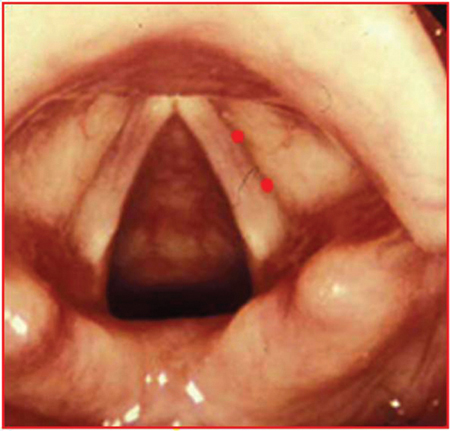
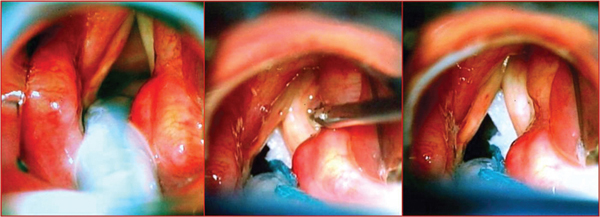
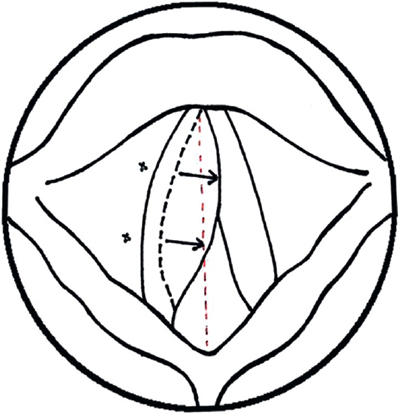
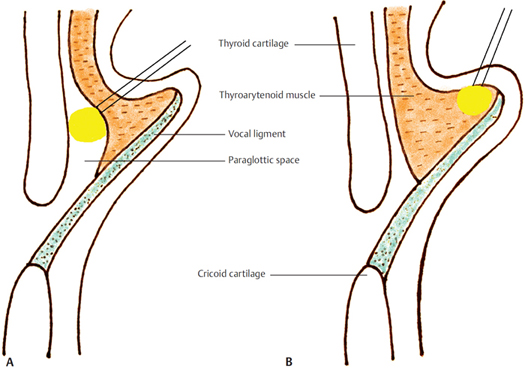
14 Injection Medialization Procedures for the Vocal Fold Injection medialization aims to establish vocal fold approximation to achieve airway protection and to improve the voice quality in patients suffering from inadequate glottic closure. In small defects (typically <1 mm), the opposite vocal fold may adequately compensate following speech therapy, and surgical intervention can be avoided. For larger defects or for those patients refractory to speech therapy, vocal fold injection or formal laryngeal framework surgery may be considered. The ultimate goal of treatment is to bring the edge of the nonfunctioning vocal fold closer to the midline to facilitate glottal closure during phonation and swallowing by allowing the functioning vocal fold to approximate to the nonfunctioning side more easily. Laryngeal framework surgery has been discussed elsewhere. In this section, the alternative use of injection laryngoplasty to achieve vocal fold medialization will be discussed. Conditions for which vocal fold injection procedures may be considered include •Vocal fold paralysis and paresis •Vocal fold atrophy •To augment laryngeal framework surgery •Presbylarynx The first report of the procedure was published by Brunings in 1911. He described using paraffin via a direct laryngoscopic approach under local anesthetic.1 Over the last century, the procedure has evolved and now provides a safe, effective, and reliable method for providing voice improvement in certain patients with defective glottic closure. Injection techniques offer anterior glottic approximation for small-to-medium-sized defects (up to 3 mm) and have the potential advantage of straightening small irregularities in the free edge of the vocal fold depending on the material used. The procedure is generally quick and provides immediate results. Potential disadvantages include airway compromise secondary to over-injection, migration, and foreign body reaction with granuloma formation. In this section, we will address the options for treatment and describe the various injectable materials that may be considered. For each option, the specific advantages and disadvantages will be discussed. As always, each patient presents a unique set of circumstances that must be considered when contemplating injection laryngoplasty. Patient selection will depend on numerous factors, including comorbidities, surgical access issues, and patient expectations. A thorough history and examination is paramount to establish an accurate diagnosis, and the injectable material used will differ depending on the underlying cause of glottic insufficiency. The tolerance to procedures under local anesthetic is also very important when considering local versus general anesthetic techniques. Some patients may benefit from a “trial” injection with a short-term, absorbable material before considering more permanent treatments. Several techniques are available and must be tailored to suit the individual patient requirements and the experience of the surgeon. In general, operative methods may be subdivided into endoscopic and percutaneous techniques. The choice of injectable material used will depend on the desire for a temporary or permanent treatment, diagnosis, availability of materials, experience, and cost. Where possible, injections should be performed under local anesthetic as this allows immediate auditory feedback and may avoid airway compromise from over-injection. However, endoscopic treatment under general anesthetic will be required for patients who are unable to tolerate the procedure while awake. The site of injection is dependent on the clinical indication. Superficial injection of a substance into the lamina propria may be indicated for vocal fold scarring and lamina propria defects, with the aim of correcting vibratory defects. More commonly, the injection will be directed deeper and more laterally into the thyroarytenoid/lateral cricoarytenoid complex to achieve vocal fold augmentation. This method results in medialization of the affected fold in a similar way to type 1 thyroplasty (Figs. 14.1 and 14.2). Lateral injection may be used to correct mild-to-moderate glottal insufficiency (1 to 3 mm glottal gaps).2 Figure 14.1 A schematic diagram demonstrating the site of injection (thyroarytenoid/lateral cricoarytenoid complex) to medialize anterior vocal fold. Most commonly, endoscopic procedures are performed under general anesthetic via formal suspension laryngoscopy with a small tube or jet ventilation. This allows a controlled setting with a full array of microsurgical instruments and high-definition endoscopic visualization of static vocal folds (Fig. 14.3). It is also possible to perform a direct laryngoscopy in an awake, sedated patient with a small laryngoscope using telescopic visualization without the need for formal general anesthetic. Figure 14.2 Photograph demonstrating the site of injection to achieve right vocal fold medialization. The volume of injection may be difficult to judge due to lack of patient feedback via phonation under general anesthesia.3 Over-injection may lead to airway compromise and this may only become apparent when the patient is extubated. Underinjection risks an inadequate result and the need for a repeat procedure. In addition to the usual anesthetic risks, access may prove difficult using this technique due to anatomical factors and cervical spine problems. A common error when performing this technique is unintentional superficial injection into the super ficial lamina propria of the vocal fold. This results in scarring and may adversely affect the mucosal wave with consequent compromise of vocal outcomes (Fig. 14.4). Figure 14.3 Intraoperative photographs to demonstrate successful endoscopic medialization. Figure 14.4 Site of injection for direct laryngoscopy. (A) Correct position (deep) into paraglottic space used for medialization. (B) Superficial injection may be used to map scarring and deliver therapeutic drugs, this is unsuitable for medialization as it distorts the mucosal wave. Clinical Pearls and Tips Ensure that the injection needle is fully loaded with the implant material till the needle tip to prevent any false medialization with air. Stabilization of the vocal folds with neurosurgical patties placing the patties under the affected fold is helpful in preventing the “hammock effect.” The implant material is optimally distributed to achieve medialization in the stabilized position. The patties also prevent any accidental spill and inhalation of the implant material in the airways. Vocal fold injections can be performed as “office procedures”. Please refer to Section C, Chapter 4 for a detailed description of the techniques. In an awake patient, under topical local anesthesia, per-oral injection may be performed with a curved needle under flexible endoscopic guidance. The patient adopts a “sniffing the morning air” position (neck flexed, head slightly extended) and protrudes their tongue. The needle (typically 220 to 250 mm length) is inserted via the mouth and passed into the vocal fold following retraction of the false vocal fold with the needle shaft.2 Flexible endoscopic injections may be performed under local anesthesia and recently, some surgeons have described using flexible endoscopes (e.g., via transnasal esophagoscopy setup) through the mouth or nose with a side port from which injection may be performed following appropriate topical anesthetic. This method is technically demanding in an awake patient and requires specialist experience and advanced equipment. Large amounts of the injectable material may be required to account for the dead space in the long injection catheters, further increasing potential costs. This technique uses a transcutaneous injection under direct visualization with a flexible nasoendoscope in an awake patient. The use of modern chip-tip endoscopes provides excellent image resolution to allow accurate placement of the injection. With experience, outcomes of percutaneous techniques match those of direct laryngoscopic approaches.4,5 There are several advantages in using this technique, in particular, the opportunity for direct auditory feedback from the patient during the injection. This technique may also be preferred for patients too frail or elderly to tolerate general anesthesia. Patient selection is crucial, and a calm, cooperative patient without a strong gag reflex is required. A concern with percutaneous approaches is a lack of accuracy in needle placement when compared with direct laryngoscopic methods. The injection needle may be inserted trans-cricothyroid, trans-thyrohyoid membrane, or trans-thyroid cartilage.2,6–8 For each approach, the injection effect can be directly monitored by the operating surgeon both visually via a transnasal endoscope and also by monitoring auditory changes during phonation. This also lessens the risk of over-injection as airway compromise can be immediately detected (Fig. 14.5). A needle is inserted below the inferior border of the thyroid cartilage, from 3 to 7 mm lateral to the midline and the directed superolaterally in the submucosal tissues. Alternatively, the needle may be inserted in the midline below the vocal folds and aimed superolaterally across the tracheal lumen to penetrate the deep vocal fold (Fig. 14.6). The injection needle is inserted at right angles to the thyroid ala 3 to 5 mm above the inferior border. Gentle pressure medially is assessed endoscopically to confirm needle position before injection. This approach may be difficult with heavily calcified cartilages in older patients. Figure 14.5 Over-injection of left vocal fold causing medial bowing.
Aims
Indications
Background
Patient Selection
Techniques
Approaches
Endoscopic Injection
Direct Laryngoscopy
Per-Oral Injection
Flexible Endoscopic Injection
Percutaneous Injection
Trans-Cricothyroid
Trans-Thyroid

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


