Purpose
To examine the relationship between refractive error and optic disc topographic parameters and retinal nerve fiber layer (RNFL) thickness.
Design
Population-based cross-sectional study.
Methods
All 3280 (78.7% response rate) persons of Asian Malay ethnicity 40 to 80 years of age underwent a standardized interview, ocular examinations, and optic disc imaging with the Heidelberg Retina Tomography II (HRT; Heidelberg Engineering). Associations between spherical equivalent (SE) and HRT parameters were evaluated by partial correlation analysis.
Results
There were 2457 (74.9%) right eyes with good-quality HRT images for analyses. When compared with emmetropic eyes, highly myopic eyes (SE < −6.0 diopters) had greater disc area, rim area, rim volume, whereas hyperopic eyes (SE > 0.5 diopters) had significantly smaller disc area, rim area, and cross-sectional RNFL area (all P < .005). In partial correlation after adjustment for age, sex, body mass index, intraocular pressure, and optic disc area, increase of SE (toward hyperopia) was related significantly with greater cup area (partial correlation coefficient, r = 0.058; P = .004) and cup-to-disc area ratio ( r = 0.058; P = .004) and with smaller optic disc area ( r = −0.058; P = .004), rim area ( r = 0.058; P = .004), and rim volume ( r = −0.091; P < .001).
Conclusions
This population-based study shows that refractive error is significantly (but weakly) associated with HRT parameters of disc area, cup area, rim area, cup-to-disc area ratio, and rim volume. The clinical significance of these associations need to be determined in further studies.
Morphologic assessment of the optic nerve head is essential for the diagnosis of glaucoma and evaluation of progression. Controversy exists with regard to the influence of refractive error on optic disc parameters, such as the optic disc area and neuroretinal rim area. The Rotterdam Study showed that the optic disc area and rim area increased (by 0.033 mm 2 and 0.029 mm 2 , respectively) for each 1-diopter increase in myopia, whereas a hospital-based study of eyes from white persons and a population-based study on Chinese eyes found that the optic disc size is independent of refractive error within the spherical equivalent (SE) range of −8 to +4 diopters (D). In a Chinese population-based study, the rim area of highly myopic eyes was not significantly different from that of mildly myopic eyes.
The Heidelberg Retina Tomograph (HRT; Heidelberg Engineering, Heidelberg, Germany) is a confocal scanning laser ophthalmoscope that can measure optic nerve head parameters and the retinal nerve fiber layer (RNFL) thickness more precisely and objectively. HRT has been used widely to diagnose glaucomatous optic neuropathy. However, its use is only accurate within a specific range of refractive error; it has been reported that in myopic eyes, the HRT had a lower diagnostic accuracy of glaucoma. There are few population-based data of the influence of ametropia on HRT parameters, with the Tajimi study reporting associations between myopia and some HRT parameters in a Japanese population. In the present analysis, we examined the relationships of refractive errors with optic disc and RNFL parameters based on HRT measurements in a population-based study in Singapore.
Methods
Study Population
The Singapore Malay Eye Study was a population-based cross-sectional study of 3280 (78.7% response rate) Malay subjects 40 to 80 years of age. The Singapore Malay Eye Study was conducted to quantify the prevalence of and risk factors for age-related eye diseases in people of Malay ethnicity in Singapore. The study methodology has been described previously. In brief, an age-stratified random sampling procedure was used to select people of Malay ethnicity 40 to 80 years of age living in the southwestern part of Singapore. This study was conducted in accordance with the World Medical Association Declaration of Helsinki, and ethics approval was obtained from the institutional review board.
The results reported herein were part of a series of secondary analyses from the Singapore Malay Eye Study. For this analysis, we included in the analysis only the HRT images with good quality. Images with a mean pixel height standard deviation of more than 50 μm were excluded. Furthermore, eyes with a history of intraocular surgery (including cataract, glaucoma, and vitreoretinal surgeries) or retinal laser photocoagulation, glaucoma, severe diabetic retinopathy, or retinal vein occlusion were excluded. In addition, eyes with SE less than −12 D also were excluded according to the operating manual of the HRT II.
Measurements
All participants underwent a standardized interview, systemic and ocular examination, and ocular imaging at a centralized study clinic. Relevant portions of the examination are presented here. The refraction (sphere, cylinder, and axis) of each eye was measured using an autorefractor machine (Canon RK 5 Auto Ref-Keratometer; Canon Inc Ltd., Tochigiken, Japan), the corneal curvature radius in the horizontal and vertical meridian was measured at the same time, and the mean of 2 corneal curvature radius readings was obtained. Manual subjective static refraction was then used to refine vision, using the results of the objective refraction as the starting point. In this study, refraction data were obtained from subjective refraction techniques. If subjective refraction was not available, autorefraction data were used instead. SE was defined as sphere plus half cylinder. Myopia was defined as follows: (1) mild to moderate myopia, SE less than −6.0 D; and (2) high myopia, SE of −6.0 D or less. Emmetropia was defined as SE from −0.5 to 0.5 D, and hyperopia was defined as SE more than 0.5 D. Five central corneal thickness measurements were obtained from each eye with an ultrasound pachymeter (Advent; Mentor O & O, Norwell, Massachusetts, USA) and the median reading was obtained. Noncontact partial coherence laser interferometry (IOLMaster version 3.01; Carl Zeiss Meditec AG, Jena, Germany) was used to measure axial length.
Slit-lamp biomicroscopy (model BQ-900; Haag-Streit, Köniz, Switzerland) was performed to identify abnormalities of the anterior segment. Intraocular pressure (IOP) was measured using a Goldmann applanation tonometer (Haag-Streit). After pupil dilation, the optic disc and the retina were evaluated with a +78-D lens at a slit lamp. Glaucoma cases were defined according to the International Society for Geographical and Epidemiological Ophthalmology criteria.
Height was measured using a wall-mounted tape and weight with a digital scale (SECA model 782 2321009; Vogel & Halke, Hamburg, Germany). Body mass index was calculated as weight (in kilograms) divided by height in square meters.
Heidelberg Retina Tomography Imaging
HRT II uses a diode laser (670-nm wavelength) to scan the optic disc and parapapillary retina sequentially with the field of view set at 15 degrees. HRT scans were conducted through dilated pupils. Corneal curvature radius was entered into the HRT II software for all subjects, and cylindrical lens power was adapted for those with astigmatism of 1 D or more. Magnification errors were corrected using subjects’ refractive status and corneal curvature measurements. All HRT II examinations were performed by 2 trained operators. The HRT II optic nerve head scan protocol generates a mean topographic image with a resolution of 384 × 384 generated from 3 individual topographic images.
After completion of the study, the optic disc margin or contour line was defined and manually outlined by a trained ophthalmologist. This step was accomplished by plotting a series of 6 dots around the disc margin on the reflectance image. The disc margin was defined as the inner edge of the Elschnig ring. The standard reference plane was defined at 50 μm posterior to the mean contour line height between 350 and 356 degrees along the contour line. Global optic nerve head parameters were measured and calculated by the HRT II software.
Statistical Analysis
Statistical analysis was performed using SPSS software version 17.0 (SPSS, Inc, Chicago, Illinois, USA). Because the correlations between the 2 eyes for optic disc parameters were high (e.g., correlation coefficients between right and left eyes for optic disc area, 0.85), only the data from right eyes were included in the analysis. The independent t test or chi-square test was used to test the differences of demographic characteristics between included and excluded participants. Analyses of covariance (ANCOVA) were performed to estimate the differences in the HRT parameters between eyes with different refractive status. Because it has been reported that age, sex, body mass index, IOP, and disc area are confounders for optic disc HRT parameters, partial correlation models adjusted for these confounding factors were used to examine the relationships of SE with HRT parameters. The significance level was set at P < .005 (0.05/10) to correct for multiple comparisons (Bonferroni correction).
Results
Of 3280 participants, after excluding eyes as stated above, 2457 right eyes (74.9%) were included for the final analyses. In general, excluded subjects had an older age, higher levels of systolic blood pressure, and higher prevalence of hypertension and diabetes, but lower prevalence of current smoking. In addition, excluded eyes had smaller mean central corneal thickness but similar axial length and IOP.
Table 1 shows the HRT parameters of the study subjects with different refractive status. When compared with emmetropic eyes, highly myopic eyes had significantly greater optic disc area ( P = .004), neuroretinal rim area ( P = .001), and rim volume ( P < .001), whereas hyperopic eyes had significantly smaller disc area ( P < .001), rim area ( P < .001), and RNFL cross-sectional area ( P < .001). HRT parameters of mild-to-moderately myopic eyes were not significantly different from those of emmetropic eyes (all P > .005).
| HRT II Parameters | All (N = 2457) | High Myopia (n = 44) | Mild to Moderate Myopia (n = 508) | Emmetropia (n = 1026) | Hyperopia (n = 879) | |||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | P value a | Mean (SD) | P value a | Mean (SD) | Mean (SD) | P value a | ||
| Disc area, mm 2 | 2.14 (0.47) | 2.32 (0.75) | .004 | 2.15 (0.49) | .34 | 2.17 (0.47) | 2.09 (0.44) | <.001 b |
| Cup area, mm 2 | 0.59 (0.39) | 0.49 (0.36) | .09 | 0.59 (0.42) | .78 | 0.59 (0.39) | 0.58 (0.39) | .41 |
| Rim area, mm 2 | 1.55 (0.32) | 1.74 (0.59) | .001 b | 1.56 (0.36) | .30 | 1.58 (0.31) | 1.51 (0.30) | <.001 b |
| Cup-to-disc area ratio | 0.26 (0.14) | 0.20 (0.13) | .015 | 0.26 (0.15) | .96 | 0.26 (0.13) | 0.26 (0.14) | .66 |
| Cup volume, mm 3 | 0.12 (0.13) | 0.09 (0.12) | .07 | 0.12 (0.13) | .77 | 0.13 (0.13) | 0.12 (0.12) | .15 |
| Rim volume, mm 3 | 0.41 (0.15) | 0.51 (0.20) | <.001 b | 0.42 (0.17) | .13 | 0.41 (0.14) | 0.39 (0.14) | .02 |
| Mean cup depth, mm | 0.21 (0.08) | 0.20 (0.10) | .43 | 0.21 (0.09) | .87 | 0.21 (0.09) | 0.21 (0.08) | .11 |
| Cup shape measure | −0.17 (0.07) | −0.18 (0.08) | .32 | −0.17 (0.07) | .14 | −0.17 (0.07) | −0.17 (0.06) | .02 |
| Mean RNFL thickness, mm | 0.25 (0.08) | 0.28 (0.11) | .016 | 0.25 (0.09) | .62 | 0.25 (0.07) | 0.25 (0.07) | .02 |
| RNFL cross-sectional area, mm 2 | 1.29 (0.40) | 1.41 (0.51) | .12 | 1.29 (0.46) | .29 | 1.31 (0.38) | 1.25 (0.38) | <.001 b |
a Compared with emmetropia, analysis of variance.
b P < .005 (0.05/10, with Bonferroni correction for multiple comparisons).
The relationship of SE with optic disc area is shown in the Figure . A significant but weak ( R 2 = 0.010; P = .004) association between SE and optic disc area was observed.
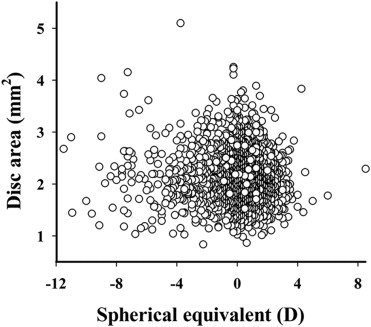
Table 2 shows the relationship of SE with HRT parameters in the study population in multiple linear regression models. In all participants with an SE range of −11.5 to +8.5 D, after adjustment for age, sex, body mass index, IOP and optic disc area, increase of SE (toward hyperopia) was significantly related to greater cup area (partial correlation coefficient: r = 0.058; P = .004) and cup-to-disc area ratio ( r = 0.058; P = .004) and with smaller optic disc area ( r = −0.058; P = .004), rim area ( r = 0.058; P = .004), and rim volume ( r = −0.091; P < .001).
| HRT II Parameters | Partial Correlation Coefficient a | P Value |
|---|---|---|
| Disc area, mm 2 | −0.058 | .004 b |
| Cup area, mm 2 | 0.058 | .004 b |
| Rim area, mm 2 | −0.058 | .004 b |
| Cup-to-disc area ratio | 0.058 | .004 b |
| Cup volume, mm 3 | 0.053 | .009 |
| Rim volume, mm 3 | −0.091 | <.001 b |
| Mean cup depth, mm | 0.033 | .10 |
| Cup shape measure | 0.045 | .026 |
| Mean RNFL thickness, μm | −0.002 | .93 |
| RNFL cross-sectional area, mm 2 | 0.014 | .48 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


