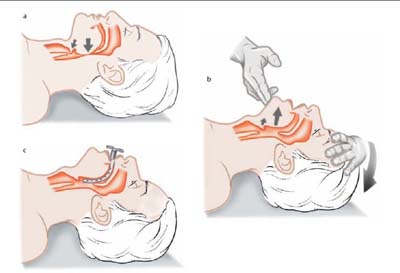
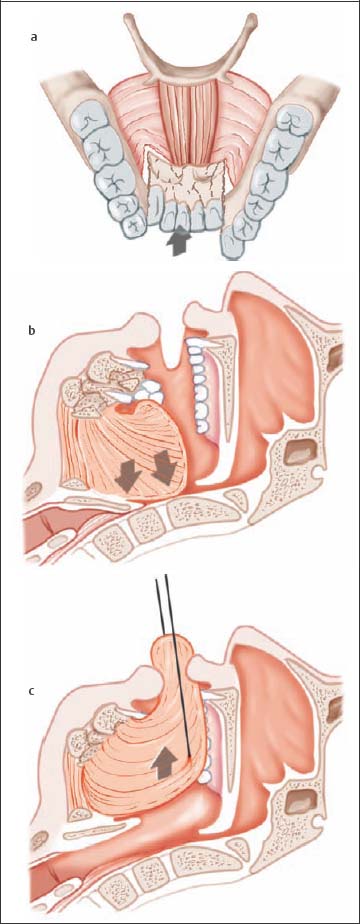
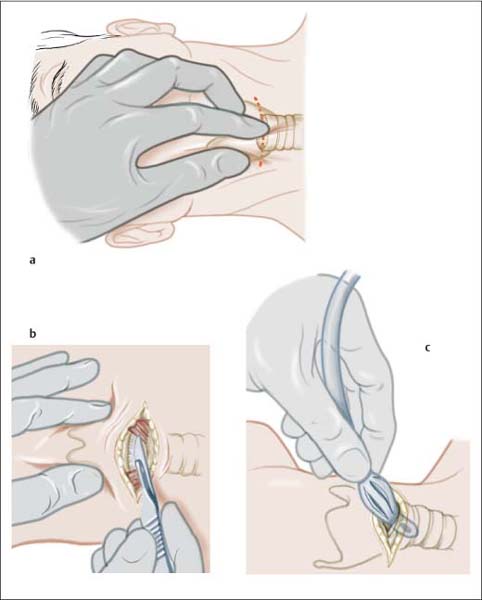
1 Initial Management In areas where rapid access to medical care is ensured, persons arriving at the scene normally need only to call the paramedics and wait for their arrival. Securing the scene of the accident has absolute priority over further measures in order to protect the injured individual, motorists, and other persons administering aid. Vital signs should always be determined first as a means of initial assessment: Obstruction of the upper airways is the greatest threat in patients with head and neck injuries. The jaw-thrust and chin-lift maneuvers (Fig. 1.1) are the simplest means of stabilizing the airways. Foreign bodies (dentures, mucus, and vomitus) must be removed from the oral cavity using a finger. More proximal airways should be cleaned by suction if possible. Intubation with pharyngeal tubes is another possibility for securing the airways (Guedel tube, Wendel tube; Fig. 1.1c). For complex injuries, transport to a regional trauma center is essential. If associated injury of the neurocranium is suspected, early orotracheal intubation should be performed. It is imperative that treatment of shock begin at the scene. Initial management includes: Massive hemorrhage should be managed with direct compression. Ligation of the extremities should be avoided, however, and the exact time that compression began must be noted. Cardiopulmonary resuscitation should be performed if necessary. Soft tissue injuries should be covered with a sterile bandage to help control bleeding and protect the wound from additional contamination. Penetrating foreign bodies should be removed only after the patient is in a clinical setting. If cervical spine injury is suspected, rotation or hyperextension of the patient’s neck must be avoided. If removal of a motorcycle helmet at the scene is necessary in order to control the airways, a second person must stabilize the cervical spine using traction. Then, a rigid cervical collar must be applied until cervical spine injury has been excluded. After emergent care procedures are complete, further treatment should take place in a specialized properly equipped trauma center. This is especially important for complex injuries. The patient should only be moved after stabilization of vital functions. Fig. 1.1 Obstruction of the upper airways caused by fall-back of the tongue and epiglottis (modified from Eisele and McQuone 2000). a Laxity of the tongue musculature causing it to obstruct the upper airways. b Tilting the head to dorsal and applying pressure to the chin assures the patency of the airways. c Positioning a Guedel tube to secure the upper airways. Establishment and maintenance of the airways is of the utmost urgency in treating any multiply injured patient with craniofacial trauma. It is important to remember that following an accident, even airways with adequate ventilation can quickly become obstructed by blood or swelling. A particular problem of craniofacial injury is the fall-back of the tongue in segmental fractures of the mandible, especially those involving the midface. The continuity of the horseshoe-shaped mandible, to which the tongue is attached, is disrupted and the injured individual is no longer able to maintain the position of the tongue to keep the airways open (Fig. 1.2). In an emergency, one can attempt to place the patient in the lateral position or to advance the fractured mandibular arch manually. If the patient is unconscious, a suture can be placed through the posterior of the tongue, lifting the tongue and pulling it forward (Fig. 1.2c). Oral intubation follows. Successfully positioning the larynx is usually unproblematic, despite hemorrhage and swelling, as the tongue base loses its supporting buttress as a result of mandibular injury. Fig. 1.2 Obstruction of the upper airways in a mandibular fracture. a Dorsal displacement of the mandibular arch and tearing of the musculature of the floor of the mouth and tongue. b Fall-back of the tongue due to loss of fixation on the mandible. c Emergency procedure for advancing the tongue using a suture to establish the airways. Specific problems related to injury of the larynx and trachea can arise and should be expected: In an emergency, tracheotomy is always preferable to intubation. Cricothyrotomy involves creating an opening in the cricothyroid membrane, which covers the area between the thyroid lamina and the cricoid cartilage. The emergency cricothyrotomy kits available today belong to standard paramedic equipment: If an emergency kit is not available, a horizontal incision is made over the cricothyroid membrane. A blade with suitable dimensions is advanced directly into the trachea. The blade is not removed, but instead is rotated, thus serving to guide a speculum or catheter for placing the tube. Fig. 1.3 Cricothyrotomy (modified from Eisele and McQuone 2000). a Palpation of the cricoid cartilage; an incision is made at its superior border. b A suitably sized blade is used to penetrate the cricothyroid membrane and is advanced in the trachea, where it is then rotated. c Intubation occurs through the opening created into the trachea.
 Checklist Initial Evaluation, Chapter 3, p. 15
Checklist Initial Evaluation, Chapter 3, p. 15
 Checklist Initial Management, Chapter 3, p. 15
Checklist Initial Management, Chapter 3, p. 15
First Aid at the Scene
Evaluation of Vital Functions
 Neurologic status is evaluated on the basis of the patient’s response when spoken to and to pain.
Neurologic status is evaluated on the basis of the patient’s response when spoken to and to pain.
 The Glasgow Coma Scale (GCS; Table 5.1, p. 39) is necessary for further clinical assessment.
The Glasgow Coma Scale (GCS; Table 5.1, p. 39) is necessary for further clinical assessment.
 Respiratory status is evaluated based on observation of breathing pattern and respiratory rate.
Respiratory status is evaluated based on observation of breathing pattern and respiratory rate.
 Circulation can be evaluated by palpating the carotid pulse.
Circulation can be evaluated by palpating the carotid pulse.
Stabilizing Vital Functions
Stabilizing Circulation
 elevation of the patient’s legs (autotransfusion);
elevation of the patient’s legs (autotransfusion);
 intravenous administration of a colloidal volume substitute;
intravenous administration of a colloidal volume substitute;
 adequate pain management;
adequate pain management;
 protection from hypothermia.
protection from hypothermia.
Emergency Care
Emergency Measures
Airways
Fall-Back of the Tongue
Injuries of the Larynx and Trachea
 Extensive injury of the larynx often renders oral intubation impossible; intubation should never be forced under such circumstances as manipulation can permanently obstruct any remaining space in the larynx. In rare cases, intubation can be attempted using a stiff tube.
Extensive injury of the larynx often renders oral intubation impossible; intubation should never be forced under such circumstances as manipulation can permanently obstruct any remaining space in the larynx. In rare cases, intubation can be attempted using a stiff tube.
 Cricothyrotomy is not advisable due to possible existing concomitant injury of the cricoid cartilage or cricoid lamina.
Cricothyrotomy is not advisable due to possible existing concomitant injury of the cricoid cartilage or cricoid lamina.
 In penetrating injuries of the trachea or larynx, the injury site should be used for intubation (Fig. 23.2a, p. 208).
In penetrating injuries of the trachea or larynx, the injury site should be used for intubation (Fig. 23.2a, p. 208).
 If tracheal rupture is suspected, intubation should be accomplished using a flexible endoscope or by means of primary tracheotomy. The endoscope is advanced under visualization past the tracheal injury and the tube is positioned inferior to the injury site. The tube should not be too large as this can result in further displacement of the ruptured trachea (Fig. 14.5, p. 126).
If tracheal rupture is suspected, intubation should be accomplished using a flexible endoscope or by means of primary tracheotomy. The endoscope is advanced under visualization past the tracheal injury and the tube is positioned inferior to the injury site. The tube should not be too large as this can result in further displacement of the ruptured trachea (Fig. 14.5, p. 126).
Cricothyrotomy
 The cricoid cartilage is palpated and the slight indentation above it is punctured with a needle.
The cricoid cartilage is palpated and the slight indentation above it is punctured with a needle.
 If the needle comes into contact with the thyroid cartilage, it can be used to guide the needle to the cricothyroid membrane. The needle tip then points in the direction of the jugular and is directed downward to the palpable gap and then advanced through the cricothyroid membrane (Fig. 1.3).
If the needle comes into contact with the thyroid cartilage, it can be used to guide the needle to the cricothyroid membrane. The needle tip then points in the direction of the jugular and is directed downward to the palpable gap and then advanced through the cricothyroid membrane (Fig. 1.3).
 Following cardiopulmonary resuscitation, a cricothyrotomy should be transformed into a tracheotomy as it will otherwise result in permanent damage to the larynx after a few days.
Following cardiopulmonary resuscitation, a cricothyrotomy should be transformed into a tracheotomy as it will otherwise result in permanent damage to the larynx after a few days.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


