Overview of Interventional Endoscopy
|
 Endoscopic hemostasis
Endoscopic hemostasis Specimen collection
Specimen collection Endoscopic treatment of precancerous lesions and early carcinoma
Endoscopic treatment of precancerous lesions and early carcinoma Endoscopic tube placement
Endoscopic tube placement Foreign body removal
Foreign body removal Endoscopic treatment of stenoses
Endoscopic treatment of stenoses Dye methods
Dye methods 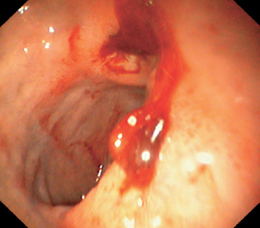
Fig. 4.1 Bleeding gastric ulcer
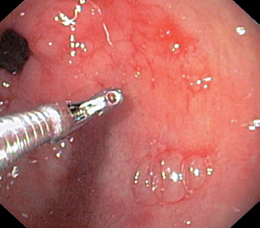
Fig. 4.2 Endoscopic biopsy
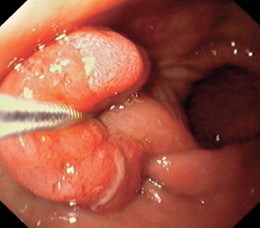
Fig. 4.3 Polyp removal
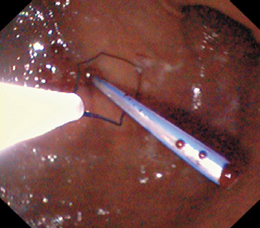
Fig. 4.4 PEG placement

Fig. 4.5 Foreign body removal: coins

Fig. 4.6 Stent insertion for a malignant esophageal stricture
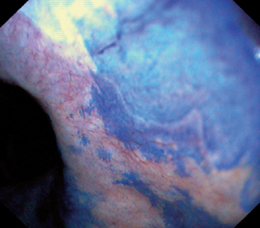
Fig. 4.7 Methylene blue staining of Barrett esophagus
Upper Gastrointestinal Bleeding: Incidence and Signs
 Incidence
Incidence
Acute gastrointestinal bleeding is the most common emergency in gastroenterology. Ninety percent of all acute hemorrhages arise in the upper gastrointestinal tract, approximately 9 % in the colon, and approximately 1 % between the ligament of Treitz and the ileocecal valve (Figs. 4.8, 4.9). The incidence is age-dependent, ranging from approximately 30:100 000 in young individuals to as much as 400:100 000 in persons over age 75 according to published reports. The overall mortality rate is approximately 15%; it is markedly lower in young patients, rising to 40% in elderly patients with multiple morbidity.
 Causes
Causes
The most frequent cause is ulcer bleeding associated with the ingestion of nonsteroidal anti-inflammatory drugs (NSAIDs). This type of bleeding usually occurs early during NSAID use and may occur even at low doses. The concomitant use of corticosteroids significantly increases the risk, and concurrent anticoagulant use can increase it dramatically.
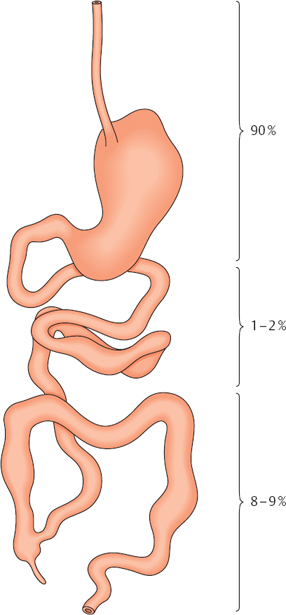
Fig. 4.8 Relative frequency of acute bleeding at different levels in the gastrointestinal tract
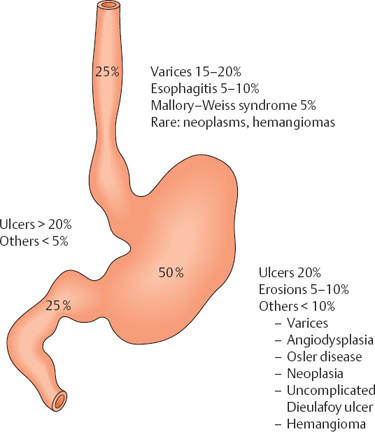
Fig. 4.9 Location and relative frequency of acute upper gastrointestinal bleeding
 Symptoms
Symptoms
The main symptoms of upper gastrointestinal bleeding are hematemesis, melena, and signs of hemorrhagic shock.
The major problems associated with upper gastrointestinal bleeding are hemorrhagic shock and aspiration pneumonia (bleeding and vomiting). They dictate the priorities that are followed in primary treatment:
- Hemodynamic stabilization
- Maintenance of adequate respiration
- Identifying the source of bleeding and hemostasis
- Prevention of rebleeding
| Cardinal symptoms and likelihood of massive bleeding |
|---|
|
| General symptoms |
|
 Dizziness
Dizziness Syncope Dyspnea
Syncope Dyspnea Angina pectoris
Angina pectoris Hemorrhagic shock
Hemorrhagic shock
Upper Gastrointestinal Bleeding: Primary Treatment
 Hemodynamic Stabilization
Hemodynamic Stabilization
 Is there impending or frank hemorrhagic shock (Table 4.3)?
Is there impending or frank hemorrhagic shock (Table 4.3)?
 Caution: Symptoms may be masked by:
Caution: Symptoms may be masked by:
– Beta-blocking drugs
– Vasovagal bradycardia
– Preexisting hypertension
 Note:
Note:
– An orthostatic rise in the heart rate by more than 20 bpm suggests a blood loss greater than 500 mL
– A blood pressure differential > 15-20 mmHg between sitting and lying down suggests a blood loss greater than 1000 mL
 Treat for shock before performing endoscopy!
Treat for shock before performing endoscopy!
– Place two large-caliber i. v. lines as soon as possible.
– Augment the circulating volume (preferably with a crystalloid such as 100 mL physiological saline solution or Ringer lactate).
– Goal: Heart rate < 100 bpm, blood pressure > 100 mmHg
 Necessary laboratory tests
Necessary laboratory tests
– Blood for typing, cross-matched blood, blood count, coagulation values, electrolytes
|
 Heart rate > 100
Heart rate > 100 Blood pressure < 100 systolic
Blood pressure < 100 systolic Cool extremities
Cool extremities Cold sweat
Cold sweat Obtundation
Obtundation Angina pectoris
Angina pectoris Maintaining Adequate Respiration
Maintaining Adequate Respiration
 Clear the airway (Caution: vomited blood).
Clear the airway (Caution: vomited blood).
 Suction the airway as needed.
Suction the airway as needed.
 Administer O2 by nasal catheter.
Administer O2 by nasal catheter.
 Intubate if necessary (Table 4.4).
Intubate if necessary (Table 4.4).
|
 Frank hemorrhagic shock
Frank hemorrhagic shock Patient somnolent before endoscopy
Patient somnolent before endoscopy Patient uncooperative before endoscopy
Patient uncooperative before endoscopy
 Identify the Source of Bleeding and Stop the Bleeding
Identify the Source of Bleeding and Stop the Bleeding
 Preendoscopy checklist
Preendoscopy checklist
– Adequate treatment for shock?
– Need to intubate before endoscopy?
– Time for blood replacement? (If Hb < 8, try to transfuse before endoscopy.)
– Open surgery instead of endoscopy (Table 4.5)
 Identify the source of bleeding
Identify the source of bleeding
– Always perform complete esophagogastroduodenoscopy (EGD) according to standard protocols.
– If one bleeding site is detected, always look for another potential source of bleeding.
– It is not unusual for multiple sources of bleeding to coexist.
 Hemostasis
Hemostasis
– The most frequent sources of upper gastrointestinal bleeding are ulcers and varices (Fig. 4.9).
– Hemostatic modalities include pharmacological therapy, balloon catheter insertion, injection therapy, thermal methods, banding, and transjugular intrahepatic portosystemic shunting (TIPS). The method of choice is determined by customary recommendations and by the technical capabilities and interests of the endoscopy department.
– The goals of endoscopic treatment are always to control active bleeding and prevent rebleeding. Endoscopic techniques are appropriate for the sources of bleeding listed in Table 4.6. Necessary instruments and equipment are listed in Table 4.7.
 Prevent rebleeding
Prevent rebleeding
|
 Refractory shock
Refractory shock Recurrent bleeding from a known ulcer on the posterior wall of the duodenal bulb
Recurrent bleeding from a known ulcer on the posterior wall of the duodenal bulb Recurrent bleeding in an elderly patient with comorbidity
Recurrent bleeding in an elderly patient with comorbidity Recurrent bleeding in a patient with high initial bleeding activity
Recurrent bleeding in a patient with high initial bleeding activity
|
 Esophageal varices and fundic varices
Esophageal varices and fundic varices Gastric and duodenal ulcer
Gastric and duodenal ulcer Reflux esophagitis
Reflux esophagitis Mallory-Weiss syndrome
Mallory-Weiss syndrome Erosions
Erosions
|
 Endoscope with a large working channel
Endoscope with a large working channel High-performance suction pump
High-performance suction pump Second suction pump for the pharynx
Second suction pump for the pharynx Water pump for irrigation
Water pump for irrigation Sclerotherapy needles
Sclerotherapy needles Injection needles for Histoacryl
Injection needles for Histoacryl Clips with applicators
Clips with applicators Argon plasma coagulation
Argon plasma coagulation Multiband ligator set
Multiband ligator set Epinephrine 1 :1000
Epinephrine 1 :1000 Histoacryl
Histoacryl Lipiodol
Lipiodol Polydocanol 1 %
Polydocanol 1 % Fibrin glue (optional)
Fibrin glue (optional)
Bleeding Esophageal Varices and Fundic Varices: Medications and Tubes
The mortality rate due to variceal bleeding (Fig. 4.10) is high, at 15-30%. The recurrence rate after an initial bleed is approximately 60% during the first two weeks. One third of varices will stop bleeding spontaneously.
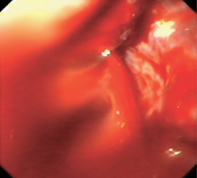
Fig. 4.10 Bleeding esophageal varices
 Treatment Methods
Treatment Methods
The following treatment methods are used:
 Pharmacological
Pharmacological
– Terlipressin plus nitrate
 Balloon tamponade
Balloon tamponade
– Sengstaken-Blakemore tube (for esophageal varices)
– Linton-Nachlas tube (for fundic varices)
 Endoscopic
Endoscopic
– Sclerotherapy
– Banding
 TIPS
TIPS
 Operative treatment
Operative treatment
Besides the control of bleeding and prevention of rebleeding, additional therapeutic measures may be taken depending on the clinical situation (Table 4.8).
|
 PPI i.v.
PPI i.v. Antibiotic therapy (lowers risk of rebleeding and of spontaneous bacterial peritonitis)
Antibiotic therapy (lowers risk of rebleeding and of spontaneous bacterial peritonitis) Lactulose 3×50 mL
Lactulose 3×50 mL Neomycin 2-4g/day
Neomycin 2-4g/day Protein restriction
Protein restriction Fresh frozen plasma
Fresh frozen plasma Packed red blood cells
Packed red blood cells Volume replacement
Volume replacement
 Pharmacological Therapy of Bleeding Esophageal Varices
Pharmacological Therapy of Bleeding Esophageal Varices
Principle and Key Characteristics
 Principle: medication to lower the portal venous and intravenous pressure
Principle: medication to lower the portal venous and intravenous pressure
 Vasopressin and terlipressin are the only two medications that have been approved for the treatment of bleeding esophageal varices.
Vasopressin and terlipressin are the only two medications that have been approved for the treatment of bleeding esophageal varices.
– Terlipressin is superior to vasopressin owing to its longer half-life.
– Terlipressin should be combined with nitrates due to possible side effects (ischemia and necrosis).
 Pharmacologic therapy is an acceptable alternative to balloon tamponade if emergency endoscopy cannot be performed.
Pharmacologic therapy is an acceptable alternative to balloon tamponade if emergency endoscopy cannot be performed.
Materials
 Terlipressin
Terlipressin
 Glyceryl nitrate
Glyceryl nitrate
 Intravenous access
Intravenous access
 Perfusor and perfusor tubing
Perfusor and perfusor tubing
 Syringes
Syringes
Technique
 Terlipressin, 2 mg by i. v. bolus
Terlipressin, 2 mg by i. v. bolus
 Repeat at 1 mg every four to six hours
Repeat at 1 mg every four to six hours
 Duration: two to three days
Duration: two to three days
 Always combined with glyceryl nitrate i.v. by perfusor, 14 mg/hour
Always combined with glyceryl nitrate i.v. by perfusor, 14 mg/hour
 Balloon Tamponade
Balloon Tamponade
Principle and Key Characteristics
 Principle: external compression of the bleeding varix with an inflated balloon
Principle: external compression of the bleeding varix with an inflated balloon
 Suitable if emergency endoscopy is not an option or as a temporizing measure after unsuccessful endoscopic or operative treatment or TIPS
Suitable if emergency endoscopy is not an option or as a temporizing measure after unsuccessful endoscopic or operative treatment or TIPS
 Esophageal varices: Sengstaken-Blakemore tube (two balloons)
Esophageal varices: Sengstaken-Blakemore tube (two balloons)
 Fundic varices: Linton-Nachlas tube (one balloon)
Fundic varices: Linton-Nachlas tube (one balloon)
Problems
 Pressure necrosis
Pressure necrosis
 Aspiration pneumonia
Aspiration pneumonia
 Rupture of the cardia
Rupture of the cardia
 Retching or vomiting may dislodge the tube, causing airway obstruction (Tube can be cut in an emergency; keep scissors handy)
Retching or vomiting may dislodge the tube, causing airway obstruction (Tube can be cut in an emergency; keep scissors handy)
Materials
 Sengstaken-Blakemore or Linton-Nachlas tube
Sengstaken-Blakemore or Linton-Nachlas tube
 Topical anesthetic
Topical anesthetic
 Lubricant
Lubricant
 Padding
Padding
 Adhesive tape
Adhesive tape
 Manometer
Manometer
 50-mL syringe
50-mL syringe
 Clamps
Clamps
Technique
 Do not tamponade if the patient is vomiting.
Do not tamponade if the patient is vomiting.
 Check the tube for air tightness before use.
Check the tube for air tightness before use.
 Smear the tube and balloon with lubricant.
Smear the tube and balloon with lubricant.
 Anesthetize the nasal mucosa.
Anesthetize the nasal mucosa.
 Squeeze residual air from the balloon.
Squeeze residual air from the balloon.
 Insert the tube transnasally, advancing to 50 cm.
Insert the tube transnasally, advancing to 50 cm.
 Sengstaken–Blakemore tube
Sengstaken–Blakemore tube
– Inflate the gastric balloon to 150 mL and clamp off. Slowly withdraw the tube until a springy resistance, synchronous with respirations, is felt.
– Secure the tube with strong adhesive tape.
– Pad the tube at the nostrils.
– Inflate the epithelial balloon to 45 mmHg by manometry, then clamp.
 Linton–Nachlas tube
Linton–Nachlas tube
– Inflate the balloon to 400 mL
– Withdraw until a springy resistance is felt.
– Secure in place.
– Add another 200 mL
 Deflate the tube for 30 minutes every six to eight hours.
Deflate the tube for 30 minutes every six to eight hours.
 Maximum duration of tube placement: 24 hours.
Maximum duration of tube placement: 24 hours.
Bleeding Esophageal Varices: Sclerotherapy
 Endoscopic Treatments
Endoscopic Treatments
The treatment of choice for bleeding varices is endoscopic therapy. The following methods are available:
 Sclerotherapy with polidocanol (esophageal varices)
Sclerotherapy with polidocanol (esophageal varices)
 Rubber band ligation (esophageal varices)
Rubber band ligation (esophageal varices)
 Sclerotherapy with Histoacryl (fundic varices)
Sclerotherapy with Histoacryl (fundic varices)
 Sclerotherapy with Polidocanol (Ethoxysclerol)
Sclerotherapy with Polidocanol (Ethoxysclerol)
Principle and Key Characteristics (Fig. 4.11)
 Principle: compression and thrombosis of the varix, induction of inflammation with subsequent scarring
Principle: compression and thrombosis of the varix, induction of inflammation with subsequent scarring
 Paravariceal or intravariceal injection
Paravariceal or intravariceal injection
 Established therapy
Established therapy
 Advantages
Advantages
– Good in cases where vision is poor
– Relatively easy to perform
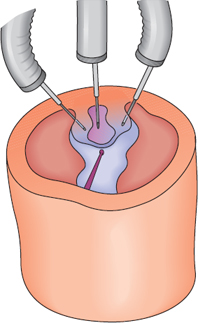
Fig. 4.11 Treatment of esophageal varices. Principle of paravariceal and intravariceal injection of the sclerosant
Materials
 Endoscope
Endoscope
 Suction pump
Suction pump
 Water jet
Water jet
 Sclerotherapy needle, 4-6 mm long
Sclerotherapy needle, 4-6 mm long
 Polidocanol 0.5-1 %
Polidocanol 0.5-1 %
 Technique (Figs. 4.12, 4.13)
Technique (Figs. 4.12, 4.13)
 Lateral position with the upper body elevated
Lateral position with the upper body elevated
 No pharyngeal anesthesia
No pharyngeal anesthesia
 Pulse oximetry
Pulse oximetry
 The instrument is inserted, and the bleeding varix is identified.
The instrument is inserted, and the bleeding varix is identified.
 Injection is begun close to the cardia.
Injection is begun close to the cardia.
 Intravariceal and paravariceal injection
Intravariceal and paravariceal injection
- – 0.5 mL injected on both sides of the varix (produces compression, inflammation, fibrosis)
- – 1.0 mL injected directly into the varix (induces thrombosis)
- – Maximum of 2 mL per injection site
- – 0.5 mL injected on both sides of the varix (produces compression, inflammation, fibrosis)
 If there is postinjection bleeding, advance the endoscope and compress the varix for approximately one minute.
If there is postinjection bleeding, advance the endoscope and compress the varix for approximately one minute.
 If no further bleeding occurs, sclerose any varices that show signs of an increased bleeding risk.
If no further bleeding occurs, sclerose any varices that show signs of an increased bleeding risk.
 If treatment is unsuccessful, discontinue sclerotherapy and insert a Sengstaken-Blakemore tube.
If treatment is unsuccessful, discontinue sclerotherapy and insert a Sengstaken-Blakemore tube.
Aftercare
 See Management of Bleeding Varices, page 88.
See Management of Bleeding Varices, page 88.
Complications
 Sclerotherapy ulcer
Sclerotherapy ulcer
 Esophageal stricture
Esophageal stricture
 Esophageal perforation
Esophageal perforation
 Pleural effusion
Pleural effusion
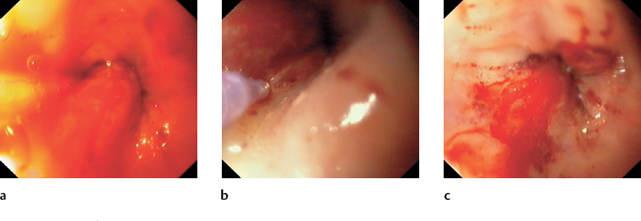
Fig. 4.12a–c Injection therapy of bleeding esophageal varices
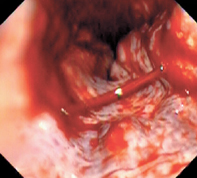
Fig. 4.13 Spurting hemorrhage from an esophageal varix
Bleeding Esophageal Varices: Banding
Principle and Key Characteristics
 Varix is sucked into a sleeve at the endoscope tip and ligated with an elastic band.
Varix is sucked into a sleeve at the endoscope tip and ligated with an elastic band.
 Induction of thrombosis, necrosis, and scarring
Induction of thrombosis, necrosis, and scarring
 Established therapy
Established therapy
 Advantages
Advantages
– Low complication rate
– Overall mortality and mortality due to bleeding are lower than in sclerotherapy
– Early rebleeding is less common than with sclerotherapy
 Disadvantage
Disadvantage
– Limited vision in cases with massive bleeding
Materials (Fig. 4.14a)
 Endoscope
Endoscope
 Suction pump
Suction pump
 Water jet
Water jet
 Variceal ligation set (multi- or single-band ligator)
Variceal ligation set (multi- or single-band ligator)
 Technique (Figs. 4.14 b, 4.15)
Technique (Figs. 4.14 b, 4.15)
 Use a standard endoscope with an overtube.
Use a standard endoscope with an overtube.
 Advance the overtube.
Advance the overtube.
 Perform a complete EGD.
Perform a complete EGD.
 Withdraw the endoscope.
Withdraw the endoscope.
 Set up the endoscopic and ligation set.
Set up the endoscopic and ligation set.
 Reenter through the overtube.
Reenter through the overtube.
 Begin the ligation near the cardia.
Begin the ligation near the cardia.
 Entrap the varix, suck the varix into the sleeve, and release the elastic band.
Entrap the varix, suck the varix into the sleeve, and release the elastic band.
 Usually three or four bands are applied per sitting, but considerably more may be placed if needed.
Usually three or four bands are applied per sitting, but considerably more may be placed if needed.
 If bleeding is severe and it is difficult to identify the source, band the distal varices.
If bleeding is severe and it is difficult to identify the source, band the distal varices.
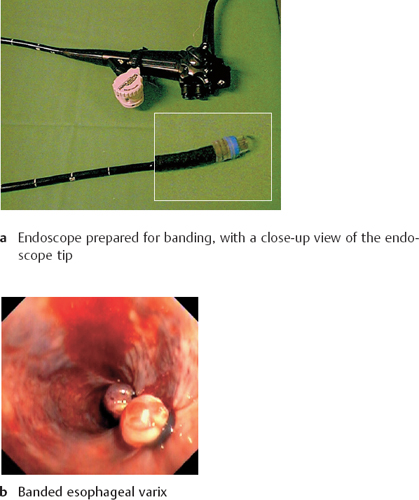
Fig. 4.14 Banding of esophageal varices
Aftercare
 Repeat three or four times at two-week intervals.
Repeat three or four times at two-week intervals.
 Reexamine at three months.
Reexamine at three months.
Complications
 Early: perforation of the hypopharynx or esophagus by the overtube
Early: perforation of the hypopharynx or esophagus by the overtube
 Late: strictures, stenoses
Late: strictures, stenoses
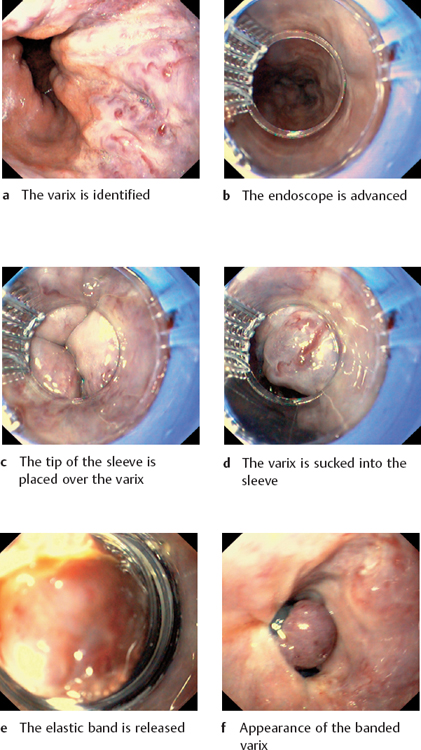
Fig. 4.15 Banding of esophageal varices
Sclerotherapy of Fundic Varices, TIPS, and Operative Treatment
Principle and Key Characteristics
 Principle: The varices are obliterated with a tissue adhesive.
Principle: The varices are obliterated with a tissue adhesive.
 Sclerotherapy with cyanoacrylate (Histoacryl) is the treatment of choice for fundic varices (Fig. 4.16).
Sclerotherapy with cyanoacrylate (Histoacryl) is the treatment of choice for fundic varices (Fig. 4.16).
Materials
 Endoscope
Endoscope
 Suction pumps
Suction pumps
 Water jet
Water jet
 Disposable sclerotherapy needles, 6 mm long with 0.7 mm outer diameter
Disposable sclerotherapy needles, 6 mm long with 0.7 mm outer diameter
 Histoacryl
Histoacryl
 Lipiodol
Lipiodol
 Protective eyewear
Protective eyewear
 Distilled water
Distilled water
 Silicone oil
Silicone oil
 Technique
Technique
 Use protective eyewear.
Use protective eyewear.
 Draw Histoacryl and Lipiodol (1:1) into a 2-mL syringe.
Draw Histoacryl and Lipiodol (1:1) into a 2-mL syringe.
 Flush the sclerotherapy needle with distilled water (Histoacryl polymerizes on contact with electrolytes).
Flush the sclerotherapy needle with distilled water (Histoacryl polymerizes on contact with electrolytes).
 Introduce silicone oil into the working channel.
Introduce silicone oil into the working channel.
 Insert the syringe.
Insert the syringe.
 Inject 0.5-1 mL into the varix.
Inject 0.5-1 mL into the varix.
 Flush with water.
Flush with water.
 Retract the needle into the plastic sleeve, and wait one minute for the Histoacryl to polymerize before completely withdrawing the needle through the endoscope.
Retract the needle into the plastic sleeve, and wait one minute for the Histoacryl to polymerize before completely withdrawing the needle through the endoscope.
 If this is unsuccessful, insert a Linton-Nachlas tube.
If this is unsuccessful, insert a Linton-Nachlas tube.
Complications
 Histoacryl embolism
Histoacryl embolism
 Sclerotherapy ulcer
Sclerotherapy ulcer
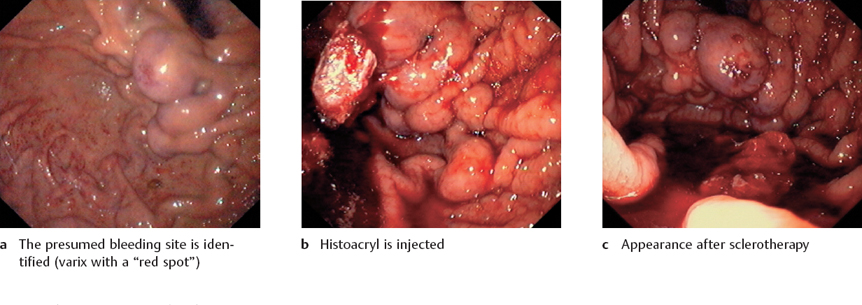
Fig. 4.16 Sclerotherapy of fundic varices with Histoacryl
 Transjugular Intrahepatic Portosystemic Shunt (TIPS)
Transjugular Intrahepatic Portosystemic Shunt (TIPS)
Principle and Key Characteristics (Fig. 4.17)
 Principle: A connection is established between the hepatic vein and intrahepatic portal vein branch.
Principle: A connection is established between the hepatic vein and intrahepatic portal vein branch.
 A puncture needle is passed to the right hepatic vein through a transjugular catheter, and the intrahepatic portal vein branch is punctured. The puncture tract is dilated and then stabilized with an expanding stent.
A puncture needle is passed to the right hepatic vein through a transjugular catheter, and the intrahepatic portal vein branch is punctured. The puncture tract is dilated and then stabilized with an expanding stent.
 Last recourse for refractory bleeding.
Last recourse for refractory bleeding.
 Operative Treatment
Operative Treatment
Principle and Key Characteristics
 Principle: surgical creation of a portosystemic anastomosis.
Principle: surgical creation of a portosystemic anastomosis.
 Not practical in emergency situations.
Not practical in emergency situations.
 Considerably higher mortality compared with TIPS.
Considerably higher mortality compared with TIPS.
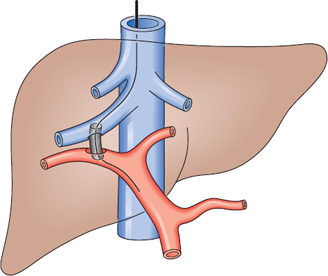
Fig. 4.17 Schematic diagram of TIPS placement. The shunt establishes a connection between the hepatic vein and portal vein
Bleeding Ulcers: Nonoperative Therapies
 Incidence and Symptoms
Incidence and Symptoms
Fifty percent of all acute upper gastrointestinal hemorrhages are caused by a bleeding ulcer (Fig. 4.18). It is estimated that approximately 20% of all patients with recurrent gastric or duodenal ulcers experience bleeding. This may be an oozing hemorrhage with gradual progression of anemia or may present as an acute, massive, life-threatening hemorrhage.
The symptoms are variable and may be very subtle, particularly in NSAID users. Approximately 80 % of bleeding ulcers will stop bleeding spontaneously, and 20 % of those will rebleed. The mortality rate is 6-15 %. Acute bleeding can be successfully controlled by endoscopic treatment in over 85 % of cases. The risk of recurrence after primary hemostasis is 20-25%.
 Nonoperative Treatment Methods
Nonoperative Treatment Methods
The following nonoperative treatment modalities are used:
 Pharmacological therapy
Pharmacological therapy
 Endoscopic techniques
Endoscopic techniques
– Injection therapy: epinephrine, physiological saline solution, polidocanol, ethanol, fibrin glue
– Hemostatic clips
– Thermal methods: laser, electrocoagulation, argon plasma coagulation
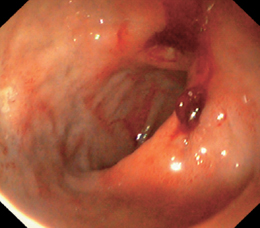
Fig. 4.18 Bleeding gastric ulcer
 Indications for Endoscopic Treatment
Indications for Endoscopic Treatment
The Forrest classification is used in selecting patients for endoscopic treatment (Table 4.9; Figs. 4.19, 4.20). Treatment is indicated for Forrest classes Ia and Ib, which are actively bleeding lesions, and for a high percentage of recurrent ulcers of class IIa. For class IIb lesions, an effort is made to flush away the adherent clot. If this is successful, the treatment decision is based on the new finding. Removing the clot may induce active bleeding, leave a “visible vessel,” or expose a hematin- or fibrin-covered ulcer base.
If the bleeding cannot be controlled endoscopically, prompt operative treatment is indicated.
| Class | Bleeding activity | Risk of rebleeding (%) |
|---|---|---|
| I | Active bleeding | |
| Ia | Spurting hemorrhage Oozing hemorrhage | 90 |
| Ib | Oozing hemorrhage | 30 |
| II | Signs of hemorrhage without active bleeding | |
| IIa | Visible vessel | 50–100 |
| IIb | Adherent clot | 20 |
| IIc | Hematin on ulcer base | <5 |
| III | Ulcer base with no signs of bleeding | <5 |
Forrest Class I-IIa lesions are an indication for endoscopic treatment
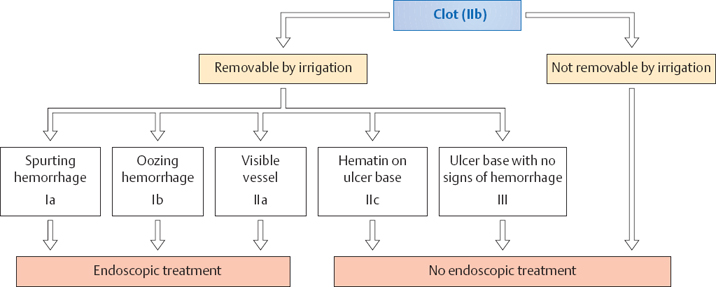
Fig. 4.19 Flowchart for management of an adherent clot
Bleeding Ulcers: Forrest Classification
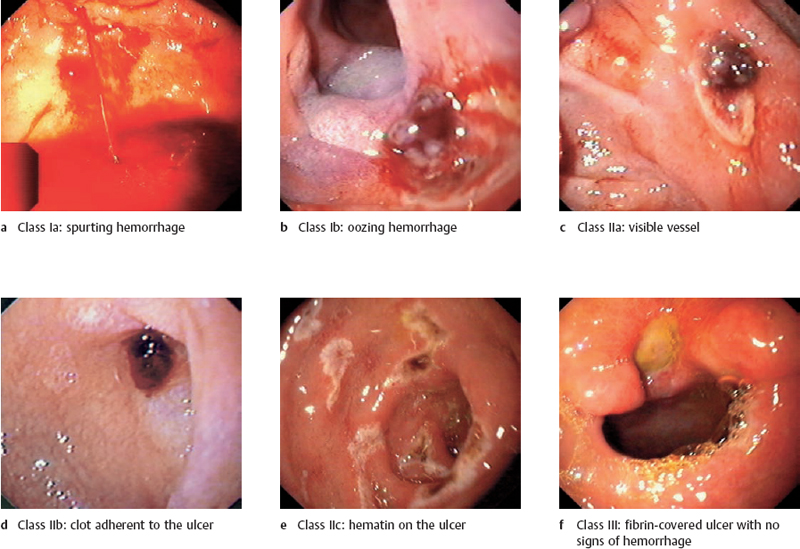
Fig. 4.20 Forrest classification of acute ulcer bleeding
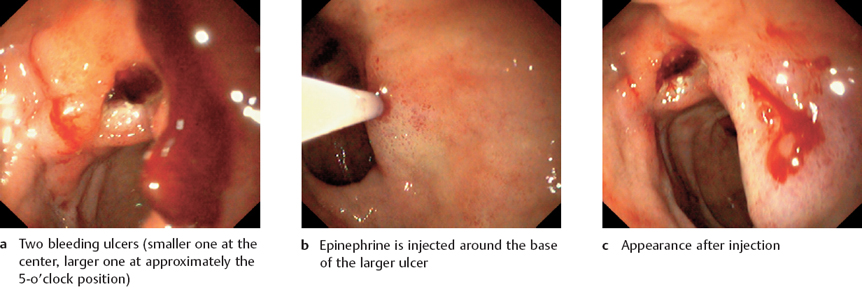
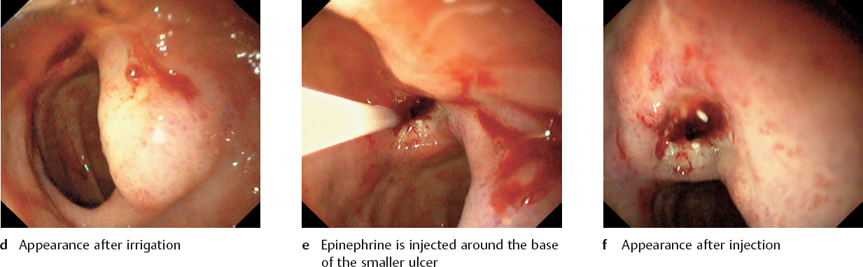
Fig. 4.21 Epinephrine injection for acute ulcer bleeding
Bleeding Ulcers: Pharmacological Therapy and Injection Techniques
 Pharmacological Therapy of Bleeding Ulcers
Pharmacological Therapy of Bleeding Ulcers
Hemostasis cannot be achieved with medical therapy alone. PPI are used, but their benefit is still unproved. If H. pylori is detected, eradication therapy should be performed. This can expedite healing and lower the risk of recurrence. NSAIDs should be discontinued.
 Endoscopic Techniques
Endoscopic Techniques
The treatment of choice is endoscopic hemostasis (injection therapy, hemoclips, thermal methods).
 Injection Therapy
Injection Therapy
Key Characteristics
 Epinephrine
Epinephrine
– Therapy of choice
– Safe, economical, can be used to treat rebleeding after prior hemostasis with polidocanol
 Polidocanol
Polidocanol
– Very effective, especially after initial use of epinephrine
– Problem: enlarges tissue lesion, should not be used to treat rebleeding
– Agent of second choice
 Fibrin glue
Fibrin glue
– Two components (fibrin and thrombin) form a fibrin clot when mixed together. They are mixed at the time of injection.
– Excellent tissue compatibility; very costly, laborious technique
– Very effective for rebleeding
 Physiological saline solution, glucose, ethanol
Physiological saline solution, glucose, ethanol
– Very rarely used today as a solitary treatment
Materials
 Endoscope
Endoscope
 Suction pumps
Suction pumps
 Water jet
Water jet
 Single-lumen injection needles for epinephrine and polidocanol, double-lumen needles for fibrin glue
Single-lumen injection needles for epinephrine and polidocanol, double-lumen needles for fibrin glue
 Epinephrine 1:10 000 in physiological saline solution, 1 % polidocanol, fibrin glue
Epinephrine 1:10 000 in physiological saline solution, 1 % polidocanol, fibrin glue
 Technique
Technique
 Epinephrine (Fig. 4.21)
Epinephrine (Fig. 4.21)
- – Make several injections of 1 mL each around the bleeding ulcer.
- – Then inject 1-2 mL into the bleeding site at the ulcer base.
- – Make several injections of 1 mL each around the bleeding ulcer.
 Polidocanol
Polidocanol
- – Inject 1 mL of polidocanol into the bleeding site.
- – Caution: Inject no more than 2 mL per ulcer; more could cause a substantial tissue lesion.
- – Inject 1 mL of polidocanol into the bleeding site.
 Fibrin glue
Fibrin glue
- – Preflush the needle with physiological saline solution.
- – Inject 2 mL of both components into the bleeding site through a double-lumen needle.
- – Then flush the needle with physiological saline solution.
- – Preflush the needle with physiological saline solution.
Bleeding Ulcers: Hemoclip Application and Thermal Methods
 Hemoclip Application
Hemoclip Application
Principle and Key Characteristics
 Principle: compression of the lesion or bleeding vessel with a metal clip
Principle: compression of the lesion or bleeding vessel with a metal clip
 Safe, appears as effective as injection therapy, causes no tissue damage, relatively low cost
Safe, appears as effective as injection therapy, causes no tissue damage, relatively low cost
 Excellent for treating “visible vessels” and arterial hemorrhages, Dieulafoy ulcer, and bleeding after polypectomies
Excellent for treating “visible vessels” and arterial hemorrhages, Dieulafoy ulcer, and bleeding after polypectomies
Materials
 Endoscope
Endoscope
 Suction pumps
Suction pumps
 Water jet
Water jet
 Hemoclips with applicator
Hemoclips with applicator
 Technique
Technique
 Load the hemoclip onto the applicator and insert.
Load the hemoclip onto the applicator and insert.
 Apply the hemoclip to the bleeding vessel.
Apply the hemoclip to the bleeding vessel.
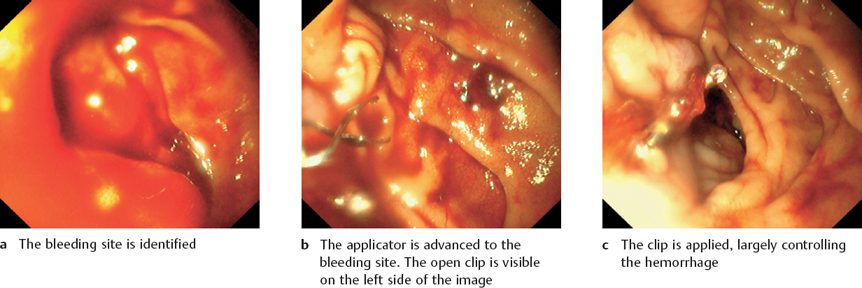
Fig. 4.22 Clipping of a bleeding gastric ulcer
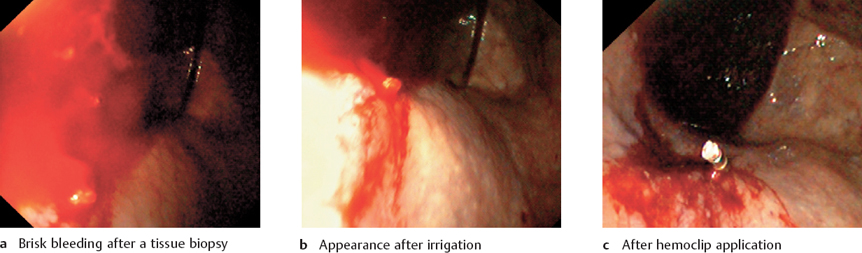
Fig. 4.23 Clipping of a bleeding biopsy site
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


