Infant, Toddler, and Children’s Visual Acuity—Practical Aspects
Robert H. Duckman
Visual acuity is a clinical test that gives the clinician insights into the child’s visual status. It is usually a reflection of the individual’s visual function (i.e., if the acuity is normal or better, it can almost always be inferred that the patient is doing well visually). When the visual acuity is decreased, it alerts the clinician to the likelihood that some anomalous condition (e.g., pathology, refractive error, or binocular problems) is present. Of course, it is possible to have normal acuity and still have a serious problem with the eyes. Visual acuity, therefore, is only one clinical finding that can aid the clinician’s strategy in the examination. Visual acuity helps in decision-making and therapy choices. When the visual acuity is lower than expected, the clinician spends much of the examination attempting to find the reason acuity is down and then trying to bring it up to expected levels. This is an important part of a vision examination whether examining an adult or a child. The difficulty lies in the fact that obtaining a visual acuity measure on a young child (birth to 5 or 6 years of age) is much more challenging than obtaining a visual acuity measure on older patients. In the early 1960s, few real ways existed to accurately quantify visual acuity in preverbal children. About the only clinical tool was the optokinetic drum. It provided some information about visual function, but nothing that was quantifiable or that could be used to gauge improvement in tracking acuity in an amblyopic eye. Now, we know that optokinetic nystagmus (OKN) (Chapter 2) is mediated subcortically and provides little to no information about cortical visual function.
As we saw earlier (Chapter 2), visual acuity in the infant or toddler patient is not equal to an adult’s acuity. This can be reconciled by the immature development of the macula and the visual cortex, and the incomplete myelinization of the visual pathways (Chapter 1). As the visual system matures, visual acuity improves and approaches the adult’s level. The point at which the child’s visual acuity responses reach adult levels depends on many things. The primary and most important factor, however, is the measurement tool used to quantify acuity. Different tools produce significantly different results in the measurement of acuity in children.
Visual acuity can be a critical clinical finding in children. The young child, with or without specific and as yet unidentified visual anomalies (e.g., anisometropia or strabismus), often develops amblyopia. If amblyopia is identified sufficiently early, treatment is usually prescribed. Without a reliable visual acuity measurement each time the child comes in, it is difficult to tell whether treatment is effecting change, if it is effective, and if it should be continued.
Until the 1970s, little could be done to measure acuity in preverbal children. Part of the reason for this is that up to that time, it was generally believed that infants, toddlers, and preschoolers did not have normal function and that adult function was not possible before age 5 years. Most practitioners told their patients with
children that they should wait until the child was 5 years of age to have a visual examination. As the understanding of the development of the visual system became clearer through the efforts of psychophysicists and vision researchers in the 1970s and onward, it became clear that the visual system of the young child was much more sophisticated than people had been willing to admit. It also became clear that when a visual problem existed, it responded better to therapy (e.g., patching) the earlier it was applied. We know today that early rather than late intervention offers greater promise to the restoration of normal visual function of an eye with a functional problem.
children that they should wait until the child was 5 years of age to have a visual examination. As the understanding of the development of the visual system became clearer through the efforts of psychophysicists and vision researchers in the 1970s and onward, it became clear that the visual system of the young child was much more sophisticated than people had been willing to admit. It also became clear that when a visual problem existed, it responded better to therapy (e.g., patching) the earlier it was applied. We know today that early rather than late intervention offers greater promise to the restoration of normal visual function of an eye with a functional problem.
It is our responsibility, therefore, to encourage parents to bring children in for eye examinations as early as possible and to identify and treat problems that could cause eventual loss of visual function (e.g., amblyopia in refractive anisometropia). In many cases of anisometropia, rarely are signs or symptoms seen of a visual problem. The parent assumes the child can see normally. When the child enters school and has a vision examination, however, a very significant difference is seen in acuity between the two eyes. By this time, the child may be 5 or 6 years of age and has 20/20 in one eye and 20/400 in the other eye. It is not too late to apply patching therapy at this point and improve acuity, but it will be more difficult and have a more guarded prognosis. One reason is age; another significant reason is that it is difficult for a school child to wear a patch in class. The child receives a lot of ridicule and become the brunt of a lot of teasing. So had the child in this example been tested at 6 months, it would have been easier to patch and to improve the visual acuity in the eye with the greater refractive error. It is not impossible to take the child described above and achieve improvement later on, but it will be more difficult and improvement will be slower. The child with anisometropia that is not corrected with lenses or not given a patching regimen can eventually sustain irreversible loss of visual function.
As mentioned in Chapter 2, the best acuity measurement is a recognition acuity. Obviously, an infant or toddler cannot sit and read letters, pictures, or numbers from an eye chart. Therefore, it is not possible to get a recognition acuity on these patients. Using electrophysiologic or behavioral techniques, however, the clinician may be able to obtain a threshold minimum separable acuity. This, therefore, is the best we can do with children who are very young or who cannot respond verbally or motorically, as in a matching task. These techniques, however, are certainly sufficiently sensitive to measure improvement in an amblyopic eye or ascertain the difference in acuity with the application of lenses in a child with refractive error. Because acuity age norms have been established for visually evoked potentials (VEP) (see Chapter 2) and forced-choice preferential looking (FPL) (see Chapter 2), it is possible, on repeated measures, to determine if the child’s visual development is proceeding in a normal pattern.
What is the difference between VEP measurement and FPL? As mentioned in Chapter 2, VEP has advantages and disadvantages when compared with FPL. VEP is faster and, therefore, more reliable. The main factor in dealing with very young children is maintaining their interest in the task. Because the VEP acuity test requires less time, especially if a sweep VEP is used, it is more likely that the child will be able to attend for the duration of the test. FPL techniques take significantly longer to do and, therefore, may become less reliable as attention wanes with continued presentations. As an aside, I find that many young patients respond robustly to the FPL cards and then suddenly, as if deciding “this is enough,” they no longer attend. When there is no clear decrease in responsiveness, but rather only an all or nothing type of response, I refer to these acuity values as “minimal visual acuity” and not threshold visual acuity. The VEP measures the electrophysiologic response of patterns of light into the eye and up to the level of the visual cortex. This test, therefore, can provide valuable information about the intactness of the visual system from the eye to the visual cortex, but it says nothing about visual processing beyond the cortex. It gives no information about what the individual child is actually seeing—just the limits of the child’s potential to see. The biggest disadvantage of the VEP procedure is that the instrumentation is very expensive and if the practitioner does not need to do a lot of these procedures, it is unlikely to find its way into the practice.
The advantages of the FPL procedure are (a) it is the clearest indication of what the patient can actually see of any of the techniques available; (b) the spatial frequencies available cover a very wide range of minimum separable visual acuity values (20/2400 to 20/10); and (c) it is easier to administer and is portable so it can easily be moved around. Of course, disadvantages are seen as well. The most significant one is the extended period of time it takes to administer. No matter how streamlined the task is made, it is extremely difficult to get three measurements (OD, OS, OU) in a single testing session. Infants may like stripes, but not that much. My preference is to test acuity first because it probably demands the greatest attention. If no reason exists to suspect that one eye is seeing less well than the other (e.g., in constant right esotropia, concern would exist that the right eye is seeing less well than the left and a monocular right eye acuity test would be done first) and with no historical information suggesting an interocular difference in acuity, then I would first measure binocular acuity. Children having this procedure often get extremely upset when a patch is placed on their eye. If they do get upset, the child may not ever continue. If you start with a binocular visual acuity test, however, you will very likely get a visual acuity value. This will allow you to assess whether the acuity development is normal for the child’s age. At this point, if you wish, you can attempt monocular acuity measurements. I prefer to let the monocular measurements “sit until needed.” If, on the other hand, the child comes in with a constant right esotropia present since 3 months of age, my biggest concern is to get the monocular right eye acuity. In this case, I will put the patch on the left eye and proceed with the Teller acuity cards (TAC). This may likely upset the child, but, in this case, it is essential to find out what the acuity in the right eye is to determine how to manage the child’s care. A binocular acuity value in this case tells nothing about the deprived right eye. So, if no reason is seen to suspect a difference in acuity between the eyes, start with a binocular condition. When there is concern about an interocular acuity difference, do the deprived eye first. When the binocular acuity is normal for the child’s age, continue with the rest of the examination. If during the examination, you uncover an amblyogenic factor (e.g., refraction = OD -7.00 Sph OS Plano) that was not obvious before the examination, it becomes urgently important to go back and measure the visual acuity in the deprived eye (in this case, the right eye). In measuring the deprived eye acuity, the refractive correction should be applied in a trial frame. (By far the best infant, toddler, and even pediatric trial frame that I have come across is the product Solo Bambini by Occhialino di Prova seen in Fig. 10.1.
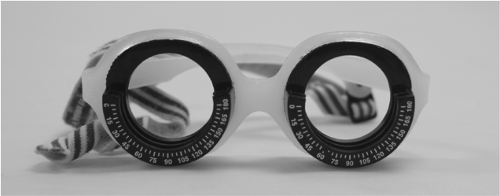 Figure 10.1. The Solo Bambini Baby 2 Trial Frame by Occhialino di Prova. |
If the child objects to the patching and becomes behaviorally difficult, set up another appointment to measure the right eye acuity. It is a good idea to have the child wear a patch for 5 to 10 minutes at home each day on the non- deprived eye until the next visit. This to accustom the youngster to experiencing the patch in a “safe” environment. Testing is best done about
30 minutes after feeding or napping. The worst time to attempt to examine an infant or toddler is while they would normally be napping or when they are hungry. Appointments should be made accordingly. On the return visit, first attempt quantification of the visual acuity of the deprived eye. Once this is done in conjunction with the previous findings, a treatment plan can be formulated. For the kind of lenses to prescribe, see Chapter 20.
30 minutes after feeding or napping. The worst time to attempt to examine an infant or toddler is while they would normally be napping or when they are hungry. Appointments should be made accordingly. On the return visit, first attempt quantification of the visual acuity of the deprived eye. Once this is done in conjunction with the previous findings, a treatment plan can be formulated. For the kind of lenses to prescribe, see Chapter 20.
It is important when testing FPL to use the most expedient methodology so that it takes the least amount of time. My preference is to use a modified “staircase” presentation. In this procedure, the spatial frequencies are presented from lowest to highest cycles per degree (cpd). Rather than starting from the lowest spatial frequency, however, I start at the expected acuity card diagnostic stripe width for the child’s age, then present higher and higher spatial frequency cards until reaching threshold or losing attention. Of course, if the child cannot perform at the age-appropriate diagnostic stripe width, decrease spatial frequency until a response is elicited.
Another methodology referred to as diagnostic stripe width (DSW) is available (see Chapter 2). As an example, if the child is 6 months of age, the DSW is equal to minimum separable acuity of 20/100 (ca. 6.5 cpd). The clinician would then show the child the card corresponding to 6.5 cpd at the utilized test distance ten or more times. If the child correctly looks to the stripes 70% of the time or greater, the child has developed to the expected acuity for that child’s age. This is not necessarily a threshold acuity value and a statement cannot be made about the child’s best possible visual acuity. What can be said, however, and in a relatively short period of time, is that this child’s visual acuity development is normal (1,2). (If the child cannot demonstrate DSW, it would be in everyone’s best interest to find out what the child’s visual acuity threshold is and why.)
FPL using TAC or any other type of presentation takes a degree of practice to get comfortable with the technique. It is very easy to make the observations about the patient’s fixations when you are well above threshold. As the clinician approaches threshold acuity, however, the observations become increasingly more difficult to make. Judgments about which side the stimulus is on in the FPL procedure should be made on the basis of
First fixation
Relative interest in the stimulus
How much time the child fixates one side over the other
Judgments should be practiced to take into consideration all possible subtleties. Understand, the child has a 50/50 chance of looking to the correct side. When the child does fixate to the right or left side, however, make sure the child is fixating the stimulus and not, for example, part of a hand that is holding the card or a toy off to the side of the stimulus presentation. Again, these observations are easy to make when you are well above threshold, but become increasingly more difficult as you reach the child’s visual acuity threshold.
Teller Visual Acuity Cards
Teller acuity cards (TAC) (Fig. 10.2) are recommended to test visual acuity in infants from birth to approximately 1 year of age. The cards and the procedure “top out” at about 12 months because, by this point in development, children are too fascinated with the world around them to be enamored with spatial frequency gratings. It therefore becomes necessary to look for other instruments to measure visual acuity. This is an extremely important time for the infant in terms of visual development, because it is a time when abnormal visual experience can have a very large impact on normal visual development. If, for example, the child has an amblyopic eye and therapy is being applied (e.g., patching), make sure the visual acuity is improving over time. A reliable tool is needed with which to measure visual acuity across time. If acuity is measured in
an amblyopic eye when the infant is 6 months of age and is shown to be below normal while the partner eye is normal, you may want to initiate a patching regimen. Recheck the child and monitor acuity 1 to 2 months later. At the recheck visit, if visual acuity has improved, but is still below the paired opposite eye, continue with the patching regimen. Continue this for several more visits, until the child is 16 months old. Although all earlier measurements were done with TAC, the child will now no longer attend to them. The child’s acuity, on whatever instrument you now use to measure acuity, cannot be equated to the acuity measurements obtained with the FPL procedure. Monocular acuities can be taken with a new visual acuity procedure and by comparing the previously normal eye with the previously amblyopic eye. One cannot say that the amblyopic eye has changed when comparing one measurement procedure with the other.
an amblyopic eye when the infant is 6 months of age and is shown to be below normal while the partner eye is normal, you may want to initiate a patching regimen. Recheck the child and monitor acuity 1 to 2 months later. At the recheck visit, if visual acuity has improved, but is still below the paired opposite eye, continue with the patching regimen. Continue this for several more visits, until the child is 16 months old. Although all earlier measurements were done with TAC, the child will now no longer attend to them. The child’s acuity, on whatever instrument you now use to measure acuity, cannot be equated to the acuity measurements obtained with the FPL procedure. Monocular acuities can be taken with a new visual acuity procedure and by comparing the previously normal eye with the previously amblyopic eye. One cannot say that the amblyopic eye has changed when comparing one measurement procedure with the other.
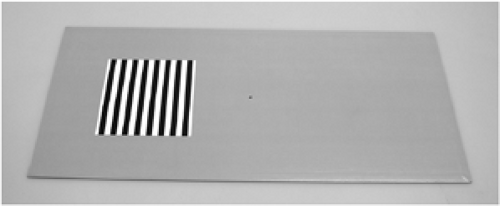 Figure 10.2. Teller acuity cards (Precision Vision). |
As mentioned, the TAC produce their best results when used on a population of normal infants from birth to approximately 1 year of age. It has also been used on children with developmental disabilities. Duckman and Selenow (3) found that this procedure could be used very effectively, almost without limitation on age, on neurologically impaired children. Jacobsen et al. (4) found that when the TAC were used to measure acuity of mentally retarded children, they were effective and there was good test–retest reliability.
In the ancient history of visual development research (1980), FPL was “born.” Initially, the targets were very difficult to make because the presentations were made by rear-projecting spatial frequency slides against high optical transmission material such as Polacoat. The striped slide projections were matched for mean luminance with the gray slides. At the end of the procedure, therefore, a spatial visual acuity (minimum separable) would have been obtained. The last spatial frequency the infant was able to achieve, at the criterion level of 75%, becomes the visual acuity threshold for the FPL procedure. Later in the decade, Vistech Corporation, with Davida Teller, achieved a set of cards, commercially produced, which had the background gray of the card match the mean luminance of the stimulus’ spatial frequency. These cards are now considered an important clinical tool utilized throughout the country and the world. The cards have recently been plasticized, have slightly lower contrast, and need to be recalibrated. The overall utility of the cards, however, is sound and reliable. Although TAC are useful for infants from birth to about 12 months of age, age range can be extended if the child understands the instructional set “look at or point to the lines.” Sometimes it is very important to get a visual acuity on a child because of expected or known amblyopia. If the child cannot respond to looking at or pointing to the stripes, it is reasonable to attempt a conditioned FPL paradigm. In this procedure, the child is conditioned, through positive reinforcement schedules, to look at or point to the stripes. It is difficult to do, but if it works, a threshold visual acuity can be obtained on the amblyopic and nondeprived eye. By the time the child is about 2.5 years of age, it should be possible to capture recognition acuities on one of the available charts.
Forced-choice Preferential Looking Paddle Acuity
Teller acuity cards are a reliable clinical tool that is used both in clinical and laboratory settings. The TAC, however, are relatively expensive (approximately $3000) and clinicians often find it difficult to justify spending that much money on the occasional infant they see in their practices. Therefore, “budget” versions of FPL acuity testing have emerged in the form of spatial frequency paddles (approximately $200).
Several companies produce these paddles (Fig. 10.3




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
