Infranuclear Disorders of Eye Movement
Joel S. Glaser
R. Michael Siatkowski
Hilda Capo
Neuroanatomy
The supranuclear control of eye movements is discussed in detail in Chapters 9 and 10. However, for purposes of review it should be recalled that supranuclear ocular motor pathways descend from the cerebral hemispheres, decussate in the caudal midbrain, and terminate in the pontine horizontal gaze complex (Fig. 12.1). From here, the motor nuclei of the ocular muscles are integrated by way of the medial longitudinal fasciculus.
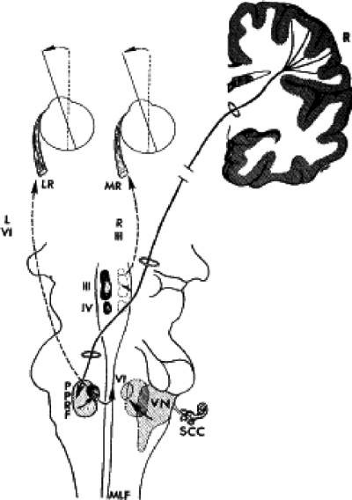 Figure 12.1 Supranuclear oculomotor system. Conjugate horizontal gaze to left originates in right frontal optomotor cortex (R). Pathway descends in area of internal capsule, decussates at level of trochlear nucleus (IV) to synapse in left pontine paramedian reticular formation (PPRF). Via direct connection to abducens nucleus (VI; labeled on right side), left lateral rectus (LR) is innervated. From abducens nucleus via contralateral medial longitudinal fasciculus (MLF), impulse is directed to contralateral oculomotor nuclear complex (III; labeled on left side), then to right medial rectus (MR). VN, vestibular nuclear complex; SCC, semicircular canals. |
The nuclear complex of the third (oculomotor) nerve lies beneath the aqueductal gray matter of the rostral midbrain at the level of the superior colliculus (Fig. 12.2). The medial longitudinal fasciculus (MLF) passes just lateral to the oculomotor nuclei, and the fourth (trochlear) cranial nerve nucleus is contiguous caudally. The organization of the oculomotor nuclear complex into distinct motor cell pools subserving individual extraocular muscles was investigated by Warwick,1 from whose schema (Fig. 12.3) the following points are especially noteworthy: (a) both lid levators are served by a single dorsocaudal midline nucleus; (b) the motor cell pool of the superior rectus muscle sends fibers across to the contralateral oculomotor nerve; (c) a nucleus for convergence has been demonstrated in some primates; and (d) at the caudal aspect of the oculomotor complex is the trochlear nucleus, whose axons turn dorsally to cross in the anterior medullary velum and innervate the contralateral superior oblique. Therefore, the nuclear motor pools of the superior rectus and superior oblique muscles are contralateral to the eye that they move. Warwick proposed that each muscle (intrinsic and extrinsic) innervated by the oculomotor nerve is subserved by a single, circumscribed mass of cells called a subnucleus. Modern tracer techniques have, to date, confirmed this concept for all the extrinsic muscles except the medial rectus, which has three definable subnuclei2,3; there are also afferent fibers to the ipsilateral trigeminal ganglion. Results of elegant axonal tracer studies mapping the intricate connections of the visceral nuclei of the oculomotor complex have been summarized by Burde.4
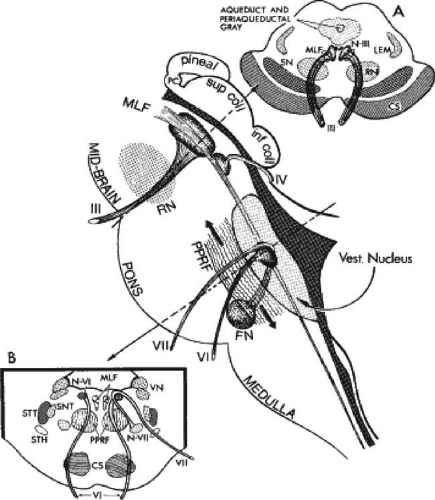 Figure 12.2 Diagrammatic section of brainstem. A: Cross-section at level of superior colliculus. NIII, oculomotor nucleus; MLF, medial longitudinal fasciculus; LEM, medial lemniscus; RN, red nucleus; SN, substantia nigra; CS, corticospinal tract. B: Cross-section at level of abducens nucleus (N-VI). PPRF, pontine paramedian reticular formation (note that reticular formation continues rostrally and caudally [arrows]); N-VII [FN], facial nucleus; VN, vestibular nuclear complex; SNT, spinal nucleus of trigeminal; STT, spinal tract of trigeminal; STH, spinothalamic tract. |
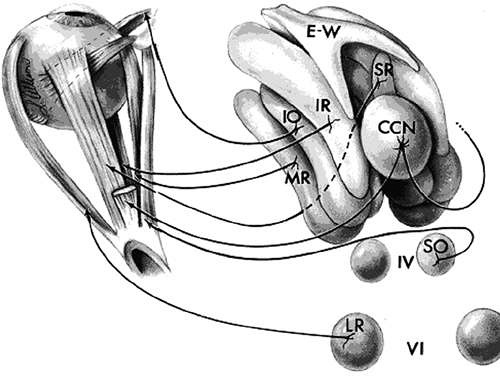 Figure 12.3 Organization of oculomotor nuclear complex viewed from above, left posterior. E-W, Edinger-Westphal parasympathetic subnucleus; subnuclei IR, inferior rectus; IO, inferior oblique; MR, medial rectus. Note that SR, superior rectus motor pool, is crossed, as is SO, superior oblique; CCN, caudal nucleus to both lid levators; LR, abducens nucleus for lateral rectus. Source: Adapted Warwick R: Representation of the extra-ocular muscles in the oculomotor complex. J Comp Neurol 98:449, 1953 |
From the oculomotor complex, the efferent fibers exit ventrally and pass through the red nucleus and medial aspect of the cerebral peduncles. The fascicles emerge in the interpeduncular space anterior to the midbrain as the paired oculomotor nerves. The oculomotor nuclei obtain their vascular supply from the terminal bifurcation of the basilar artery. Multiple arteries perforate the median mesencephalon in the interpeduncular space.
The sixth (abducens) nucleus is situated in the caudal portion of the paramedian pontine tegmentum, beneath the floor of the fourth ventricle (Fig. 12.2). Facial nerve fibers loop around the abducens nucleus before exiting in the cerebellopontine angle. This intimate relationship accounts for frequent concurrent damage seen clinically. Although lateral to the third nuclear complex in the rostral mesencephalon, the MLF passes medial to the abducens nucleus. There are two populations of neurons with cell bodies within the abducens nucleus.5,6 One group forms the sixth nerve; these abducens fibers pass ventrally to exit at the pontomedullary junction. The other internuclear neurons send fibers to join the contralateral MLF, with projection to the medial rectus subnucleus. Therefore, lesions involving the sixth nucleus produce ipsilateral conjugate gaze palsy (i.e., ipsilateral lateral rectus, contralateral medial rectus).7
The abducens, trochlear, and oculomotor nuclei are integrated via the MLF, which also has major connections with the vestibular nuclear complex (Fig. 12.1). Lesions involving the MLF typically result in internuclear ophthalmoplegia (see Chapter 10), which consists of faulty adduction of the ipsilateral eye (observed especially with attempted saccades) and often accompanied by dissociated nystagmus, greater in the abducting eye on attempted lateral horizontal gaze (Fig. 12.4). In addition, some degree of vertical nystagmus in upward gaze is often present, and skew deviation may account for vertical diplopia.8 Internuclear ophthalmoplegia, often bilateral, is by far the most common ocular motor disturbance of demyelinative origin. Unilateral ophthalmoplegia is more commonly due to a vascular incident, but bilateral involvement may be seen in brainstem infarction.9
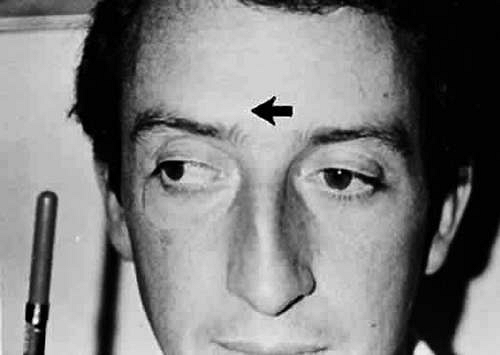 Figure 12.4 Left internuclear ophthalmoplegia. On attempted right gaze, the left eye fails to adduct due to lesion of left medial longitudinal fasciculus. |
The peripheral course of the third nerve is as follows (Fig. 12.5): as the nerve exits ventrally from the midbrain into the interpeduncular space, it passes beneath the origin of the posterior cerebral artery and lies parallel and lateral to the posterior communicating artery. Klintworth10 pointed out that, in instances where the basilar artery bifurcates at a low level, the oculomotor nerve may be angled downward at the point where the posterior cerebral artery crosses the nerve, and vascular grooving of the superior aspect of the nerve is present in approximately one-third of normal brains. The nerve runs between the free edge of the tentorium and the lateral aspect of the posterior clinoid, where it pierces the dura to enter the cavernous sinus. The oculomotor trunk occupies the superior aspect of the cavernous sinus (see ahead to Fig. 12.17) and separates into superior and inferior divisions 4 to 5 mm the superior orbital fissure. Fiber count of the superior division is about one-third that of the inferior,11 and it has been suggested that relative pupil sparing in cavernous sinus or orbital apex lesions may reflect preservation of the inferior branch. The inferior branch supplies the medial and inferior rect inferior oblique muscles, as well as parasympathetic root to the ciliary ganglion (pupil sphincter and ciliary muscle); the superior branch innervates the superior rectus and levator palpebrae.
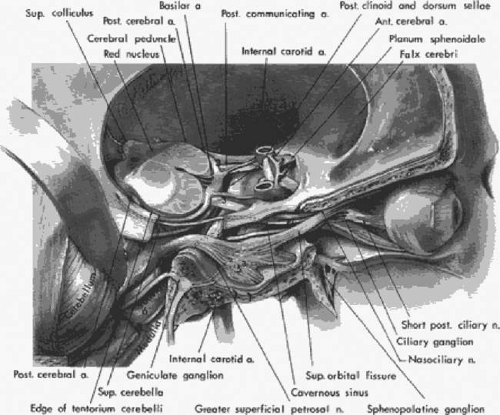 Figure 12.5 Representation of cranial nerves and related basal structures in the area of the midbrain, middle fossa, cavernous sinus, and orbital apex. The roof of the right orbit, sphenoid wing, floor of middle fossa, and petrous ridge have been sectioned; a section of the tentorial edge is removed to demonstrate the course of trochlear nerve (4). The cerebellum is retracted to show structures in the posterior fossa. Cross-section of the midbrain is at level of superior colliculi and red nuclei. (2, optic nerves and chiasm; 3, oculomotor nerves [note relationship to posterior cerebral and posterior communicating arteries]; 4, trochlear nerve in edge of tentorium; 5, trigeminal nerve [51, ophthalmic division; 52, maxillary division; 53, mandibular division]; 6, abducens nerve [note course up clivus and passage under petroclinoid ligament into posterior aspect of cavernous sinus]; 7, facial nerve; 8, acoustic nerve) |
According to Kerr,12 the pupillomotor fibers are superficial in the oculomotor nerve trunk, lying just internal to the epineurium. It is believed that this superficial position makes the pupillomotor fibers especially vulnerable to compression. In more anterior segments (e.g., cavernous sinus), however, pupillomotor fibers may be preferentially spared, even in the presence of total oculomotor palsy. t is likely that involvement or “sparing” of the pupil reflects the nature and acuteness of the lesion, rather than which specific segment of the oculomotor trunk is compromised.
The trochlear fascicles pass dorsally, lateral to the aqueduct, and the nerve exits the midbrain and crosses the contralateral fourth nerve in the anterior medullary velum, just caudal to the inferior colliculi. The fourth nerve is the only cranial nerve to exit the brainstem dorsally. The nerve continues laterally around the midbrain tectum, crosses the superior cerebellar artery, and reaches the free edge of the tentorium, where it enters the dura and runs forward into the cavernous sinus (Fig. 12.5). The fourth nerve enters the orbit through the superior orbital fissure, but above the annulus formed by the origin of the rectus muscles, and innervates only the superior oblique muscle.
The abducens nerve emerges from the brainstem at the lower border of the pons in the pontomedullary sulcus, approximately 1 cm from the midline. The nerve ascends the ventral face of the pons for a short distance, is crossed by the anterior inferior cerebellar artery, and pierces the dura of the clivus approximately 2 cm below the posterior clinoids (Fig. 12.5). The sixth nerve traverses or passes above the inferior petrosal sinus, runs beneath the petroclinoid ligament(Gruber), and enters the cavernous sinus. The sixth nerve lies freely within the body of the cavernous sinus, unlike the oculomotor and trochlear nerves that are supported in the lateral wall of the sinus. Some sympathetic fibers are briefly attached to the abducens, passing onward to the ophthalmic trigeminal.13 From the cavernous sinus, the nerve passes through the annular segment of the superior orbital fissure to innervate the lateral rectus.
Milisavljević et al.14 demonstrated penetration of oculomotor trunks by circumflex mesencephalic arteries or branches of the posterior cerebral perforating vessels, but clinical implications of such anatomic anomalies are not clear. According to the anatomic review by Lapresle and Lasjaunias,15 three arterial “systems” vascularize the cranial nerves: the inferolateral trunk arises from the intracavernous siphon of the internal carotid artery and nourishes cranial nerves III, IV, VI, and V-1; the middle meningeal system supplies nerves VII and V-2,3; and the ascending pharyngeal system supplies nerves IX through XII. The oculomotor nerve is also vascularized by the basilar artery system in the region of the posterior perforated substance, and in the supracavernous region by the artery of the free tentorial margin (Bernasconi). The clinical correlation of ischemic cranial neuropathies with these arterial territories is not entirely clear; however, neuroimaging has demonstrated that ischemic or “microvascular” cranial nerve palsies (i.e., mononeuropathies that spontaneously clear within several months) may occur anywhere along the course of the nerve, from the brainstem to the orbit.
Abducens Palsies
It is not proper to equate all lateral rectus malfunction with “sixth nerve palsy”: to do so confuses the issue and leads to inappropriate diagnostic procedures. For example, myasthenia, Graves (dysthyroid) myopathy, or orbital inflammation may all produce deficits of abduction, none of which is due to sixth nerve lesions. The “neural” etiology of lateral rectus weakness must be established or, at least, other causes excluded when possible (Table 12.1). Along with details provided by a thorough medical history, special diagnostic techniques should always be employed. Forced ductions and forced generations can be easily accomplished with local anesthesia, and are necessary to differentiate paretic from restrictive causes. When forced ductions are positive and forced generations normal, evaluation of the orbit should be performed to assess for restrictive myopathies or orbital mass lesions; when forced ductions are negative and forced generations are subnormal, a paretic process is present. In such cases, the diagnosis of myasthenia gravis should be considered and intravenous edrophonium (Tensilon) test performed if suspicion is high. The presence of a small vertical deviation (1–3 prism diopters [D]) is common, representing decompensation of normal heterophorias secondary to the acquired esotropia; however, when the vertical misalignment is larger than 5 D, concomitant involvement of other cranial nerves, or a skew deviation should be considered. Wong et al. reported that when head tilt produces an alternating hyperdeviation of the ipsilateral eye, the abducens paresis localizes to the brainstem, while nonreversing vertical deviations with head tilt result from an insult to the peripheral nerve.16
TABLE 12.1 Causes of Abduction Deficits | |
|---|---|
|
Etiology
The causes of actual sixth nerve palsy are legion (Table 12.2). As noted previously, the peripheral course of the abducens nerve is a lengthy one that predisposes this cranial nerve to involvement at all levels, from the brainstem and base of the skull, through the petrous tip and cavernous sinus, to the superior orbital fissure and orbit.
TABLE 12.2 Causes of Sixth Nerve Palsies | |
|---|---|
|
Lesions in the area of the abducens nucleus produce an ipsilateral horizontal gaze paresis because both the internuclear neurons and the motor neurons of the sixth nerve originate in this nucleus. Although it is not certain whether the horizontal gaze palsy that occurs from damage to the abducens nucleus is always symmetric, it is clear that isolated lateral rectus pareses should never be considered nuclear in origin.
The fascicular (intrapontine) portion of the abducens nerve may be involved along with adjacent structures (Fig. 12.2) to produce (a) ipsilateral paralysis of abduction (ipsilateral gaze palsy if sixth nucleus and/or pontine paramedian reticular formation [PPRF] is affected), (b) ipsilateral facial palsy, (c) ipsilateral Horner syndrome, (d) ipsilateral facial analgesia, (e) ipsilateral peripheral deafness, and (f) contralateral hemiparesis. These signs constitute the dorsolateral and ventral pontine syndromes (Foville, Millard-Gubler) at the level of the abducens fasciculus in the distribution of the anterior inferior cerebellar artery or its paramedian perforating arteries.
As the sixth nerve ascends the clivus in the subarachnoid space, it is vulnerable to various insults, including neoplasms in the prepontine basal cistern (e.g., clivus chordoma, intraforaminal extension of nasopharyngeal carcinoma), compression by downward or forward movement of the brainstem (e.g., transtentorial herniation from supratentorial space-occupying lesions, head trauma, posterior fossa masses or structural anomalies, intracranial hypotension from cerebrospinal fluid [CSF] leaks), and meningitis. It is here also that the nerve is probably affected by changes in intracranial pressure. Unilateral or bilateral abducens palsies can develop in association with pseudotumor cerebri or the syndrome of spontaneous intracranial hypotension,17 as well as after lumbar puncture, shunting for hydrocephalus, contrast myelography, spinal anesthesia,18 and treatment of cervical fractures.19
Before entering the cavernous sinus, the abducens nerve lies in relationship to the medial aspect of the petrous bone. Inflammation of the petrous bone and its dura may occur secondary to middle ear infections, with involvement of the facial nerve (facial palsy), the trigeminal ganglion (pain in the eye or face), and the abducens nerve (lateral rectus palsy). These signs and symptoms constitute the now rare Gradenigo syndrome. The combination of sixth and seventh nerve palsies, even bilateral, is not uncommon in closed head trauma, especially when the skull is compressed in its horizontal diameter (Fig. 12.6); this results in transverse fractures of the temporal bone. Leakage of blood or spinal fluid from the external ear canal, hemotympanum, or mastoid ecchymosis (Battle’s sign) may be further evidence of basal skull fracture.
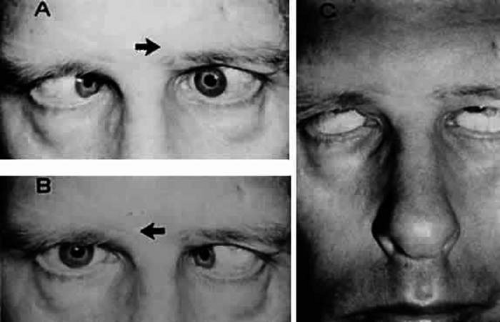 Figure 12.6 Bilateral sixth and seventh nerve palsies due to basal skull fracture. A: Left gaze. B: Right gaze. C: Attempted lid closure demonstrates intact Bell’s phenomenon and lagophthalmos. |
In the cavernous sinus, the abducens nerve may be involved in combination with the ophthalmic-trigeminal, third, or fourth nerves. Abducens monoparesis is frequent with cavernous sinus lesions, perhaps related to the nerve’s location within the sinus, inferolateral to the carotid artery and unsupported by the dural wall of the sinus.20,21 Isolated abducens palsy occurs with carotid-cavernous fistulas (especially with spontaneous dural shunts22) and intracavernous aneurysms21 (Fig. 12.7), and is the earliest indication of contralateral spread of cavernous sinus thrombosis. Sixth nerve palsy accompanied only by ipsilateral Horner syndrome also points to the cavernous sinus because the ocular sympathetics from the carotid plexus may be simultaneously involved,23 although a similar presentation may occur from brainstem disease.
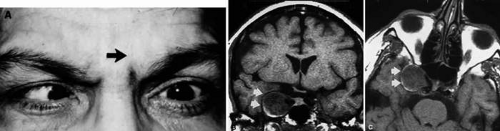 Figure 12.7 A: Chronic isolated sixth nerve palsy. Coronal (B) and axial (C) MRI sections showing large intracavernous internal carotid aneurysm (arrows). |
Lesions involving abducens nerve function at the superior orbital fissure or orbital apex regularly involve other motor nerves to the eye, or produce proptosis and/or visual compromise.
Keane24 provided an analysis of 125 cases of bilateral sixth nerve palsies. Unlike the many isolated, unilateral abducens palsies that wander in the limbo of “vascular disease,” more accurate pathoanatomic diagnoses were made where bilateral palsies existed. One-fourth of the patients in this series demonstrated deficits of other cranial nerves, and many had additional neurologic signs and symptoms, as well as spinal fluid abnormalities.
Isolated Abducens Palsy
As noted previously, all patients with abduction defects do not have sixth nerve lesions per se, and additional diagnostic techniques, such as forced ductions/generations and intravenous Tensilon tests, are mandatory. If the onset of diplopia is associated with acute eye, orbital, or head pain, then neither Graves disease nor myasthenia is a likely cause. In addition to the ocular motor (III, IV, VI) nerves, the function of cranial nerves V (especially corneal sensation), VII, and VIII should be examined.
The question now arises as to how one should proceed in the workup of the patient with a truly isolated sixth nerve palsy. In the elderly and middle-age population, vascular disease (hypertensive, diabetic, or otherwise) is a common cause of sixth nerve palsies, with remitting abducens palsies regularly encountered in the adult diabetic population. Therefore, a history of hypertension or diabetes should be sought. Given that patients may display an abducens palsy as the presenting sign of hypertension or diabetes, measurement of blood pressure and a fasting and 2-hour postprandial glucose level or glycosylated hemoglobin should be obtained. There is no correlation between severity of glucose metabolism defect and occurrence of cranial nerve palsies; thus, an isolated sixth, fourth, or pupil-sparing third nerve palsy may signal the presence of otherwise occult diabetesDiabetic retinopathy is frequently absent in these cases.
Although it would be rather extraordinary for cranial arteritis to present as isolated sixth nerve palsy, query regarding headache, jaw claudication, and scalp tenderness, as well as an erythrocyte sedimentation rate and C-reactive protein level, are reasonable in patients 65 years of age or older. Of the neurologic complications of systemic lupus erythematosus, both sixth and third nerve palsies and brainstem motility disorders are recognized.25 Because of the propensity for nasopharyngeal carcinoma to spread through the extradural space via basal skull foramina, basi-sphenoidal sections should be included in gadolinium-enhanced MRI (Table 12.3).
TABLE 12.3 Diagnostic Studies for Isolated Abduction Palsy | ||
|---|---|---|
|
When associated orbital and cranial signs and symptoms are absent, and laboratory and appropriate radiologic studies are normal, the most prudent and practical course to follow is continued observation. An examination by a neurologist is comforting, but even Tensilon testing may be postponedIn this specific clinical situation, neuroimaging is infrequently productive, and its application in the elucidation of acute or subacute isolated sixth nerve palsies is moot. However, neuroradiologic evaluation must be undertaken if pain persists or develops, if other cranial nerves become involved, or if the palsy does not begin to significantly improve over a 3- to 4-month period. Although it is true that some isolated “chronic” sixth nerve pareses last longer than 6 months, yet follow a completely benign course,26 others are indeed caused by potentially treatable basal tumors.27 Volpe and Lessell28 reported seven patients with relapsing or remitting sixth nerve palsies, which were ultimately identified to be secondary to extramedullary compression of the abducens nerve by skull-based tumors. No patients had diabetes or vascular disease, and all recovered completely at least once (and, in one case, in five separate episodes) without surgical intervention, radiotherapy, or chemotherapy before a definitive diagnosis was made. Lesions included chordomas (Fig. 12.8), chondrosarcomas, and presumed meningiomas. In other cases of isolated abducens pareses that do not recover, imaging may disclose compression from a dolichoectatic vertebral artery29,30 or a schwannoma of the nerve.31
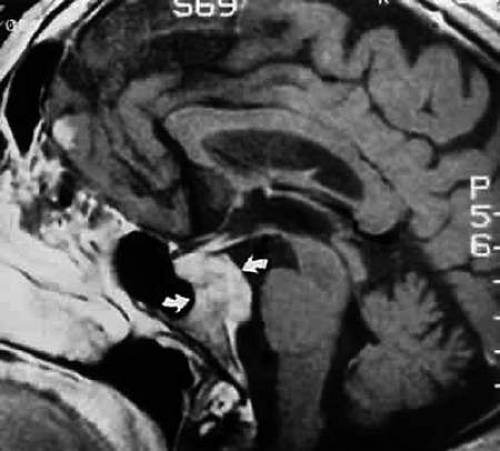 Figure 12.8 MRI sagittal section, gadolinium enhanced, shows clivus chordoma (arrows). Patient presented with chronic bilateral sixth nerve palsies. |
When pain persists and all radiologic and orbital investigations are unrevealing, a trial of corticosteroids (e.g., 60 mg prednisone orally for 5 days) may result in prompt and dramatic relief, in which case a tentative diagnosis of nonspecific inflammation of the superior orbital fissure or cavernous sinus may be made. However, the “response to steroid trial” may produce relief of pain with neoplasms as well as inflammation (see Combined Ocular Motor Palsies and Painful Ophthalmoplegia section). Certainly, unrelenting eye or orbital or facial pain is an indication for exquisite visualization of the cavernous sinus and parasellar area by thin-section MRI scanning and either magnetic resonance or conventional angiography, if vascular abnormalities are suspected.
Isolated sixth nerve palsies in children often resolve spontaneously. Newborns may rarely manifest a transient lateral rectus weakness, with resolution occurring by 6 weeks.32 Knox et al.33 called attention to transient isolated abducens palsy of presumed postviral origin developing in children 1 to 3 weeks after nonspecific febrile or respiratory illness. The age range of the patients reviewed was 18 months to the early teens; recovery of abducens function occurred within 10 weeks (one case continued for 9 months). A similar pattern may be seen with specific viral illnesses such as varicella,34 after immunization,35 or in association with Epstein-Barr viremia.36 A spate of reports indicates that some patients have multiple recurrences of these isolated “benign” sixth nerve palsies and that these recurrences have no serious implications.35,37,38,39,39A Similar cases of isolated “benign” abducens pareses in children that resolved spontaneously have been reported in association with high levels of anti-GQ1b IgG antibodies.40 A 35-year-old patient with cluster headaches also experienced three consecutive right lateral rectus palsies, on each occasion beginning a day or two after onset of pain, with recovery within 2 weeks41; radiologic studies were unremarkable, suggesting the possibility of migrainous abducens palsy.
Robertson et al.42 found a high incidence of brain tumor in his Mayo Clinic series of children with sixth nerve paresis. Although referred to as cases of “isolated” sixth nerve paresis, this definition signifies only that no other ocular motor nerves were defective. Indeed, of the children with neoplasms, one-third had papilledema and one-half demonstrated nystagmus at the time of initial examination. Of the patients with tumor who truly presented with only isolated abducens palsy, additional signs appeared within a few weeks or, rarely, within 2 to 3 months. Harley,43 in his series of children with sixth nerve palsies of all causes, whether isolated or not, noted that approximately one-third had suffered trauma and one-fourth had underlying tumors; the total clinical picture in these cases is not described.
In the child with an isolated sixth nerve palsy without other neurologic signs, including papilledema, headaches, or ataxia, the following approach is suggested: (a) rule out middle ear infection; and (b) obtain a peripheral blood count (lymphocytosis may be considered an indication of recent viral infection). The child must be re-examined at regular intervals until the paresis clears, and the parents must be advised to observe for new signs or symptoms. If the paresis persists or worsens, MRI is mandated. A persistent sixth nerve paresis in childhood may be the first clinical sign of a pontine astrocytoma or other posterior fossa mass lesion.
In a 10-year series of 49 “younger adults” (age range, 15–50 years) with isolated sixth nerve palsy, Moster et al.44 reported that about one-third had diabetes and/or hypertension; 8 had basal tumors; 6 had isolated abducens palsies as the initial sign of multiple sclerosis (all with subsequent clinical or spinal fluid abnormalities), usually with spontaneous resolution; and 11 had no specific etiology disclosed, but did have a sanguine outcome. This series excluded patients with a positive Tensilon test, abnormal forced ductions, other known neurologic disease, or bilateral palsies.
Larger series of sixth nerve palsies reported45,46,47 are helpful in reviewing the causes, although these patients were somewhat preselected. The largest number of cases fell into the nonspecific “vascular” category (37%, 7%, and 18%, respectively) and the “undetermined” category (24%, 21%, and 29%, respectively). All three series included a modest number of patients with multiple sclerosis (13%, 7%, and 4%, respectively; also 12% in the Moster44 series), but isolated abducens palsy in demyelinative disease has been exceedingly rare in our personal experience. Although MRI, not uncommonly reveals abnormal signals in the pons, clinical evaluation of ocular motility is often quite unremarkable.48
Minimal abduction paresis may herald increased intracranial pressure, such that the patient complains of horizontal diplopia when viewing distant objects. Clinically, these symptoms and findings may mimic divergence insufficiency. Kirkham et al.,49 using electro-oculographic techniques, demonstrated reduced abduction saccadic velocities, which suggest bilateral minimal sixth nerve dysfunction. Although neurons that discharge with divergence (and convergence) have been found in the mesencephalic reticular formation of the monkey,50 the existence of a “divergence center” in the human brainstem still remains controversial.
Trauma remains an important cause of sixth nerve palsy in all age groups. It is likely that the relationship between the nerve and the skull base and vessels renders it vulnerable rather than the length of the nerve itself (e.g., the trochlear nerve is nearly three times longer than the abducens51), yet both are commonly injured in closed heard injuries. Spontaneous full recovery occurs in a only minority (approximately 25%) of cases.52 Although it was in such cases that botulinum toxin injection to the ipsilateral medial rectus provided great hope of maximizing recovery and decreasing the need for surgery, unfortunately long-term results show little evidence for its efficacy in these regards.53
Symptomatic treatment of an acute sixth nerve palsy includes the use of Fresnel prisms, or alternate patching to avoid diplopia and possible medial rectus contracture. The injection of botulinum toxin type A (Botox) into the ipsilateral medial rectus is quite effective at preventing muscle contracture and improving fusion in the primary position of gaze. However, this procedure carries the disadvantage of significant crossed diplopia (exotropia) in contralateral gaze. Definitive surgical correction of a sixth nerve paresis should be employed when the deviation has been stable for at least 6 months. The primary consideration in these cases is the amount of residual abducting power of the lateral rectus because moderate to good abduction is associated with successful ipsilateral recess/resect procedures (perhaps combined with contralateral medial rectus recession). However, if residual abduction is poor or absent, ipsilateral medial rectus recession may be combined with either a full- or partial-thickness tendon transplant procedure of the superior and inferior recti, or a Jensen procedure. More recently, Foster described full-thickness transpositions with retroequitorial myopexy, which often corrects the esotropia without the need for medical rectus recession, decreasing the risk of anterior segment ischemia in susceptible patients.
Divergence paralysis is characterized by acute comitant esotropia at distance, normal fusion at near, and full ocular ductions. Of 11 patients with nontraumatic cause, Krohel et al.54 found 3 with neurologic disease and other findings. Otherwise, there was no tendency to late evolution of neurologic sequelae. Stern and Tomsak55 reported a young adult with a lower pontine lesion and also provided a useful overview of “divergence paralysis.” Divergence paralysis has been reported in association with Chiari I malformation; in some cases, fusion returns to normal after neurosurgical correction.56 In general, however, in the over-50 population, the process is idiopathic and benign, and neuroimaging is neither useful nor necessary. When surgical correction is indicated in these cases, standard horizontal muscle surgery effectively eliminates diplopia.
Trochlear Palsies
Palsy of the superior oblique, as in the case of isolated lateral rectus weakness, may be due to local orbital processes that should be distinguished from a neurogenic lesion per se. As always, myasthenia and Graves myopathy (an especially frequent cause of incomitant vertical strabismus) must be suspected and appropriate tests performed. The pattern of muscle imbalance and ocular versions can be quite similar in ipsilateral inferior rectus fibrosis (e.g., in Graves disease) and contralateral superior oblique paresis57; however, worsening of the vertical deviation in upgaze is seen in inferior rectus fibrosis, and in downgaze in superior oblique palsy. Also, intraocular pressure may increase in attempted upgaze in restrictive (Graves) disease. Excyclodeviations are more prominent in superior oblique paresis than in thyroid myopathy, which may show significant excyclotorsion only in abduction.
Superior oblique palsies may present spontaneously in late childhood and possibly represent “decompensated” congenital fourth nerve palsies. This diagnostic concept (i.e., that fusional mechanisms decompensate in later life) has also been applied to otherwise healthy adults with spontaneously acquired, unremitting superior oblique palsies of unknown origin (Fig. 12.9). A similar, often transient, occurrence of superior oblique palsy has been reported during pregnancy.58 These adults complain of reading difficulties, intermittent diplopia, and show all attributes of superior oblique palsy. Old photographs may document tilting of the head, and further inquiry may uncover a forgotten history of childhood squint. Patients with congenital trochlear palsies commonly show increased amplitudes of vertical vergence.59 Normally, only 2 to 4 prism diopters (D of vertical fusional amplitude are found, but patients with congenital superior oblique pareses may be able to fuse a 10-D or even a 30-D deviation. However, the presence of large vertical fusional amplitudes does not necessarily imply a congenital etiology because vertical fusional vergence may increase in adults within weeks or months after an acquired vertical strabismus.
 Figure 12.9 An 18-year-old with head tilt complained of intermittent diplopia for several months. Muscle balance measured 8Δ of right hypertropia in primary position and 16Δ in left gaze. Snapshots at ages 12 and 2 years demonstrate habitual head tilt consistent with right superior oblique palsy. |
The cause of most congenital superior oblique palsies is unknown; however, agenesis of the trochlear nucleus has been described in association with agenesis of other cranial nerve nuclei,60 but never in the situation of isolated congenital fourth nerve palsy. Dysplasia (aplasia) of cranial nuclei may occur after perinatal peripheral injuries to nerves, with secondary “dying back.” Also, axonal death, with selective elimination and preservation, is an established phenomenon during neurogenesis of all cranial nerves.61 Absence of the superior oblique tendon has been observed during surgery to correct putative isolated congenital superior oblique palsies. This phenomenon may be more common in patients with craniofacial dysostoses.62 Indeed, Helveston et al.63 reported congenital absence of the superior oblique tendon in 18% of patients with congenital superior oblique palsy, in whom a tuck of the superior oblique had been contemplated, and in another subgroup of patients with congenital superior oblique pareses, abnormally lax superior oblique tendons have been described. Bilateral congenital superior oblique palsies (particularly asymmetric pareses), as with bilateral acquired superior oblique palsies, may initially appear to be unilateral until corrective surgery “unmasks” the contralateral palsy.
Other than in the context of trauma, acquired isolated fourth nerve palsy occurs far less frequently than abducens or oculomotor palsies. In a retrospective study of 412 patients,57 third and sixth nerve palsies were seven times more common than fourth nerve palsy. As with isolated abducens palsy, many spontaneous trochlear palsies are classified as “unknown” or “vascular.” In the older age group, isolated fourth nerve palsy may infrequently be associated with diabetes. Keane65 provided an excellent overview of fourth nerve palsy among 215 patients, with head trauma representing the cause in more than 50%; no tumors showed isolated palsies, but were accompanied by other defects related to lesions in the cavernous sinus. In comparison, out of 149 patients with ocular myasthenia, none had isolated superior oblique weakness. Bilateral fourth palsies occurred in 19%; again, the majority of these cases were due to head trauma. Herpes zoster ophthalmicus may be associated with isolated trochlear palsy,66 with variable recovery, but meningitis produces other signs and symptoms.65 Although extremely rare, intracranial aneurysms (e.g., superior cerebellar artery) have been documented to cause superior oblique palsy as well.67 Autosomal-dominant inheritance of superior oblique palsy, some bilateral, is also documented.68 Even rarer, but well-documented, causes of isolated superior oblique palsy include perineural spread of squamous cell carcinoma,69 posteriorly draining dural-sinus fistula,70 spread of pituitary adenoma,71 schwannoma of the nerve,72 and midbrain hemorrhage.73 The causes of fourth nerve palsies are listed in Table 12.4.
TABLE 12.4 Causes of Superior Oblique Paresis | ||
|---|---|---|
|
Although uncommon, alterations in intracranial pressure may produce superior oblique paresis. Trochlear palsy has been reported in three children with pseudotumor cerebri (idiopathic intracranial hypertension [IIH]).74 Certainly in this setting one would expect to also find papilledema and abducens weakness. Although the authors have also seen superior oblique paresis in the setting of pseudotumor cerebri, the presence of such mandates intense investigation for other causes before assigning IIH as the culprit. Conversely, trochlear paresis (along with pupil-sparing oculomotor palsy) has been reported in spontaneous intracranial hypotension.75 Again, this must be exceedingly rare, and diagnosis can be made only after other potential causes have been excluded.
Susceptibility of the trochlear nerve to injury in closed head traumas has been attributed to the position of the nerves with respect to the tentorial edge. According to Lindenberg,76 the tectum of the midbrain is subject to contrecoup contusion at the tentorial notch when the forehead or skull vertex strikes a stationary object, with the impact force directed toward the tentorium. The fourth nerves may be injured as they sweep laterally around the midbrain or dorsally in the anterior medullary velum, or in the substance of the lower midbrain. In these situations, bilateral fourth nerve palsies are common. Lindenberg also pointed out that, in blows to the base of the occiput or even in falls on the buttocks, forces are transmitted such that the cerebellum is thrust against the tentorium from below. In contrast to Lindenberg’s neuropathologic material, fourth nerve palsies may result from minimal, if not insignificant, occipital trauma; these cases tend to resolve spontaneously.77 Radiographic documentation of the site of damage to the fourth nerve is unusual after trauma, but MRI of the posterior fossa has greatly increased the possibility of identifying minor intra- and extra-axial lesions in these cases.
As a rule, the diagnosis of an acute superior oblique palsy is not difficult (Fig. 12.10). Many patients rapidly learn to tilt the head toward the side opposite the defective eye. Such head tilting is not an exclusive sign of trochlear palsy, but it is seen more consistently here than with other vertical muscle pareses.78 Nevertheless, it must be cautioned that a number of patients will have no consistent head tilt, or may even show a tilt toward the palsied side, possibly to achieve greater subjective image separation so that the more peripheral image can be ignored.
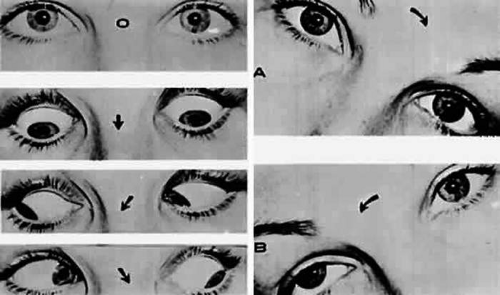 Figure 12.10 Ocular deviation with right superior oblique palsy. Left: Defective duction of right eye on gaze down and left. Right: Bielschowsky head-tilt test: (A) Tilt to left; (B) tilt to right (note increased right hyperdeviation). |
According to the data accumulated by Khawam et al.,78 all patients with unilateral superior oblique palsies show vertical deviation in the primary position, with an increase in deviation on adduction of the involved eye. A common pattern wherein the vertical deviation is greatest in adduction and elevation is seen with secondary inferior oblique overaction. With time, the vertical deviation often becomes comitant. In patients with bilateral palsies, almost all due to head trauma, the vertical deviation in primary position tends to be smaller. Anomalous head positions were present in half of the unilateral palsies and 70% of the bilateral palsies, but more than 90% of all patients demonstrated greater vertical deviation with the head tilted toward the side of the paretic muscle (i.e., a positive Bielschowsky forced head-tilt test; Fig. 12.10). Sydnor et al.79 concurred that unilateral fourth nerve palsies have large hypertropias and more vertical than torsional diplopia, whereas bilateral palsies show small hypertropias in primary gaze, large V-pattern esotropias, a compensating chin-down position that permits fusion in upgaze, and excyclotorsion >10 to 12 degrees. Lee and Flynn80 noted that bilateral superior oblique palsies should be suspected when the Bielschowsky test is positive with head tilt in both directions, especially after a relatively severe head trauma.
In the clinical dilemma of acquired vertical deviations, Trobe81 provided practical data regarding cyclotorsional defects: excyclodeviation occurred in 30 of 33 patients with trochlear palsies, 8 of 15 patients with Graves ophthalmopathy, and 1 of 13 patients with myasthenia, but did not occur in any case of skew deviation. Keane82 provided an excellent summary of the vertical diplopia syndromes seen during a 15-year inpatient hospital experience, including oculomotor palsy (579 cases), trochlear palsy (133 cases), skew deviation (434 cases), myasthenia (94 cases), and others, such as Guillain-Barré syndrome, orbital floor fracture, and Graves ophthalmopathy.
In the patient with an isolated superior oblique palsy, without antecedent trauma and with a negative Tensilon test, forced duction, and serum glucose tests, observation is the rule. Radiologic studies are of minimal value. The importance of old photograph review cannot be overemphasized, with demonstration of ocular torticollis indicative of a long-standing, if not congenital, lesion. Most patients with presumed microvascular disease spontaneously recover in less than 6 months (3–4 months being the rule).47 If such recovery does not occur, or if the patient has a decompensated congenital lesion, further treatment is necessary. If the deviation is stable, prisms can be incorporated into spectacles, but this may fail because of torsional defects or persistent incomitance. After measurements remain stable for at least 6 months, surgical correction may be undertaken with a high rate of success. In general, ductional defects should be addressed: For example, if the superior oblique is underactive, a tendon-tucking procedure is preferred; with significant inferior oblique overaction, inferior oblique myectomy or recession is quite effective. Depending on the degree and pattern of the vertical misalignment, recessions of the ipsilateral superior rectus and/or contralateral inferior rectus using the adjustable suture technique may be employed. These procedures have worked well in cases of congenital absence of the superior oblique tendon83 or bilateral superior oblique palsies. For bilateral cases, surgery should be commensurate with the relative degree of symmetry between the two eyes. In cases of persistent V-pattern esotropia and excyclodeviation, after bilateral superior oblique tucks, bilateral inferior rectus recessions often yield significant improvement.84 Finally, in cases where there is minimal vertical deviation but excyclodiplopia is the chief complaint, advancement of the anterior superior oblique tendon fibers (Harada-Ito procedure) may improve the torsional diplopia without disturbing vertical ocular alignment.
Acting as a pseudopalsy of the inferior oblique, Brown syndrome refers to an anomalous articulation between the trochlea and superior oblique tendon sheath, resulting in a restrictive strabismus showing lack of elevation in adduction. This is most often a congenital disorder, in which diplopia is infrequent and good fusion is the rule. Many patients enjoy spontaneous improvement by late childhood or early adulthood.85 When surgery is required for large hypotropia in the primary position, or for disfiguring chin-up posture in order to promote fusion, superior oblique tenectomy with or without ipsilateral inferior oblique weakening is the most commonly employed procedure. Other surgical techniques include introduction of a silicone tendon expander and superior oblique and trochlear luxation.86 A form of secondary Brown syndrome may also be acquired after orbital trauma87 or with orbital metastasis.88 It has been described in association with systemic collagen vascular disease, such as juvenile rheumatoid arthritis,89 systemic lupus erythematosus,90 and hypogammaglobulinemia. Such cases typically respond well to oral steroids or nonsteroidal agents. Local injection of depot steroids in the region of the trochlea can produce improvement as well, but may cause secondary scarring and fibrosis. Brown syndrome has also been described as a transient phenomenon in the postpartum period91 and may be an unusual presentation of extraocular muscle cysticercosis.92
Superior oblique myokymia (see also Chapter 11) consists of spasms of cyclotorsional and vertical eye movements. These are often difficult to appreciate on gross examination, but are easily seen with the slit lamp or ophthalmoscope. There is an initial intorsion and depression of the affected eye, followed by irregular torsional oscillations of minor amplitude. This phenomenon is strictly unilateral, and generally occurs in the absence of neurologic disease. However, neurovascular compression of the trochlear nerve by a branch of the superior cerebellar artery has been documented in some cases.93,94,95. Brazis et al.96 reported a long-term follow-up of 16 patients. Classic therapeutic options include carbamazepine or propranolol, although gabapentin has recently touted as highly successful.97,98 If medical treatment is ineffective or intolerable, superior oblique tenectomy combined with inferior oblique myectomy to avoid iatrogenic trochlear paresis has been documented to be an effective treatment. Kosmorsky also advocated weakening of the anterior superior oblique tendon via the Harad-Ito procedure.99 In cases of superior oblique myokymia due to neural microvascular compression, craniotomy and neurosurgical decompression have shown efficacy in some cases.100,101
Oculomotor Palsies
Oculomotor nerve function may be affected at a nuclear level, in the fascicular portion within the midbrain, in the interpeduncular space, in its course forward alongside the posterior communicating artery, at its entrance into the dura lateral and anterior to the dorsum sellae, in the cavernous sinus, in the superior orbital fissure, and in the orbit itself. The combination of oculomotor palsy with other cranial nerve (II, IV, V, VI) deficits, or with corticospinal or cerebellar-system signs, permits accurate localizing diagnoses (Table 12.5).
TABLE 12.5 Causes of Oculomotor Palsies | |
|---|---|
|
Nuclear Lesions
Disorders of the oculomotor nerve at its nuclear source may be encountered in rare instances. Based on Warwick’s anatomic configuration of the third nerve nuclear complex (Fig. 12.3), the following clinical rules are applicable:
Conditions that cannot represent nuclear lesions
Unilateral external ophthalmoplegia (with or without pupil involvement) associated with normal contralateral superior rectus function
Unilateral internal ophthalmoplegia
Unilateral ptosis
Conditions that may be nuclear
Bilateral total third nerve palsy
Bilateral ptosis
Bilateral internal ophthalmoplegia
Bilateral medial rectus palsy
Isolated single muscle involvement (except levator and superior rectus)
Obligatory nuclear lesions
Unilateral third nerve palsy with contralateral superior rectus paresis and bilateral partial ptosis
Bilateral third nerve palsy (with or without internal ophthalmoplegia) associated with spared levator function
Because ocular myasthenia and, in some instances, Graves myopathy may mimic various patterns of oculomotor nerve dysfunction, Tensilon testing and forced ductions should be considered in cases of painless ophthalmoplegia where pupils are normal. Supranuclear lesions involving midbrain structures near the third nerve nucleus may closely simulate direct damage to the nucleus. If ocular motility improves with vestibular stimulation (oculocephalic reflex, calorics) or with Bell’s phenomenon, a supranuclear lesion is present. Failure of ocular motility to improve with any of these stimuli indicates the presence of a nuclear or infranuclear lesion, but does not exclude additionalsupranuclear abnormalities.
Several clinicopathological studies have supported Warwick’s schema. There are documented instances of isolated bilateral ptosis, with discrete foci in the nuclear complex of the third nerve, in the midline at the level of the central caudal nucleus.102 Keane et al.103 described a case of unilateral oculomotor palsy, complete except for near-normal levator function; at autopsy, a solitary midbrain metastasis was seen involving the rostral ipsilateral third nerve nucleus, but sparing the central caudal levator nucleus. The MRI findings in two instances of levator-sparing nuclear oculomotor palsies, with contralateral elevator palsy, defined focal rostral midbrain infarcts.104 In several patients, isolated extraocular muscle palsies (e.g., isolated inferior rectus palsy) have been ascribed on clinical grounds to small lesions of the oculomotor nuclear complex.105
Acquired binuclear total ophthalmoplegia is occasionally seen (Fig. 12.11), as reported by Masucci.106 These findings are the result of thrombotic or embolic processes at the level of the basilar bifurcation, with occlusion of the median mesencephalic perforating arteries. Congenital bilateral total ophthalmoplegia with or without levator and pupil sparing has been reported and may be associated with dysplasia of the corpus callosum.107
 Figure 12.11 Bilateral oculomotor palsies (nuclear?) associated with abrupt onset of vertigo and mild left hemiparesis. |
Fascicular Lesions
Deficits of the oculomotor fasciculus are usually identified by the accompanying brainstem signs. Oculomotor palsy with contralateral hemiplegia (Weber syndrome) indicates involvement of the corticospinal tracts. Contralateral ataxia and intention tremor (Benedikt syndrome) indicates involvement of the red nucleus (Fig. 12.2). Nothnagel syndrome is an eponym given when signs of both Weber and Benedikt syndromes are present. Midbrain vascular accidents account for most fascicular defects.
Ksiazek108 shed some light on the fascicular arrangement of the oculomotor nerve based on two patients with partial oculomotor paresis, each with pupillary mydriasis, significant inferior rectus paresis, and medial rectus paresis. Neuroimaging revealed a lesion in the fascicular portion of the nerve, thus indicating the proximity of these fibers in the fasciculus. Monocular elevator paresis (superior rectus and inferior oblique) in mass compression of the oculomotor fasciculus has also been reported.109 In this regard, Castro et al.110 proposed the mediolateral somatotopy of the oculomotor fascicular fibers within the mesencephalon with the inferior oblique and superior rectus muscles being most lateral, and the pupilloconstrictor fibers and inferior rectus being most medial. The levator palpebrae fascicles are in an intermediate location between the superior rectus and medial rectus fascicles.
Interpeduncular Lesions
Basal lesions, including the rare rostral basilar artery aneurysm, may encroach on the oculomotor nerves as they exit in the interpeduncular space. Such slow-growing aneurysms, either saccular or fusiform, may present as partial oculomotor palsies with or without involvement of pyramidal tracts, and without subarachnoid hemorrhage.111 Aneurysms of the posterior communicating artery, in contrast, are probably the most common lesions causing acute spontaneous oculomotor palsies (Fig. 12.12). The oculomotor palsy thatoccurs from posterior communicating aneurysm is not necessarilydue to mass effect per se, but rather is attributed tohemorrhage that suddenly enlarges the aneurysmal sac to which the oculomotor nerve is adherent, or to hemorrhage into the substance of the nerve itself. Most patients present, therefore, with an intensely painful, complete unilateral oculomotor palsy in association with other signs and symptoms of subarachnoid hemorrhage. ew patients with symptomatic posterior communicating aneurysms are found in office waiting rooms; instead, they are usually obtunded or comatose in emergency rooms.
 Figure 12.12 Sudden total right ophthalmoplegia accompanied by orbital pain, due to posterior communicating artery aneurysm. A: Complete right ptosis. B: Right eye in abducted position, with dilated pupil, fixed to light. C: Failure of adduction on left gaze. D: Right eye intorts (arrow) on downward gaze, indicating retained function of fourth nerve. E: Contrast-enhanced T1-weighted MRI axial section shows aneurysm (arrows). Confirmed by angiography. |
Involvement of pupillary fibers is such a consistent finding in third nerve palsies due to bleeding aneurysms that most clinicians concur in this useful dictum: A pupil-sparing, but otherwise complete, third nerve palsy is unlikely to be due to posterior communicating aneurysms. Careful pupil evaluation may disclose subtle abnormalities in “apparent pupil sparing,” especially in cases of aberrant regeneration or with chronic cavernous sinus lesions. Generally, in patients at least 50 years of age or older, an acute, isolated, painful oculomotor palsy that spares the pupil is caused by intraneural ischemia; nevertheless, these patients must be carefully observed for further evolution. In our opinion, an acute complete oculomotor palsy with moderate to major mydriasis, even when diabetes is present, is an indication for cerebral arteriography. It should be emphasized that magnetic resonance angiography may not detect aneurysms smaller than 3 to 4 mm.113 CT angiography is a newer modality that may prove equivalent in diagnostic efficacy to conventional angiography, but at the time of this writing, the latter still remains the gold standard.114,115,116 Before ordering such tests, the clinician should be familiar with the preferences and experience of local radiologists and neurosurgeons.
The clinical management of patients with relative pupil-sparing third nerve palsies remains in debate. Observation alone arguably is appropriate management of such patients and is certainly reasonable in completely pupil-sparing lesions (e.g., there is complete ophthalmoplegia and ptosis, but the pupils are identical in size and reactivity). Many clinicians will similarly choose to observe a patient with up to 2 mm of anisocoria and complete external ophthalmoplegia; however, management becomes more difficult in cases of partial paresis. Because almost every conceivable combination of partial ophthalmoplegia and pupillary abnormality has been reported in aneurysmal compression of the third nerve, it is better to err on the side of caution and perform angiography. It is incumbent on the physician to evaluate carefully the proportion of ophthalmoplegia and ptosis in relation to the degree of pupillary abnormality when deciding appropriate workup of these patients. Similarly, Capó et al.117 pointed out that the interval from onset to maximal ophthalmoplegia does not differentiate between microvascular (3.3 days) and aneurysm (3 days). Sanders et al.118 reported that pupil-sparing oculomotor pareses due to aneurysms tend to have a more focal (divisional) pattern of muscle weakness, whereas those due to ischemic disease have a more diffuse pattern of paresis. Nevertheless, such rules are in part arbitrary and subjective, and we continue to urge clinicians to err on the side of caution, as noted previously. Even a temporal profile resulting in spontaneous recovery cannot exclude aneurysm, as at least one well-documented case attests.119
Other partial oculomotor palsies occur regularly with cavernous sinus masses and parasellar syndromes, accompanied by variable pupillary findings. Furthermore, both acute and chronic lesions may produce incomplete palsy of the superior division (supplying levator palpebrae and superior rectus muscles) or of the inferior division (medial and inferior recti, inferior oblique, ciliary muscle, and pupillomotor fibers). If pain or first trigeminal division numbness are absent, and if the pupil is uninvolved, such fractional oculomotor pareses are regularly misinterpreted as myasthenia or local orbital inflammations. Guy et al.120 described five patients with isolated ptosis and elevator paresis in abduction, consistent with selective “superior division” involvement. They also discussed five previously reported cases with the following respective diagnoses: (a) intracavernous aneurysm (usually with associated Horner syndrome) and basilar artery aneurysm, (b) diabetic ophthalmoplegia, (c) meningitis, (d) dural lymphoma, and (e) postsurgical manipulation of parasellar structures. In essence, there was little anatomic correlation with the physical separation into superior and inferior oculomotor trunks that occurs in the cavernous sinus. Moreover, two patients sustained superior division palsies during surgical manipulation of the subarachnoidal portion of the oculomotor nerve trunk. A number of cases of inferior rectus paresis, isolated or in combination with ipsilateral or contralateral superior rectus paresis, have been construed as focal lesions involving the rostral portion of the oculomotor nuclear complex.104,105,106
Oculomotor palsy following head trauma is not rare, but occurs less frequently than traumatic fourth nerve palsies. As a rule, such closed head injury causes loss of consciousness and is accompanied by skull fracture, but this is not invariable.121 Injury to the ocular motor nerves in road accidents was studied by Heinze,122 who dissected the cadavers of 21 fatal cases. He found that the relationship of frontal or temporal fractures to neural damage was unpredictable. In fact, intact nerves were encountered adjacent to gross fracture sites. The oculomotor nerve was damaged at three locations: (a) avulsion of the rootlets at their ventral exit from the brainstem, (b) contusion necrosis of the most proximal portion of the nerve trunk, and (c) intraneural and perineural hemorrhage of the nerve trunks at the level of the superior orbital fissure.Of great interest are Heinze’s findings of focal hemorrhages in extraocular muscles, usually associated with fractured orbital bones
Eyster et al.123 reported three patients with large basicranial tumors, who presented with oculomotor palsies precipitated by mild blows to the head that were insufficient to cause fracture or loss of consciousness. The oculomotor nerves were encased and stretched by tumor, which apparently rendered these tethered nerves vulnerable when innocent head blows abruptly shifted the brain. The authors pointed out that such atypical presentations of intracranial tumors may further mimic aneurysms because subarachnoid hemorrhage does occasionally occur with tumors. Neetens124 reported an additional three cases of oculomotor nerve palsies after minor trauma in the presence of basal intracranial tumors; the trochlear nerve was involved in all three cases, and in two cases, the oculomotor nerve was partially affected. Walter et al.125 reported two instances of minor head trauma resulting in complete third nerve palsies attributed to occult posterior communicating artery aneurysms. We have seen a 45-year-old school teacher who experienced an immediate right abducens palsy when playfully slapped on the back of the head; within weeks, other cranial nerve palsies announced the presence of diffuse meningeal spread of carcinoma.
In the United States, basilar meningitis is rare, but was formerly encountered with tuberculosis and syphilis. When the third nerve is involved in such cases, progressive defects are the rule and other cranial nerve palsies are commonly found. Oculomotor palsy may especially occur with meningitides in infants, including instances of viral and bacterial (e.g., Streptococcus pneumoniae, Haemophilus influenzae) infections.126
Oculomotor nerve compression by the proximal segment of the posterior cerebral artery, or by the uncus against the petroclinoid ligament, can be seen with increasing cerebral edema or with an ipsilateral expanding supratentorial mass, and it is often heralded by unilateral pupillary dilation (Hutchinson pupil). Progression rapidly leads to complete ocular motor nerve palsy. Keane127 reviewed the ocular motor signs of tentorial herniation, which include anisocoria and parasympathetic pupillary abnormalities, unilateral or bilateral ptosis, internuclear ophthalmoplegia, vertical gaze paresis, and partial third nerve palsies.
Cavernous Sinus Lesions
The oculomotor nerve may be involved by inflammatory disease, tumor, aneurysm, arteriovenous fistula, or thrombosis at the level of the cavernous sinus. The third nerve is usually involved in combination with the fourth, sixth, and ophthalmic-trigeminal nerves, and accompanying sympathetic paresis may minimize pupillary dilation. The syndrome of the cavernous sinus, therefore, includes multiple ocular motor nerve palsies and pain or numbness in the first trigeminal division. In practice, lesions involving primarily the superior orbital fissure produce signs and symptoms that, with the possible exception of proptosis, cannot be distinguished from those of the anterior cavernous sinus. In particular, dural carotid cavernous fistulas that drain primarily into the inferior petrosal sinus may cause third nerve pareses without significant orbital congestion.128
Third nerve palsies due to lesions in the cavernous sinus tend to be partial in that all muscles innervated by the oculomotor branches need not be involved. This is especially true of pupillomotor fibers, such that the pupil may be normal or minimally involved. This “pupil sparing” is offhandedly attributed to the superimposition of sympathetic paresis (Horner syndrome), but appropriate pharmacologic tests rarely substantiate this explanation (see Parasellar Syndrome section). More likely, slowly expanding masses (e.g., infraclinoid aneurysm, meningioma) functionally spare the pupilloconstrictor fibers in the intracavernous portion of the oculomotor nerve. In addition, the levator, superior, inferior, and medial recti may be involved in unequal degrees, but progressive paresis evolves. (Once again, myasthenia must be suspected in any nonpainful, pupil-sparing, nonproptotic ophthalmoplegia, with or without ptosis.) Cavernous sinus lesions are further discussed later in this chapter.
Primary neurinoma of the oculomotor nerve is a relatively rare lesion that should be considered in children or young adults with insidious third nerve palsy. These may occur in the cavernous or interpeduncular portion of the nerve (Fig. 12.13).129,129A,130 Slow progression and late appearance of aberrant regeneration are typical; diagnosis is often missed until serial neuroimaging is performed.130
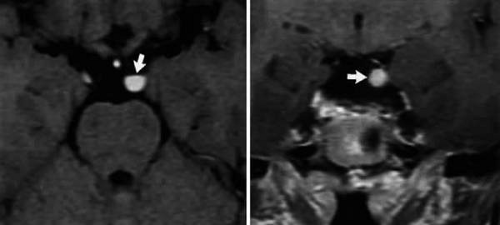 Figure 12.13 Insidiously progressive third nerve palsy due to oculomotor neurinoma (arrows) in 16-year-old girl. MRI T-1, enhanced axial (top) and coronal (bottom) sections. |
Orbital Lesions
Oculomotor nerve palsies with orbital lesions are usually accompanied by abducens weakness and proptosis. In the absence of proptosis, anterior cavernous sinus lesions may not be distinguishable from those involving the superior orbital fissure or orbital apex. Nonspecific inflammations of orbital tissues (orbital pseudotumor) may produce palsies of extraocular muscles in variable combinations, but other manifestations (e.g., pain, chemosis, ocular inflammation, proptosis) are usually present. Orbital trauma, unless overlooked or forgotten, usually presents no difficulty in diagnosis. Forced duction testing and orbital ultrasonography and/or enhanced CT imaging are indicated.
Management of Strabismus Secondary to Cranial Nerve Palsies
After a definitive diagnosis is established and the etiology of the cranial nerve palsy is determined, the next challenge is the management of the resultant strabismus. The goals of treatment are improvement of the ocular alignment and relief of the binocular diplopia. Depending on the etiology of the nerve palsy, the strabismus may improve spontaneously during the first few weeks. Nevertheless, while waiting for recovery of function of the affected muscles, various temporizing methods exist to alleviate the double vision and prevent contracture of the antagonist muscles, including patching, prisms, and botulinum toxin injections.
Temporizing Methods
Wearing a patch is especially helpful in avoiding diplopia during the immediate onset of the palsy, when incomitance of the ocular deviation is greatest. The patch can be worn over either eye, depending on the ocular dominance and the visual acuity of each eye. Wearing the patch over the sound eye may help prevent contracture of the antagonist muscle; however, disadvantages of fixating with the affected eye are the limited range of movement and past-pointing. Although prisms can be used during the acute stage, they provide only a small field of single binocular vision due to the incomitance typical of paralytic strabismus of recent onset. Prisms are most helpful once there is spread of comitance or for small residual deviations after partial recovery. Fresnel stick-on prisms are ideal for large or rapidly evolving strabismus, but for small stable deviations ground-in prisms are preferable. Fresnel prisms may be placed at oblique angles over the paretic eye in cases of combined horizontal and vertical strabismus, avoiding a second prism in the nonaffected eye.
Repeated measurements of the strabismus in various positions of gaze are of paramount importance to document the evolution of the disease. If the affected muscles demonstrate no recovery of function 6 to 8 weeks after the onset of the palsy, contracture of the antagonist muscles may ensue. To prevent contracture of the antagonist muscles, botulinum toxin injections may be used. Botulinum toxin produces temporary chemodenervation of the muscle by blocking the release of acetylcholine at the neuromuscular junction. The effect is dose related. For extraocular muscle injections, the dose recommended is 2.5 to 10 units, depending on the angle of the deviation and the level of function of the affected muscle. Botox injections are particularly helpful in sixth and third cranial nerve palsies when large-angle esotropia or exotropia is the main problem.131,132 Following botulinum toxin treatment, the diplopia may improve in primary position; however, the field of single binocular vision is very narrow due to paralysis of both agonist and antagonist muscles causing limited horizontal movement of the eye. In addition, botulinum toxin may cause blepharoptosis and vertical strabismus in 20% to 40% of cases, and perforation of the globe is a rare complication. Nevertheless, despite possible side effects, botulinum toxin injection to the antagonist muscle may help avoid surgical repair by preventing contracture and allowing restoration of alignment as the paretic muscle recovers its function.
Surgery
Many patients recover spontaneously from cranial nerve palsies over 2 to 3 months, particularly if the cause is microvascular disease; however, when the cause is trauma, brain tumor, or stroke, recovery is less likely. If recovery is absent or incomplete, then surgery may be considered. Timing is important. Surgical repair should be deferred until the strabismus is stable for at least 6 months. The goals of the strabismus surgery are to straighten the eyes, alleviate the diplopia, improve the ocular rotations in the field of action of the paretic muscle, and expand the field of single binocular vision. The most important positions of gaze are primary and reading positions; therefore, shifting the field of single binocular vision into primary position is crucial to achieving a satisfactory result and alleviating compensatory head positions. To accomplish these goals, the surgeon should follow two surgical principles: (a) eliminate contractures, and (b) balance the forces. With extraocular muscle palsies, there is an imbalance of forces caused by a dead or weak agonist muscle and an unaffected antagonist muscle. The mechanical and tonic forces of the extraocular muscles and periocular tissues acting in primary position need to be balanced to achieve stability of the results.133 A dead muscle cannot be restored by shortening it. The muscle cannot be reinnervated and the tonus cannot be completely re-established; however, shortening of muscles can produce a mechanical leash or tether.
To determine the best surgical procedure for each individual patient, a precise diagnosis is required to differentiate between a muscle paresis and a complete muscle paralysis. To evaluate the degree of muscle function, it is important to test ductions, saccades, forced ductions, and force generation. Transposition procedures should be reserved for patients with complete or almost total loss of muscle function. If residual muscle function is present, it is preferable to perform a muscle-strengthening procedure rather than transposition procedures. Creating a matching motility defect by weakening the yoke muscle of the uninvolved eye may prove helpful as well.
Sixth cranial nerve palsy
Sixth cranial nerve palsies affect only the lateral rectus muscle, producing an abduction deficit with esotropia and binocular horizontal diplopia that is typically worse at distance and in the field of action of the affected muscle. Patients with sixth nerve palsies frequently prefer an ipsilateral face turn. Surgical options include either recess/resect procedures of horizontal muscles or horizontal transposition procedures of vertical rectus muscles. The most important factors when planning surgery for sixth cranial nerve palsies are the degree of function of the affected lateral rectus muscle (abducting force) and the degree of contracture of the antagonist medial rectus muscle. Generally, ipsilateral medial rectus recession is necessary if forced ductions are positive due to contracture of the medial rectus muscle. The recession may be combined with resection of the affected lateral rectus muscle if abducting force is at least 25% of normal, with amounts of surgery inversely proportional to the abducting force. Adjustable sutures are extremely useful in these cases. Weakening the yoke muscle of the uninvolved eye by recession of the contralateral medial rectus muscle, with or without posterior fixation, may be beneficial because it may increase comitance in the affected field of gaze and may increase innervational input to the affected lateral rectus muscle.
When abducting forces are minimal to absent, less than 25% of normal, it is generally agreed that transposition procedures offer a better long-term alignment. Transposition procedures shift the vector of mechanical force generated from the tonic primary position of the transposed muscle toward the field of the paretic muscle. Innervational plasticity does not occur. There is no recruitment of the transposed muscles in the field of gaze of the transposition. A modest increase in rotational ability is due to relaxation of the antagonist combined with the tonic primary position innervation of the transposed muscles.134 Transposition creates a minimal force; therefore, a minimal restriction will create a significant opposing force and limit the effectiveness of the transposition. The most important factor determining the efficacy of transposition surgery is the tone and muscle contracture of the antagonist. If the medial rectus muscle demonstrates no mechanical restriction, an excellent result will occur from the transposition procedure. However, the greater the degree of mechanical restriction, the more disappointing the surgical result. The importance of preoperative forced duction testing cannot be overemphasized.
Transposition of the vertical recti in conjunction with ipsilateral medial rectus recession involves the risk of anterior segment ischemia, particularly in the elderly. Anterior segment ischemia may result in permanent structural damage to the eye, including anterior cortical cataracts, posterior synechiae, iris atrophy, and distortion of the pupil. Although useful visual acuity is usually recovered with aggressive topical steroid therapy, severe functional impairment or even phthisis bulbi may ensue.135,136,137 For this reason, concurrent medial rectus recession is best avoided in transposition procedures. If significant mechanical contracture of the antagonist is discovered preoperatively, options include Botox injection to the antagonist, a planned two-stage procedure separated by 4 to 6 months to allow the development of collateral circulation via the posterior ciliary arteries, recession of the contracted antagonist combined with a ciliary artery vessel-sparing procedure, or a partial rectus muscle augmented transposition.138,139
Several transposition procedures have been described. Hummelsheim was the first one to use partial tendon rectus muscle transposition in 1907.140 He transposed the temporal halves of the superior and inferior rectus muscles to the lateral rectus insertion in patients with sixth cranial nerve palsy. Full tendon transposition was reported in 1959 by Schillinger.141 Several modifications have followed, including the Jensen procedure in 1964, transposing the temporal halves of the superior and inferior rectus muscles without detaching them, and the full tendon transposition with posterior augmentation by Foster in 1997.142,143 Clark et al. demonstrated that transposition without lateral fixation results in a very small shift in the inferior and superior rectus muscle belly of <3.0 mm. Posterior fixation sutures increase this shift to 5.0 mm.144 The addition of lateral fixation sutures to the full vertical muscle transposition increases the tonic abducting forces by approximately 50% in primary position, equivalent to adding a 6-mm medial rectus recession to the nonaugmented transposition.145 The advantages of augmented transpositions are avoidance of medial rectus recession with decreased risk of postoperative anterior segment ischemia and better preservation of adduction.
Fourth Cranial Nerve Palsy
Superior oblique palsy patients present with ipsilateral hypertropia that is worse in adduction and with ipsilateral head tilt. In addition to vertical diplopia, excyclotorsion is frequently demonstrated by double Maddox rod testing. Patients may assume a compensatory head posture with preference for a contralateral face turn and contralateral head tilt to alleviate the diplopia. When planning surgery for patients with a superior oblique muscle palsy, the principle of matching the field of greatest deviation to the muscles whose greatest action is in those fields, which derives from Knapp’s classification, remains useful.146 Secondary inferior oblique muscle overactions typically develop in superior oblique muscle palsies. In these cases, the forces can be balanced by weakening the ipsilateral inferior oblique muscle.133 If the hypertropia measures ≤15 D, weakening of the inferior oblique muscle should suffice and can be accomplished by either a myectomy, with removal of a 5- to 7-mm segment of the muscle, or by a recession, which can be graded according to the degree of overaction. If the hypertropia measures >15 D, a second muscle may be added. The inferior oblique weakening procedure may be combined with rectus muscle surgery, usually either recession of the contralateral yoke inferior rectus muscle or recession of the ipsilateral superior rectus, depending on which gaze position shows worse deviation and on whether superior rectus contracture is present. Secondary superior rectus contracture should be suspected if the hypertropia measures >15 to 20 D and is accompanied by apparent underaction of the ipsilateral inferior rectus and superior oblique overaction in the fellow eye.133 If the hypertropia measures ≥30 D, a three-muscle surgery should be considered.
If no inferior oblique overaction is present, recession of one or more rectus muscles, or a recess-resect procedure of the vertical recti can be done. The number of muscles to be operated will depend on the angle of the hypertropia. The rule of thumb is one muscle for hypertropia of ≤15 D, two muscles for deviations between 15 and 30 D, and three muscles for larger deviations. Adjustable sutures are frequently employed with rectus muscle surgery.
In cases with symptomatic excyclotorsion but no inferior oblique overaction, a superior oblique strengthening procedure is indicated. A superior oblique tendon tuck is used in cases accompanied by hypertropia. The primary complication of this procedure is the postoperative iatrogenic Brown syndrome in 60% of cases, which manifests as a limitation to elevation in adduction. Despite this, the consecutive Brown syndrome is not a common cause of reoperation. Furthermore, Simons et al.147 found that isolated oblique muscle surgery appears superior to vertical rectus surgery in obtaining a successful outcome, with a smaller rate of reoperations. Harada-Ito procedures are reserved for cases with symptomatic excyclotorsion with minimal or no hyperdeviation. With this technique, which can be performed on an adjustable suture, the anterior fibers of the superior oblique tendon are brought anteriorly and temporally, achieving correction of approximately 10 degrees of excyclotorsion.148
In many cases of bilateral superior oblique palsy, particularly when symmetric, there is no significant strabismus in primary position. Symptoms often arise from excyclotropia, usually in excess of 10 degrees, V-pattern esodeviation in downgaze, right hypertropia in left gaze and right head tilt and left hypertropia in right gaze and left head tilt. These patients may benefit from bilateral Harada-Ito procedures, bilateral superior oblique tendon tucks, or bilateral inferior oblique recessions, when cyclodiplopia is present.149 Bilateral inferior rectus recessions can be used in mild cases, but may not correct large degrees of excyclotorsion. Medial rectus recessions with infraplacement alleviates esotropia in downgaze.
Third cranial nerve palsy
Oculomotor nerve palsies present with exotropia due to an adduction deficit, which may be accompanied by vertical strabismus, depending on the degree of involvement of the vertical rectus muscles and the inferior oblique muscle. Complete paralysis of the third cranial nerve typically produces a large exotropia and hypotropia with blepharoptosis. In cases with absent vertical rectus function, a supramaximal recession of the lateral and resection of the medial rectus muscle may be the best option. The lateral rectus needs to be placed as far back as possible, usually 14 to 16 mm behind the insertion in an attempt to balance the dead forces. The medial rectus needs to be resected to create a leash to hold the eye in primary position. In addition, both horizontal muscles can be supraplaced 1 mm for each 2 D of hypotropia in primary position (modified Knapp procedure) to improve the ocular alignment.150 Unfortunately, if the medial rectus muscle is dead, the forces are never completely balanced and the exotropia tends to recur, with patients requiring reoperations. Transposition of the superior oblique tendon to 2 to 3 mm anterior to the medial aspect of the superior rectus muscle insertion may help prevent the recurrent exotropia.151 The superior oblique should not be placed close to the medial rectus insertion because this may induce hypertropia and excyclotorsion. Inactivation of the lateral rectus muscle by extirpation, free tenotomy, or myectomy, or by attaching its insertion to the orbital periosteum with nonabsorbable sutures, may also prevent recurrent exotropia.152 Orbital periosteum fixation offers the advantage of reversibility. If there is preservation of function of the vertical rectus muscles, then nasal transposition to the medial rectus muscle insertion can be done, following the same principles of transposition of vertical recti in sixth cranial nerve palsy. Nasal transposition of the vertical recti, however, unlike temporal transposition, requires a small resection of each muscle. The decreased effect of nasal transpositions as compared to temporal transpositions is a result of the vertical recti anatomic orientation in a nasal-to-temporal direction in relationship to orientation of the visual axis.134 Once the strabismus is improved, patients with complete oculomotor nerve palsy require blepharoptosis repair. Due to the absent Bell’s phenomenon, there is an increased risk of corneal exposure; therefore, a conservative approach is recommended.
When managing patients with cranial nerve palsies, the principle of balancing dead forces is paramount. As stated by Jampolsky, “With principles the solution to these problems may be awfully simple; without principles the solution may be simply awful.”133
Ischemic (“Diabetic”) Oculomotor Palsy
As noted in the discussion of fourth and sixth nerve palsies, self-limited vasculopathic extraocular muscle pareses may be associated with diabetes, although the incidence of ophthalmoplegia in diabetes is relatively rare. Often, the patient is an adult with latent diabetes first brought to light during the evaluation of the acute ophthalmoplegia. A large series by the authors noted that 14% of more than 2,000 ocular motor cranial neuropathies seen over a 5-year period were due to diabetes.153 Fifty percent involved the sixth nerve, 43% the third nerve, and only 7% the trochlear nerve. For reasons that remain unclear, the prevalence of diabetic retinopathy in these patients is less than would be expected for age-matched diabetics without cranial neuropathies. Although recurrences, on either the same or opposite side and involving either the same or other nerves (III, IV, VI), are possible, they are relatively rare (4% in the authors’ series), as is simultaneous involvement of two or more ocular motor nerves (<3% in the same series),153 and both should be viewed with caution.156 We may enunciate a useful clinical dictum: A patient with diabetes is permitted one cranial neuropathy at a time; exceptions to this rule, that is, either more than one motor nerve per eye, or simultaneous bilateral cranial palsies, make investigation mandatory. Nevertheless, Eshbaugh et al.157 reported three patients with multiple simultaneous bilateral cranial neuropathies secondary to diabetes mellitus, all of which spontaneously resolved without sequelae.
Clinically, patients with ischemic oculomotor palsy present with acute pain in and about the involved eye. The pain may precede actual ophthalmoplegia and can be so severe as to suggest a bleeding aneurysm (but without neck stiffness, photophobia, obtundation, etc.), or it may accompany the onset of ptosis or diplopia as a mild brow pain or headache. The pupil is almost always spared, in contradistinction to posterior communicating artery aneurysm. Some degree of internal ophthalmoplegia occurs in approximately one-third of patients but is minimal, and anisocoria rarely exceeds 1 to 2 mm.158 Ophthalmoplegia may be partial, with some muscles spared entirely (Fig. 12.14). Recovery is predictable, occurring after several weeks and usually within 4 months.
 Figure 12.14 Ischemic (diabetic) right oculomotor ophthalmoplegia of mild degree. A: Note failure of adduction on left gaze and unusual lack of ptosis. B: Pupil is spared, with intact light reaction. C: Superior rectus weakness. D: Inferior rectus weakness. Mild pain accompanied onset of diplopia, with complete resolution in 3 weeks. This was the second episode in a 62-year-old patient with known diabetes. |
Studies by Weber et al.159 and Asbury et al.160 have indicated the following: (a) the lesion is primarily a focal demyelinization with minimal axonal degeneration; (b) remyelinization is believed to be responsible for recovery without aberrant regeneration; and (c) ischemia due to closure of intraneural arterioles is believed to cause the demyelinative lesion, which may occur in the intracavernous160 or subarachnoid159 segment of the third nerve. However, the advent of MRI has clearly demonstrated that intraparenchymal midbrain lesions may be responsible for pupil-sparing ophthalmoplegia.161,162
The key to diagnosis is threefold: a high level of suspicion should be entertained when a middle-age or elderly person (a) presents with a pupil-sparing ophthalmoplegia involving all or most of the ocular muscles innervated by the third nerve only (with or without accompanying pain); (b) has elevated serum glucose levels either during fasting or after a measured or elevated glucose load or an elevated, glycosylated hemoglobin (hemoglobin A1c), reflecting mean glycemia over the preceding 2 to 3 months; and (c) has a documented recovery within 3 to 4 months. The significant proportion of cranial nerve pareses due to diabetes or another microvascular disease cannot be overemphasized. The Mayo Clinic has reviewed more than 4,000 cases of third, fourth, or sixth cranial nerve palsy.47 Similar to the data noted previously, slightly more than 15% of all cranial neuropathies were attributed to vascular causes (e.g., diabetes, hypertension, atherosclerosis). Note, however, that these figures pertain to adults only: Microvascular cranial neuropathies do not occur in the pediatric population. We would again caution the clinician regarding cases of partial ophthalmoloplegia and partial pupillary involvement. Jacobson163 reported 24 cases of third nerve paresis with anisocoria between 0.5 and 2.0 mm. Approximately half of these were found to have tumors or aneurysms, whereas the other half were microvascular in origin; thus, in cases where etiology is initially unclear, erring on the side of caution with appropriate neuroimaging is wise. A final clinical consideration is that, due to the near-universal rate of spontaneous improvement, ischemic oculomotor paresis do not develop cholinergic hypersensitivity of the iris sphincter; however, long-standing palsies, as may be due to compressive lesions, may develop a supersensitivity similar to that seen in Adie syndrome.164
Because the vast majority of patients with ischemic ocular motor palsies enjoy complete or near-complete spontaneous recovery, management generally consists of monocular occlusion and observation. However, one report suggests that treatment with systemic alpha-lipoic acid, which has been shown to improve peripheral diabetic neuropathy, enhances recovery of ophthalmoplegia, with significant improvement occurring within 2 weeks.165
Oculomotor Synkinesis
Since the era of Ramon y Cajal, it has been appreciated that, following trauma, regenerating axons of peripheral motor nerves may randomly access structures other than those originally innervated. This neurophysiological phenomenon accounts for intrafacial dyskinesias following seventh nerve palsies, or for paradoxic gustatory facial sweating (Frey syndrome) and gustatory tearing (“crocodile tears”) with misdirection of regenerated autonomic axons. Because the oculomotor nerve innervates multiple extraocular muscles, the levator palpebrae, and the pupil sphincter, aberrant innervation patterns may be produced by misdirected axonal sprouting after injury, producing variable patterns of dyskinetic ocular movement.
The precise mechanism whereby oculomotor synkinesis occurs is controversial and unsettled. Sibony et al.167 reviewed the various hypotheses proposed to explain oculomotor synkinesis. Random misdirection of regenerating motor axons within an injured oculomotor nerve trunk, with erroneous muscle reinnervation, is the traditional explanation for oculomotor synkinesis, and indeed histopathological, clinical, and experimental evidence may be cited in support of this hypothesis.168 But transient oculomotor synkinesis,169,170,171 spontaneous “primary” oculomotor synkinesis,169,172,173,174,175 and synkinesis involving superior and inferior divisions of the third nerve after damage to only the superior division112 have been observed and are difficult, but not impossible,167 to explain by the hypothesis of indiscriminate axonal regeneration. Such clinical oddities prompted Lepore and Glaser169 to challenge the concept that misdirection of regenerating oculomotor fibers is responsible for all oculomotor synkinesis and to invoke two alternative mechanisms: (a) ephaptic transmission (axo-axonal “cross-talk”) and (b) synaptic reorganization of the oculomotor nucleus following retrograde axonal degeneration.
After acute ophthalmoplegia, clinical signs of dyskinesia begin at about 8 to 10 weeks, accompanying variable degrees of recovered function (Fig. 12.15). When recovery begins earlier, synkinesia is less frequent—and, of course, when there is no recovery, there is no synkinesia. Several paradoxic patterns may evolve: elevation of the upper lid on attempted use of the inferior (pseudo-von Graefe sign) or medial rectus muscles (“reverse Duane” syndrome) (Fig. 12.13); adduction or retraction of the globe on attempted downward or upward gaze; and a light-near (or lateral gaze) pupillary dissociation with constriction of a larger than normal pupil occurring on attempted adduction. According to Hepler and Cantu,176 of 25 patients with aberrant oculomotor regeneration after posterior communicating artery aneurysms, 20 demonstrated the pseudo-von Graefe phenomenon of lid elevation on attempted downgaze. This critical sign is best appreciated by first directing the patient’s gaze downward, and then slowly from side to side. Czar neki and Thompson177 reported other pupillary anomalies, including asynchronous sectoral contractions with both light stimulation and eye movement.
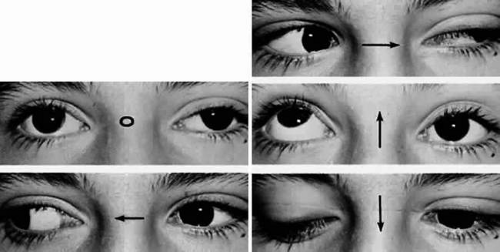 Figure 12.15 Aberrant regeneration of left oculomotor nerve following head trauma. Note modest limitation of medial rectus function and marked deficit of superior rectus. On attempted downward gaze (inferior rectus), the left lid elevates, that is, the pseudo-Graefe phenomenon. |
Oculomotor synkinesis is frequently observed in congenital third nerve palsies.43,178,179,180 The spontaneous and progressive development of oculomotor synkinesis in patients with no prior acute oculomotor palsy169,172,173,174,175 is seen most commonly with slowly growing lesions in the cavernous sinus, usually meningiomas or aneurysms, and has been termed primary oculomotor synkinesis. Both Varma and Miller181 and Carrasco et al.182 pointed out that although aneurysms typically present with acute, painful oculomotor pareses, they may produce painless third nerve palsies with primary aberrant regeneration. Secondary oculomotor synkinesis?that is, synkinesis following recognized acquired oculomotor palsy?most commonly occurs in association with trauma or aneurysms, but may rarely be seen with neoplasia or even ophthalmoplegic migraine.183 Misdirection has been reported only twice after ischemic (diabetic) ophthalmoplegia or demyelinative syndromes,184 but in the authors’ opinion, the purported synkinesis in these patients, if indeed present, is extremely subtle, much unlike the very obvious type found in compressive or traumatic palsies.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


