .007 b | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


