
Signs of bacterial superinfection include the following (Fig. 10.4):
▪ Eyelash folliculitis with ulceration near the lash bases and fibrinous collarettes
▪ Eyelash follicle damage, resulting in short, misdirected, or absent eyelashes
▪ Stye or external hordeolum, a focal abscess within the gland of Zeis
▪ Multiple chalazia, resulting from retained Meibomian secretions from inflamed orifices
▪ Internal hordeolum, a secondary infection of the chalazion
▪ Corneal changes, including inferior epithelial keratitis or marginal autoimmune ulcers
▪ Foamy tears and discharge from soaps created by bacterial lipases.

Angular blepharitis presents with redness, scaling, and fissuring of the lateral canthus, often associated with lateral conjunctivitis and discharge.
Fungal lid margin infections with Candida may show ulcerations, pustules, or small granulomas.
Infestation with P. pubis (crab lice) is characterized by itching and inflammation of the lid margin with translucent lice egg cases (nits) bound to the eyelash hairs. The adult louse is well camouflaged, but a known history of body hair infestation should trigger suspicion.
Controversy: Demodex folliculorum can be associated with chronic blepharitis, although its role and frequency in pathogenesis is uncertain. It is identified by transparent sleeves extending from the eyelash follicle along the base of the lashes.15
Investigations
Cultures of eyelid margin flakes or discharge may identify pathogens and sensitivities. Mites may be seen on microscopy on epilated lashes (Fig. 10.5).

Management
Seborrheic blepharitis is managed with antiseborrheic shampoos and lid hygiene using dilute bland soaps to remove lid margin flakes.18
Posterior meibomitis is treated with warm compresses, eyelid massage, and focal lid scrubs.
Controversy: Fish oil supplements may improve tear lipid composition. Microprobing and focal variable compression with heated clamps (Lipiflow) remain controversial.18,19
Topical ophthalmic tobramycin or bacitracin may reduce surface bacterial overgrowth, and topical or oral azithromycin improves oil secretions and reduces inflammation.
Systemic tetracyclines (doxycycline 100 mg daily) for several months may reduce infective blepharitis and rosacea. Topical metronidazole ointment 0.75% gel (Metrogel) is useful for cutaneous acne rosacea.
Topical corticosteroid ointment reduces inflammation and aids lipid flow. Supratarsal subcutaneous injections of dexamethasone phosphate solution or triamcinolone suspension are helpful for small chalazia and focal meibomitis, but embolic blindness has been reported with periorbital injections of suspensions.
Topical ketoconazole may be used for infections with Candida and Malassezia. Lice are smothered with lubricant or antibiotic ointment while body hair is treated with permethrin 1% cream rinse (Kwellada-P). Demodex may respond to scrubbing the lid margins with half-strength tea tree oil.20
Chalazia and hordeola may be incised and curetted if sufficiently large.
Complications and Prognosis
Infective blepharitis is a chronic condition that requires ongoing measures for control and may lead to oil gland destruction, eyelash damage, lid margin distortion, and corneal ulceration or scarring. It may cause preseptal or rarely orbital cellulitis.
Impetigo and Erysipelas
Pathogenesis and Etiology
Impetigo contagiosum involves the superficial skin layers and is usually caused by S. aureus or Streptococcus pyogenes. The “bullous” form causes blisters in the superficial epidermis with acute dermal inflammation, and the “common” form shows acute inflammatory cells and serum within epidermis and dermal layers. The disease is spread through direct contact, often through a small break in the skin.21
Erysipelas (St Anthony’s fire) is a rare infection typically associated with pharyngitis caused by β-hemolytic Group A or B Streptococcus species (S. pyogenes and S. agalactiae). Exotoxins induce a well-defined rash involving the superficial dermis and lymphatics. It does not involve subcutaneous tissue, unlike preseptal cellulitis or necrotizing fasciitis.22 Necrotizing fasciitis of the eyelids is discussed later under “Preseptal cellulitis”.
Epidemiology
Impetigo is often seen in young children or their caregivers. Those with eczema and atopic dermatitis are at higher risk. Erysipelas is most frequent in the young, older adults, and the immunosuppressed.
Clinical Features
Impetigo presents as pustular lesions and round red patches at the site of eczema or minor trauma. The bullous type forms clear blisters, whereas the common type forms yellow crusts (Fig. 10.6).

Erysipelas is a rapidly expanding, painful, bright red skin lesion with raised, well-defined margins. Its texture may be rough and form small blisters or zones of necrosis. Surrounding lymph nodes and lymphatics are often painful, and there may be associated fever, rigors, and headache. The periorbital areas and nose are frequently involved22 (Fig. 10.7).

Investigations
Wound cultures may be useful for impetigo but have a poor yield for erysipelas; blood cultures are occasionally positive with the latter.
Management
Impetigo lesions are soaked with warm dilute vinegar and treated with fusidic acid ointment. Oral cloxacillin or trimethoprim-sulfamethoxazole (TMP-SMZ) for MRSA are prescribed for bullous disease. Contacts should be examined if symptomatic and nasal passages cultured and treated with topical mupirocin, although eradication is difficult.21
Erysipelas is treated with oral or intravenous antibiotics against streptococcal species. Penicillin and its derivatives or clindamycin for at least 7 days is recommended. Because of recurrences, nasal flora should be cultured and treated.
Complications and Prognosis
Bacteria causing impetigo and erysipelas may spread into subcutaneous layers, resulting in preseptal cellulitis or necrotizing fasciitis. Hematogenous extension via orbital veins may result in orbital cellulitis or cavernous sinus thrombosis. Streptococcal bacteremia may result in glomerulonephritis or arthritis.
Fungal Eyelid Infections
Pathogenesis and Etiology
Human fungus such as Trichophyton rubrum may be transmitted from sites elsewhere on the body including feet, nails, or groin or from other infected humans. Animal fungi such as Microsporum canis23 may be inoculated directly from infected pets. Some fungi such as Blastomycosis are regional and may be associated with life-threatening systemic infections24 (Fig. 10.8).

Epidemiology
Athletes, the immunocompromised, and those with pets are most susceptible.
Clinical Features
Fungal infections may present with oval scaly red patches with central pallor (“ring worm”). Eyelash loss is a frequent finding.23
Investigations
Lesion scrapings or biopsy may reveal hyphae on pathology and is often more sensitive than cultures.
Management
Suspected eyelid fungal infections are often treated empirically with topical ketoconazole with or without corticosteroid. Oral itraconazole may be necessary for more virulent organisms such as Blastomycosis.
Viral Papillomas: Molluscum and Warts
Pathogenesis and Etiology
Viral warts are caused by 130 different types of human papilloma virus (HPV): different types affect specific regions of the body. These infect the nucleus of squamous epithelium, causing hyperplasia and hyperkeratosis. Those involving the eyelid region have no malignant potential.
Molluscum contagiosum virus is a member of the Poxviridae family that affects only humans. Four types have been categorized: type 1 is responsible for over 95% of infections in immunocompetent individuals, and type 2 is isolated in the majority of cases associated with human immunodeficiency virus (HIV) infection. It invades the cytoplasm of cutaneous epithelial cells, presumably through an area of microtrauma, expanding the cells until they rupture and release virus for further transmission. Inoculation is through direct contact from one individual to another, through autoinoculation, and through contaminated shared towels and athletic equipment.
Epidemiology
Athletes, young children and their caregivers, and the immunocompromised (especially HIV-positive individuals) are most susceptible to molluscum.
Clinical Features
Viral warts affecting the eyelid are skin tags with a serrated surface that may be broad based (sessile, verruca plana) or pedunculated (filiform) (Fig. 10.9A and B).

Molluscum contagiosum presents as single or clustered papules in moist areas of the body, including armpits, groin, and lid skin. They are 1 to 4 mm in size and white to brown in color (Fig. 10.10A). Occasionally, larger lesions up to 2 cm develop in HIV-positive individuals (Fig. 10.10B). They have a waxy surface with a central pit (umbilicated), from which the soft white core (molluscum body) containing virus may be shed or expressed. There may be an associated red, flaky dermatitis and follicular conjunctivitis from lesions near the lid margin.25

Investigations
Usually diagnosed clinically but histopathology of biopsied specimens confirms the diagnosis (Fig. 10.9C, and Fig. 10.10C).
Management
Viral warts may regress spontaneously. Simple excision with cautery is effective and safer than chemical therapies. Molluscum lesions may be abraded, curetted, or excised.25
Complications and Prognosis
New lesions and recurrences are relatively common and are similarly treated. Potential contacts should be notified and examined for molluscum lesions.
Bacterial superinfection is possible with molluscum (Fig. 10.10B).
Viral Vesicular Eruptions: Herpes simplex and Herpes zoster
Pathogenesis and Etiology
Herpes simplex virus (HSV) type 1 usually causes facial infections (fever blisters, keratitis, and blepharoconjunctivitis), and type 2 affects the genitals. Primary HSV-1 infections typically occur in infancy or childhood, transmitted via saliva through skin or mucous membranes. They lie dormant in sensory nerve cells until activated by stress, infections, or ultraviolet exposure, causing progression along the axon with cutaneous or ocular surface lesions.26
Varicella zoster virus (VZV) causes chickenpox (varicella) as a primary infection, usually in unvaccinated children. Virus seeded to sensory nerve cells in the spinal cord may be reactivated, typically in older adults, resulting in shingles (herpes zoster).27
Ophthalmic involvement by shingles and herpes simplex results from the ophthalmic or maxillary divisions of the trigeminal nerve.28
Clinical Features
Herpes simplex presents as a vesicular eruption on lid margin or skin, often associated with a corneal dendritic ulcer (Fig. 10.11).24

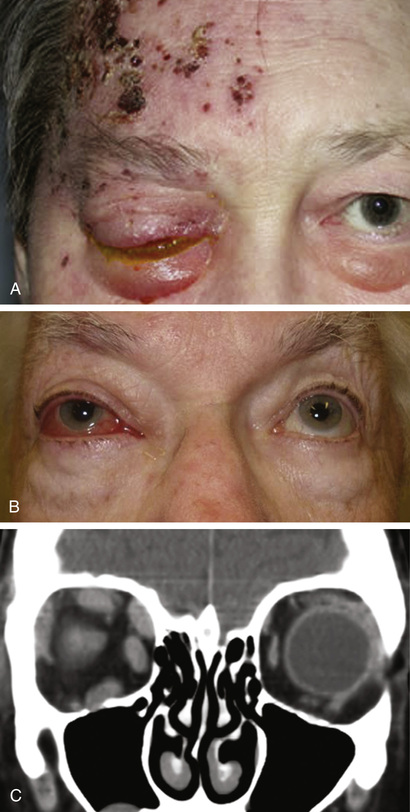
Herpes zoster presents with fever, malaise, and pain at one or more contiguous infected dermatomes. Within days, the painful skin becomes erythematous and progresses through blisters, pustules, and eventual crusting (Fig. 10.12A). Depending on affected nerve branches, inflammatory lesions may involve skin, conjunctiva, cornea (dendritic ulcer), aqueous and vitreous humor, retina, optic nerve, and orbit (myositis) (Fig. 10.12B and C). Lesions on the tip of the nose should raise suspicion of ocular involvement from the nasociliary nerve.27
Investigations
Polyester swabs of vesicular lesions or fragments of scabs may be shipped dry at room temperature for polymerase chain reaction (PCR) techniques to identify viral etiology.27
Management
H. simplex dermatitis may be treated with topical acyclovir, and keratitis and conjunctivitis are treated with topical and oral antiviral agents. For active infections, oral regimens include acyclovir, 200 mg five times daily for 10 days, or valacyclovir, 1 g twice daily for 10 days. Valacyclovir, 500 mg daily, may be given for prevention.
Periocular shingles are cleansed with bland antiseptic soaks and calamine lotion. Oral antiviral agents (acyclovir 800 mg five times daily for 7 days; valacyclovir 1 g three times daily for 7 days) given at onset of symptoms may shorten the duration. Postherpetic neuralgia may be treated with topical anesthetic gels and oral carbamazepine or gabapentin. Oral antibiotics (cephalexin or TMP-SMZ) are used to treat bacterial superinfections.27
Complications and Prognosis
Both infections may cause corneal or cutaneous scars and possible canalicular stenosis. Recurrences are common. Zoster may cause postherpetic neuralgia.
Preseptal Cellulitis
Pathogenesis and Etiology
Preseptal cellulitis is an infection of the soft tissues of the superficial eyelid anterior to the orbital septum that spreads readily beyond the margins of the orbital rim.
Portals of Entry.
Direct inoculation through skin occurs through insect bites, trauma, foreign bodies, and iatrogenic causes, including contaminated needles, piercings, and surgical incisions. Infection is more likely in inflamed, burned, or damaged skin.29
Spread may occur from contiguous infections, including hordeola, impetigo, canaliculitis, or dacryocystitis. Microorganisms may spread through the soft tissues of the cheeks, nose, or forehead from adjoining sinusitis or from teeth abscesses or dental procedures.29 Bacterial or viral conjunctivitis may develop preseptal cellulitis.30
Hematogenous spread from distant sites is less common, associated with systemic upper respiratory infections.
Pathogens.
S. aureus and various streptococcal species, including S. pneumonia and S. pyogenes, are most frequently identified. MRSA is increasingly prevalent in many regions.30 Pathogens associated with trauma include the Bacillus species (including Anthrax in South Asia and B. cereus worldwide)31 and fungi with organic foreign bodies. Anaerobic bacteria (Peptococcus, Peptostreptococcus, and Bacteroides species) must be considered with animal and human bites, with dental abscesses or dental procedures, and in cases with adult sinusitis.29,30
Hemophilus influenza type b (Hib) was the most common isolated organism in children less than 5 years old in preseptal cellulitis associated with respiratory infections or from eyelid trauma before the introduction of the Hib vaccine in 198532 but is now relatively rare.
Viral pathogens include Adenovirus (epidemic keratoconjunctivitis), H. simplex, and bacterial superinfections of Molluscum. Fungal pathogens include Aspergillus and Blastomyces.
Epidemiology
Preseptal cellulitis is most common in children under 10 years, with over half being younger than 5 years. Thereis an equal gender distribution. It occurs four times more often than orbital cellulitis. It is more common in winter months associated with upper respiratory infections (URIs).29,30
Clinical Features
Acute swelling, redness, and pain develop in the affected eyelid and may induce upper lid ptosis. Tearing, conjunctival injection, and blurred vision suggest an associated conjunctivitis or keratitis. Fever and malaise indicate hematogenous spread.
The patient may report preceding URI, sinusitis, dental procedure, insect bite, lid trauma or surgery, or contiguous infection. The area of maximal inflammation suggests the likely source.
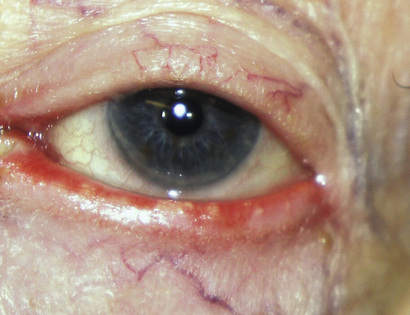
Preseptal cellulitis must be distinguished from deeper orbital infections. In the former, the zone of inflammation typically spreads beyond the orbital rim, whereas in orbital cellulitis it is demarcated by the insertion of the orbital septum at the tarsal plates and at the arcus marginalis. In preseptal cellulitis, there is no globe displacement, ocular restriction, or orbital hypertension (Fig. 10.13).

Necrotizing fasciitis (NecFasc) is a rapidly spreading bacterial infection causing extensive necrosis in subcutaneous tissues, commonly caused by Group A β-hemolytic streptococci, including S. pyogenes (NecFasc type II). Other implicated pathogens are S. aureus (including MRSA) and polymicrobial infections with anaerobes (NecFasc type I). Scarlet red blisters with subsequent necrosis or skin sloughing, rapid expansion of the involved area, and patient malaise with high fever suggest the diagnosis (Fig. 10.14). Early management, with combined expertise, broad spectrum antibiotics, and surgical debridement, is employed to avoid disfigurement, morbidity, or death.33

Investigations
Leukocyte counts are often elevated. Cultures of discharge from the conjunctiva, lid lesions, or canaliculus help define sensitivities. Fungal cultures may be sent for penetrating wounds and PCR obtained for viral identification in skin blisters or keratoconjunctivitis. Blood cultures may be drawn for suspected sinusitis or for cases with high fever or malaise, but only 10% are positive. Lumbar puncture should be considered in neonates to rule out meningitis from the Listeria, Neisseria, or Hemophilus species.
Orbital, sinus, and dental computed tomography (CT) scans are obtained to rule out orbital cellulitis in uncertain cases and identify sinus or odontogenic source.
Infected tissue is biopsied for culture and histology in suspected necrotizing fasciitis.
Management
Medications.
Treatment is with antibiotics, based on the likely source and the age of patient:
▪ Oral cephalexin: hordeola, impetigo, and penetrating injuries
▪ Oral clindamycin or TMP-SMZ: suspected MRSA
▪ Oral amoxicillin and clavulanate (Augmentin, Clavulin): lacrimal and sinus sources, animal bites, and dental disease
▪ Valacyclovir (Valtrex): for H. zoster
▪ Oral antifungals (fluconazole for candida and voriconazole for aspergillus): on recommendation of infectious disease
The patient is admitted to hospital to be given intravenous antibiotics (amoxicillin-clavulanate, if available, or piperacillin-tazobactam; or vancomycin with ceftriaxone or cefotaxime) for suspected bacteremia, neurologic signs, or necrotizing fasciitis.
Complications and Prognosis
Amblyopia should be considered in cases of severe preseptal cellulitis with ptosis in younger children.34 Residual ptosis or cutaneous scars may result from prolonged infections or trauma.29 Progression to orbital cellulitis carries risk of visual loss or mortality. Necrotizing fasciitis has a mortality rate of 20% if not recognized and managed promptly.33
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


