Infectious Diseases
Alex V. Levin
Thomas W. Wilson
Nasrin Najm-Tehrani
Virtually every infectious disease may affect the eye either through direct infection, hematogenous spread, contiguous spread, or complications related to a primary infection at another site. This chapter focuses on ocular complications of systemic and remote infection. Diagnosis of the ocular manifestation might require culture from a site remote from the eye or, less commonly, sampling of intraocular fluids or tissues. Given the difficulty in obtaining intraocular tissues for culture, careful attention to remote sites for diagnostic culture or titers becomes essential.
Suspicion of an infectious cause for an ocular abnormality might stem from the presence of systemic signs such as fever, shock, or other more localized indicators. The presence of infection in the cerebrospinal fluid or blood is particularly worrisome with regard to potential ocular involvement. Transplacental spread of infection to a fetus may present with multiorgan system involvement or even malformations. Taking a careful history is another powerful diagnostic tool and should include queries regarding contacts and exposures, course of the illness, other systemic indicators of infection, treatment with antibiotics or other agents, contact with pets and other animals, travel, and, in the case of suspected fetal infection, pregnancy history. Diagnostic studies on family members (e.g., the mother in a case of suspected fetal infection) may be appropriate in some circumstances.
Some ocular complications of systemic and remote infectious disease are treated by topical or intraocular agents, whereas others require systemic treatment. When diagnostic tissue culture is not obtainable, broad-spectrum antibiotic coverage may be appropriate. The American Academy of Pediatrics Red Book is a particularly useful reference for diagnosis and treatment guidelines.
 Figure 19.1 Gradenigo Syndrome Aggressive bacterial otitis media can lead to involvement of the petrous bone and mastoid. Cranial nerve VI runs over the intracranial petrous bone on its way to the ipsilateral lateral rectus muscle. Inflammation in the intracranial space can result in an abduction deficit, as shown in this child’s right eye (Chapter 1: Strabismus, Fig. 1.51). Other diagnostic findings include otitis media, papilledema from increased intracranial pressure, signs of systemic illness (in particular pain, fever, and headache), and diagnostic inflammatory signs in the region of the petrous bone with or without mastoiditis on computed tomography scan or magnetic resonance imaging. |
 Figure 19.2 Necrotizing Fasciitis/ Flesh-eating Disease Necrotizing fasciitis is a cutaneous disease with aggressive destruction of the skin and underlying tissues. Skin injury almost always precedes the infection. Death can result within days. The infection is caused by anaerobic bacteria with or without aerobic bacteria or group A streptococcus (as shown in the photograph). Pain and fever are key signs, along with a characteristic feathery appearance to the infected area with air on computed tomography or magnetic resonance imaging. Debridement and a variety of antibiotics have been the cornerstone of treatment. Hyperbaric oxygen therapy has also been used. Survivors usually require extensive reconstructive plastic surgery. |
 Figure 19.3 Toxoplasmosis Toxoplasmosis is an infectious disease caused by the protozoan Toxoplasma gondii. Humans acquire the infection from ingestion of oocysts contained within cat feces or undercooked meat. Congenital toxoplasmosis occurs following transplacental transmission of the protozoan and presents with the classic triad of chorioretinitis, hydrocephalus, and intracranial calcification. This photograph shows optic atrophy and a typical dense chorioretinal scar, typically located in the macula. Diagnosis of toxoplasmosis can be confirmed by serology tests. Treatment modalities include pyrimethamine and sulfadiazine. |
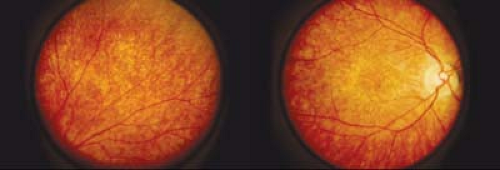 Figure 19.4 Congenital Rubella Clinical findings of congenital rubella include posterior cervical and retroauricular adenopathy, a rash on the soft palate and pharyngeal mucosa, growth and mental retardation, congenital heart defects (especially peripheral pulmonic stenosis), hearing loss, hepatosplenomegaly, intracranial calcification, and thrombocytopenic purpura. Ocular manifestations include cataracts, glaucoma, microphthalmia, and corneal endotheliitis. Active virus can be isolated from the lens for diagnosis. Retinal pigmentary disturbances include a “salt and pepper” mottling due to internal limiting membrane gliosis and retinal pigment epithelium hyperplasia. The vision tends to be normal with a normal electroretinogram, which differentiates this condition from other retinal dystrophies. Retinal blood vessels and the optic nerve may appear surprisingly healthy. |
 Figure 19.5 Herpes Simplex Herpes simplex virus type I (and less commonly type II) primary infection typically occurs within the first decade following contact with an adult with oral herpes and presents with aphthous stomatitis, dermatitis, or conjunctivitis. The herpes simplex virus becomes latent within the trigeminal ganglion. Factors that may cause recurrence include stress, ultraviolet radiation, menses, fever, and trauma. The skin lesions typically clear within 1 to 2 weeks without significant scarring, although they may become secondarily infected with bacteria and cause a preseptal cellulitis. Approximately 25% of patients with primary herpetic conjunctivitis will develop keratitis including superficial punctate keratitis, subepithelial infiltrates, and possibly dendrites. Patients with primary herpetic conjunctivitis should be treated with topical antiviral ointment or drops.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|