Interpreting Fundus Autofluorescence
Alan C. Bird
Interpretation of autofluorescence (AF) images with illumination at 488 nm (standard AF image) is based on the principle that the majority of the signal is derived from lipofuscin in the retinal pigment epithelium (RPE) (see Chapter 3) (1, 2, 3). Although there are many fluorophores in the retina, the signal from RPE lipofuscin is stronger than that from any other substance. The quantity of lipofuscin in the RPE is a balance between accumulation and clearance. Lipofuscin is formed of retinal and ethanolamine in the photoreceptor outer segment and is ingested by the RPE by phagocytosis of shed outer segment material (see Chapter 2) (4,5). Thus, accumulation of lipofuscin is driven by outer segment renewal. Clearance of lipofsucin may be due in part to discharge of long-term phagolysosomes by the RPE into the extracellular space (see Chapter 2) and in part to photodegradation (6), although the half life of the fluorophores is unknown. Thus, the “background” levels of AF in the normal healthy eye reflect a normal photoreceptor outer segment turnover and retinoid cycling. A reduction in the number of photoreceptors causes loss of AF over time. Increased levels of AF are caused by RPE dysfunction either because of an intrinsic failure of lipofuscin clearance or the presence of an abnormal metabolic load.
Imaging of AF depends on the clarity of the media. Extravascular blood internal to the RPE will prevent detection of the signal, and nuclear sclerosis will attenuate illumination. Under other circumstances, the variation reflects the lipofuscin content of the RPE. The image of a normal fundus with illumination at 488 nm shows homogeneous AF over most of the posterior pole (see Chapters 2 and 9) (2). The blood vessels and fovea are dark because of light absorption by blood and luteal pigment, respectively, since both absorb short wavelength light. The optic disc is dark because of the absence of a fluorophore. The AF level increases with age and tends to be highest at about 10 degrees of eccentricity (see also Chapter 3). Deviation from this pattern indicates outer retinal disease. Current imaging techniques with commercially available systems are very valuable for detecting abnormalities in the distribution of AF, but are relatively unreliable for measuring absolute levels of AF (see Chapter 5). Described below are the circumstances in which evaluation of fundus AF is the most valuable.
CONTINUITY OF AUTOFLUORESCENCE (NORMAL AUTOFLUORESCENCE PATTERN)
In the presence of unexplained loss of vision, the existence of normal AF with illumination of 488 nm usually implies that the loss of vision is unlikely to be due to outer retinal disease. However, there are certain circumstances in which normal AF is present in cases of outer retinal disease. This was observed in a study of patients with Leber congenital amaurosis (7) (see also Chapter 11D) (Fig. 7.1), in which it was concluded
that photoreceptor cell dysfunction occurred without population loss. The loss of vision may be due to transduction failure or constant noise, i.e., the photoreceptor cells may behave as if they are in constant light, thus reducing signal-to-noise ratios. If it were possible to correct the metabolic abnormality, AF imaging suggests that such patients might be able to recover vision. A similar situation of loss of function with normal AF signal was found in acute zonal and occult outer retinopathy (AZOOR), at least in the first 5 years of disease, implying the possibility of spontaneous recovery (8). In some patients with retinitis pigmentosa (RP), there is a ring of increased AF at variable eccentricity around the fovea (see also Chapter 11A) (Fig. 7.2) (9,10). On either side of the ring of increased AF, AF is normal but scotopic function is markedly reduced; photopic function is also reduced in areas external to the ring of increased AF. There is no explanation as to why the function is poor in the presence of a normal population
of photoreceptor cells unless the half life of the fluorophores is very long. Curiously, near-infrared AF (NIA) coincides with function (see also Chapter 6).
that photoreceptor cell dysfunction occurred without population loss. The loss of vision may be due to transduction failure or constant noise, i.e., the photoreceptor cells may behave as if they are in constant light, thus reducing signal-to-noise ratios. If it were possible to correct the metabolic abnormality, AF imaging suggests that such patients might be able to recover vision. A similar situation of loss of function with normal AF signal was found in acute zonal and occult outer retinopathy (AZOOR), at least in the first 5 years of disease, implying the possibility of spontaneous recovery (8). In some patients with retinitis pigmentosa (RP), there is a ring of increased AF at variable eccentricity around the fovea (see also Chapter 11A) (Fig. 7.2) (9,10). On either side of the ring of increased AF, AF is normal but scotopic function is markedly reduced; photopic function is also reduced in areas external to the ring of increased AF. There is no explanation as to why the function is poor in the presence of a normal population
of photoreceptor cells unless the half life of the fluorophores is very long. Curiously, near-infrared AF (NIA) coincides with function (see also Chapter 6).
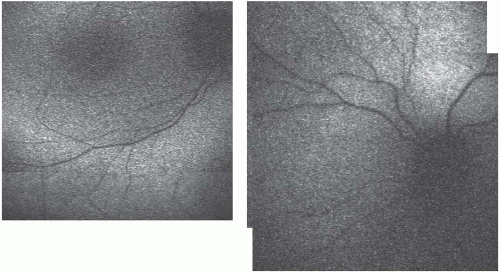 FIGURE 7.1. AF images of the right and left eyes of a 16-year-old female with Leber congenital amaurosis who had light perception vision throughout life and a flat electroretinogram in the first year of life. |
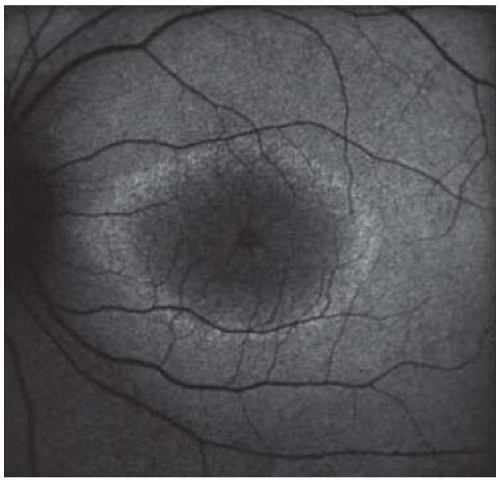 FIGURE 7.2. AF image of a 32-year-old male with RP showing a ring of increased AF around the fovea and cystoid macular edema. |
AF is also very important for determining the integrity of the outer retina at the time of treatment of choroidal neovascularization (CNV). Until recently, poor visual acuity was interpreted as indicating loss of central photoreceptor cells, but recovery of visual acuity following intravitreal injection of antivascular endothelial growth factor (VEGF) agents implies that this is not the case. Further support for the concept that the outer retina may be physically intact comes from the observation of normal AF in such cases (see also Chapter 10B) (Fig. 7.3) (11,12). AF imaging would be of great value for assessing the likely therapeutic benefit of such treatments.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


