Table 24.2
Genetics of Vascular Malformations
| Malformation | Inheritance Pattern |
Capillary malformations (CMs) Port-wine stains | CMC1 locus on chromosome 5q 13–2219 |
Capillary malformation–arteriovenous malformation (CM-AVM) Parkes-Weber syndrome | RASA 1 mutation ( p120RasGAP protein)20 |
| Venous malformation (VM), cutaneomucosal venous malformation (VMCM) | Mutation in the tyrosine kinase receptor TIE2, also known as TEK on VMCM1 locus 9p2121 |
| Glomovenous malformation (GVM) | Autosomal dominant Ch. 1p 21–2222 |
| Lymphatic malformation: primary congenital lymphedema (Milroy disease or type 1 lymphedema) | Ch. 5q35.3 (mutation in VEGFR3)23 |
| Lymphatic malformation: late onset lymphedema (Meige disease or type 2 lymphedema) | Ch. 16q24.3 (missense mutation in the transcription factor FOXC2)24 |
| Hereditary hemorrhagic telangiectasia (HHT) | HHT1 Ch. 9q33–44, HHT2 Ch. 12q11–14, HHT3 Ch.5q, HHT4 Ch. 7p1425 |
| Cerebral cavernous malformation (CCM) | CCM1 Ch. 7q11–22 CCM2 Ch. 7p1326 |
| Klippel-Trenaunay-Weber syndrome | Mutation on chromosome 5q13.3 causes defective AGGF1 expression27 Translocations involving chromosomes 8,1428 |
Lymphatic Malformations
Epidemiology
LMs are benign vascular malformations with an international incidence of approximately 1 in 6000 to 1 in 16,000 live births.11 Sixty percent occur in the head and neck region; 35% of these affect the eyelids, conjunctiva, and orbit.12 They are slightly more common in females.13 Although most LMs are diagnosed by age 2 years, even those that present later in life are felt to be present from birth.1,14,15 LMs account for approximately 3% of all orbital masses16 and confer considerable risk of intracranial vascular malformations.17 Orbital LMs may be found in isolation or as part of more extensive, quadrantic, or hemifacial or cervicofacial LMs.18
Pathogenesis
LMs arise from the pluripotent venous anlagen, which may develop into both venous and lymphatic structures.8,9,14 The primary defect is believed to occur in lymph channels, rather than in nodes, and leads to lymphedema, with secondary dilation of lymph channels and mass formation.1 Another theory proposes that LMs arise from maldevelopment of the undifferentiated capillary network leading to a hemodynamically isolated infiltrative vascular malformation.8,29 Jakobiec and Font30 suggested that the germ of an LM is probably a vascular anlage that has been misdirected by unknown influences. This second theory is more widely accepted.
LMs consist of dilated, thin-walled vascular chambers lined with endothelium and supported by fibrous stroma. They contain a proteinaceous material reminiscent of lymph. They represent anomalous development of the lymphatic channels that occur during the weeks 6 to 7 of embryogenesis.28 For clinical purposes, these lesions are often discussed as one of three morphologic groups: macrocystic, microcystic, and combined. The subclassification is clinically useful because large cystic areas and small, spongiform areas respond differently to different treatment protocols (Fig. 24.2).

Isolated macrocystic LMs, also known as cystic hygromas, are amenable to surgical resection (Fig. 24.3). In contrast, microcystic LMs are infiltrative, with poorly defined borders, and typically cannot be surgically extirpated. They can present in both the superficial and the deep orbital spaces.

In addition to cystic hygroma, these lesions have been known in the literature as lymphangioma, lymphangioma circumscriptum, and lymphangiomatosis.31 Although the term “lymphangioma” has persisted particularly strongly in ophthalmology, the more accurate term “lymphatic malformation” is gaining rapid acceptance.
Differential Diagnosis
Generally, the differential diagnosis of vascular malformations includes hemangiomas and other vascular tumors (see Fig. 25.1). Specific differential diagnosis of LM includes rhabdomyosarcomas, metastatic neuroblastoma, venous malformation, AVM, solitary fibrous tumor (SFT), encephalocele, and mucocele.32,33
Clinical Features
LMs may be evident at birth but generally manifest in infancy or childhood (43% are diagnosed before age 6 years; 60% before age 16 years). The most common presenting complaints in orbital LM include ocular dysmotility, blepharoptosis, proptosis and related disfigurements, decreased vision, and pain. Pain is often associated with hemorrhage.32 LMs are unencapsulated, diffuse, and multicompartmental, often including both intraconal and extraconal components that are insinuated between normal orbital structures.14,16,29 They do not respect typical anatomic barriers such as the intermuscular septum orbital septum, or even the bony orbit (Fig. 24.4). They are usually unilateral, lobulated lesions with microcystic and macrocystic, components (defined as cystic spaces ≥2 cm3).34 Intraoral examination may reveal pathognomonic vesicles in the hard or soft palate.

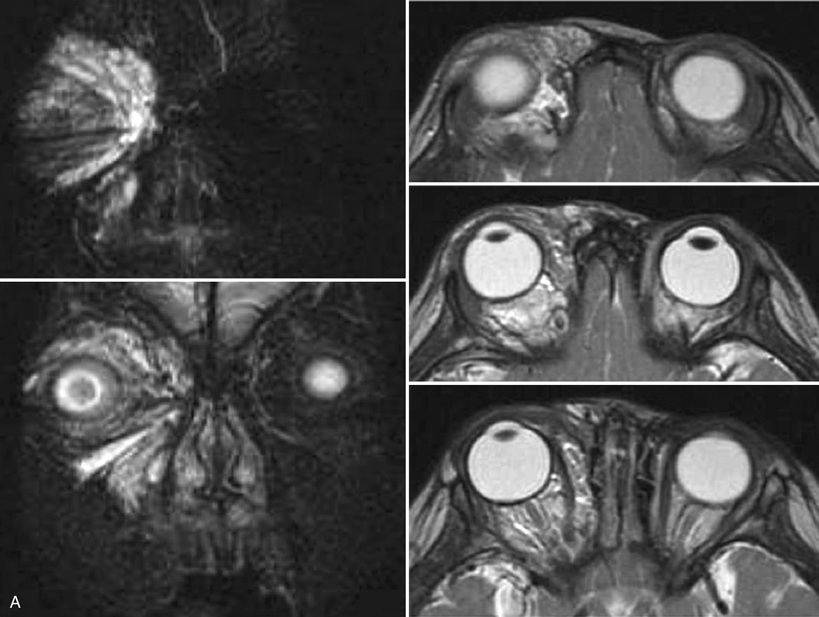
The fragile vessels in the intervening connective tissue septations may bleed within the cysts, best visualized on nuclear magnetic resonance imaging (MRI)35 (Fig. 24.5).

LMs enlarge during viral infections and shifts in hormonal milieu or may expand suddenly as a result of intralesional hemorrhage (spontaneously or after minor trauma).36 The hemorrhagic vessels are known as “chocolate cysts” because of the dark brown appearance on surgical exploration.37 Spontaneous intracystic hemorrhage produces ocular emergencies, with significant risk of permanent visual loss as a result of optic nerve stretching or compression15 (Fig. 24.6).

Like cavernous VMs, orbital LMs are isolated from the normal orbital vasculature. As such, they are not affected by postural changes and do not develop expansion, pain, or exophthalmos with inversion, as is typical for distensible venous lesions.14,35
Investigations
MRI is the imaging modality of choice for definition of soft tissue in the orbit. Fluid-fluid levels are seen as a result of recurrent hemorrhages within cysts, a feature considered pathognomonic. T2-weighted images typically are more revealing.31,32,35 Ultrasonography may identify internal septations and distinguish microcystic lesions from macrocystic lesions. Low-level internal echoes are usually demonstrated in cystic components, although an intracystic clot may be hyperechoic.14
Computed tomography (CT) demonstrates skeletal landmarks and identifies potential expansion of the bony orbit without bone destruction; it is less useful for distinguishing soft tissue components. These lesions typically occur in young children when the radiation exposure from CT is to be avoided.38
Pathology
Histopathology of LM shows delicate, irregular, bloodless, lymph-filled, attenuated endothelium-lined lymphatic cysts of various luminal diameters (from capillary to cavernous to cystic sizes), interrupted basement membrane, absence of pericytes, loose fibrous stroma, and few smooth muscle cells. Intervening connective tissue septa contain collections of lymphocytes and fragile blood vessels (neovascular tufts) that are believed to be sources of the hemorrhage.14,16,18
Lymphatic endothelial cells can be identified by D2-40, a selective monoclonal antibody directed against human podoplanin, a membrane glycoprotein of podocytes, expressed in the endothelium of lymphatic endothelium but not in the blood vasculature5,39,40 (Fig. 24.7).

Management
LMs grow relentlessly without involution. Treatment must consist of acute and long-term management.1 Multidisciplinary management, developed largely in the 1990s, has led to refined treatments and novel protocols. These include supportive homeopathic measures, systemic medications, endovascular therapies, percutaneous embolization, and traditional surgical approaches.1
Medical treatment is usually conservative, starting with observation. Corticosteroids are effective in temporizing flare-ups of inflammation. Children with recurrent upper respiratory infection should receive oral corticosteroids concurrent with oral antibiotics.18 Sirolimus has shown some promise in the treatment of extreme LMs but has not been used to treat isolated orbital disease. Simple drainage is usually temporary, with transudative reformation of the cyst. Drainage as part of a sclerotherapy protocol is more permanent. Surgical excision of complex LMs may be difficult.36
Because of difficult access, possible compromise of ophthalmic veins, postinterventional swelling, and risk of orbital compartment syndrome, the treatment of periorbital malformations is challenging.15 These lesions are routinely described as the most difficult of all orbital lesions to manage. Isolated macrocystic LMs are amenable to surgical resection or sclerotherapy, whereas microcystic LMs typically cannot be surgically extirpated. Recently, advances in sclerotherapy have shown promise even for microcystic LMs. Emergent treatment may be necessary in cases of rapid enlargement.1
Until recently, surgical excision was the primary treatment option. For conjunctival LMs, cryopreserved amniotic membrane has been successfully used to reconstruct conjunctival defects after excision of these lesions.41 Indications for surgical extirpation in orbital cases include compartment syndrome, optic neuropathy, proptosis, facial disfigurement, blepharoptosis, exposure keratopathy, amblyopia, strabismus, and astigmatism. The specific surgical intervention must be tailored according to location, chronicity, and severity. Surgical aspiration, although not a definitive treatment, can be effective in temporarily decompressing acute hemorrhage or a fluid-filled cyst, but rapid refilling in as little as 24 hours should be anticipated. Some surgeons prefer orbital decompression to excision, especially in cases of infiltrative, microcystic LMs. A theoretical advantage proposed by some is the possibility of inciting less inflammation in the immediate postoperative period with the possible benefit of years of relief. Others oppose decompression because of loss of anatomic barriers and the lifelong progression of the malformation. Anterior LMs with relatively large cysts may be accessed through a lid crease or conjunctival incision. These cysts may require surgical adjuncts such as thrombin or fibrinogen tissue adhesives. A transcranial orbitomy may be needed to access the posterior superior orbit.1
Although surgical approach is reasonably effective, high rates of recurrence and the risk of complications related to hemorrhage and induction of new blood cysts, as well as damage to surrounding structures and scarring, have provided the impetus to develop less-invasive approaches.42 Sclerotherapy involves the endovascular, percutaneous, or direct introduction of a chemical irritant into the lesion causing inflammation, scarring, and intralesional adhesions that obliterate the potential space within the cavitations.1 In the past few years, sclerotherapy has emerged as a promising alternative to the surgical management for LMs in children.18,42–45 Macrocystic LMs have shown the best response to this technique; some microcystic lesions were also amenable to sclerosant treatment.46,47
Although the popularity of sclerotherapy in the treatment of LMs is growing, no consensus exists with regard to the best sclerosants to use in any given clinical scenario. Ethanol, sodium tetradecyl sulfate, bleomycin, doxycycline, and OK-342 have all been employed in the treatment of head and neck vascular malformations, based on experiences with other sclerotherapy procedures and with varying but generally positive results.11,37,42,45 At least two individuals have suffered blinding orbital compartment syndrome after intraorbital injections of OK-432, and similar cases have been seen with alcohol injections. The current standard of care calls for fluoroscopic guidance for the introduction of orbital sclerosants. A microcatheter, angiocatheter, or needle is inserted into the lesion, allowing the introduction of contrast fluid. Once needle placement is confirmed, the sclerosant is introduced, sometimes mixed with contrast material.1 Nevertheless, the use of intralesional sclerotherapy for postseptal lesions must be approached carefully because of the risk of blindness from increased orbital pressure or direct chemical toxicity.1
Disease Course, Complications, and Prognosis
The natural history of LMs is as variable and unpredictable as the many forms they may take involving the orbit. Pan-facial and hemifacial lesions may be associated with orbital components, whereas other lesions may involve only the eyelid or conjunctiva in isolation (Fig. 24.8). Particularly in the orbit, danger arises mostly because of acute increase of size of the lesion after bleeding or upper respiratory infection. Other complications include intermittent swelling, blepharoptosis, amblyopia, chemosis, globe displacement, optic neuropathy, exposure keratopathy, astigmatism, and strabismus.14,37 Even without rapid enlargement, LMs may cause bone remodeling and produce skeletal hypertrophy, with protrusion of the zygoma and/or frontal bone. Gradual expansion often leads to progressive proptosis and slow decline in vision.1,14 Some cases may, however, show little progression, particularly when treated early and thoroughly. When a surgical approach is indicated, prognosis is excellent with complete resection.32

Reported complications of surgical resection of LMs include scarring, fibrosis, residual tumor, temporary or permanent ocular paresis, vision loss, and symptomatic recurrence. Even with such an intensive approach to resection, the recurrence rate is reported to be 40% after an incomplete excision and 17% after a macroscopically complete excision. Cutaneous wartlike lymphatic vesicles may develop within the scar but are easily treated by intravesicular sclerotherapy, cauterization, laser coagulation, or excision.18 Corticosteroid injections are routinely required as adjuncts to surgery.
Venous Malformations
Epidemiology
VMs are maldeveloped ectasias of the venous system that can be seen throughout the limbs, trunk, or head-and-neck region. In the orbit, they have been called “distensible venous malformations,” or “orbital varices.” These lesions will be referred to throughout this text as “venous malformations,” consistent with international and interspecialty nomenclature. A different lesion that is also of venous origin and commonly seen in the orbit is the so-called cavernous hemangioma. These will be referred to throughout this chapter by the more descriptive term, “cavernous venous malformation,” and will be described as a separate entity.
Venous malformations (excluding cavernous venous malformations) represent 2% of all orbital space-occupying lesions.48 Most VM cases are sporadic. However, mutations in the TIE2/TEK genes are associated with inherited forms of venous malformation.10 Whereas 40% of VMs occur in the head-and-neck region, the orbit and eyelids are rarely involved. Although they can present earlier, typically they manifest in the second or third decade of life. Females and males are affected with equal frequency.14,49
Pathogenesis
VMs are thought to result from abnormal influences during the late retiform plexus stage, the second vascular developmental phase when capillaries form between weeks 7 and 12.8 Orbital VMs presumably result from congenital weakness in the postcapillary venous wall, leading to the proliferation of venous elements and massive dilatation of the valveless orbital veins.49 Abnormal venous tangles can be seen, supporting the concept of true malformation rather than simple ectasia of pre-existing venous elements.8 These lesions are low-flow malformations that often drain to the cavernous sinus.
Differential Diagnosis
The differential diagnosis of orbital and periorbital VMs (usually presenting in childhood or adolescence) includes rhabdomyosarcoma, infantile hemangioma, LM, AVM, plexiform neurofibroma, SFT, and other vascular tumors.
Clinical Features
Venous malformations are characterized by weak, distensible segments of venous tissue that expand with raised intravenous pressure from inversion or Valsalva maneuver (Fig. 24.9). Clinical stability despite raised venous pressure should call the diagnosis into question. Although VMs change in size and color with increased pressure,8,14,35 some have only a small communication with the venous system and tend to manifest with internal hemorrhage and thrombosis and painful proptosis.49 Patients with collapsible orbital VMs manifest proptosis when exercising, but painful enophthalmos in the upright position at rest. It is not unusual to have greater than 10 mm excursion on Hertel exophthalmometry (Fig. 24.10). In other cases, the postural changes may be evident only on neuroimaging. Orbital VMs are commonly associated with contiguous or noncontiguous intracranial venous anomalies or ipsilateral hemifacial VMs that involve scalp, airway, buccal space, and masseter.14,50 In these cases, the diagnosis is more straightforward, with bluish discoloration of the involved eyelid, cheek, temple, scalp, or mouth (Fig. 24.11). Intraoral VMs can bleed, distort dentition, cause speech problems, and obstruct the upper airway and pharynx.51



Investigations
Investigations in patients suspected of VMs primarily involve imaging studies, although some serologic tests may be useful in specific circumstances. D-dimer, recently described as the first biomarker of VMs, may also help in the diagnosis, when high levels are observed.52
Ultrasonography may reveal an intermittent anechoic lesion with intrinsic flow during the Valsalva maneuver. However, as this imaging modality has a limited field of view and restricted penetration and is operator dependent, it is popular only in some institutions.53
Color Doppler imaging is important in differentiating VMs from other vascular anomalies and may demonstrate a reversal of flow toward the transducer during the maneuver. In most cases, Doppler ultrasonography demonstrates monophasic, low-velocity flow. In 20% of lesions, no flow is demonstrated, suggesting thrombosis.14,51,52
CT images obtained with the patient in the supine position usually show a normal appearance or only mild enlargement of the involved veins. In young children, the radiation associated with CT should be avoided.38 Distensibility and extension of VMs can be seen on CT, but not as clearly as in MRI, where soft tissue detail and contrast resolution are superior. On CT, VMs are hypoattenuating or heterogeneous lesions that enhance slowly and peripherally after a bolus injection of contrast, may be smooth contoured, clublike, triangular, or segmentally dilated, or they may appear as a tangled mass of vessels. Phleboliths, commonly seen on CT scans, are considered pathognomonic1,14,51 (Fig. 24.12).

Although MRI is the imaging modality of choice, VMs may appear or disappear on MRI scans, depending on patient position and venous pressure. The study should be requested with raised venous pressure and with contrast. MRI scans without the Valsalva maneuver may conceal the lesion entirely. Prone positioning is more likely to reveal an orbital or facial VM, as it is positioned dependently. VMs show hypointense to hyperintense signals on T1-weighted images and hyperintense signals on T2-weighted images and usually enhance intensely after the administration of contrast material.14
Pathology
VMs are composed of small and large dysplastic, postcapillary, thin-walled and dilated spongelike vascular channels varying in size from capillary to cavernous dimensions, with sparse smooth muscle, adventitial fibrosis, and variable amounts of hamartomatous stroma, thrombi, and phleboliths. The dysplastic venous channels usually connect with adjacent physiologic veins via narrow tributaries. Smooth muscle actin (SMA) staining reveals muscle in clumps instead of the normal smooth muscle architecture. A mural muscular anomaly is probably responsible for the gradual expansion of these lesions.54
Management
VMs are chronic, progressive lesions requiring long-term and often multidisciplinary management.1 Current options include systemic, local, and regional medications, endovascular embolization, percutaneous sclerotherapy, and surgical extirpation.1
Medically, low-dose aspirin and/or anti-inflammatory medications are used for pain or if compression is not anatomically possible, as in the head-and-neck region. When associated with elevated D-dimer levels, pain can be relieved with low-molecular-weight heparin 100 AntiXa/kg/day for 20 days, or longer if the pain returns.52 Low doses of aspirin seem to minimize phlebothromboses. Preoperative control of intravascular coagulopathy with heparin should be considered before the resection of large VMs.51
Indications for treatment of orbital venous malformations include pain, disfigurement, and dysfunction. With purely periocular lesions, eyelid swelling and pain, conjunctival engorgement, and intermittent enophthalmos and exophthalmos tend to require intervention. Facial lesions can induce a facial paralysis-like picture with hemifacial ptosis and loss of expression and orbicularis oris function (Fig. 24.13). In general, distensible lesions may be amenable to a variety of techniques, including Nd : YAG laser ablation, percutaneous sclerotherapy, and surgical excision.8,14 A common combined protocol might involve laser treatment to oral and ocular mucosal surfaces, and percutaneous sclerotherapy followed by surgical excision in 24 hours.55

The unpretreated surgical excision of VMs is difficult because the tortuous, fragile, vessels tend to rupture during surgery. Intralesional thrombotics and retrograde venous catheterization with embolization have been helpful to reduce intraoperative bleeding.8 Intralesional injection with cyanoacrylate, fibrin, gelatin, or noxious sclerosants have all been reported to have good success, but outflow to the cavernous sinus should be monitored with intraoperative venography8 (Fig. 24.14).

In the orbit, painful enophthalmos and exophthalmos, thrombosis, and deformity may demand intervention. In general, orbital VM are amenable to carbon dioxide laser ablation, percutaneous sclerotherapy, and embolization–resection protocols.8,14 Periocular VMs can also be treated with Nd : YAG and other lasers.
Disease Course, Complications, and Prognosis
The natural history of VMs is relentless, unpredictable enlargement. Troubling complications include orbital compartment syndrome and progressive pain from worsening enophthalmos-exophthalmos cycles. Patients with very large distensible malformations may become enophthalmic because of the gradual enlargement of the bony orbit and associated fat atrophy over time.36 Other complications include intermittent swelling, blepharoptosis, amblyopia, chemosis, globe displacement, optic neuropathy, exposure keratopathy, astigmatism, and strabismus.1,14,35,37
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


