Development of Accommodation in Human Infants
Mark Rosenfield
Ocular accommodation is the process whereby changes in the refractive power of the crystalline lens allow clear vision to be maintained across a range of viewing distances. Contraction of the ciliary muscle pulls the choroid forward and the attachment of the zonules inward, thereby relaxing the tension of the zonular fibers. This allows the crystalline lens to become more convex because of both the elastic forces in the lens capsule and the viscoelastic properties of the lens substance (1,2,3).
An infant needs to be able to accommodate accurately to resolve objects at a close viewing distance. With the exception of a few infants having uncorrected myopia (4,5,6,7,8), they will have poor near visual resolution without adequate accommodation. This is critical for normal visual development to proceed, because it depends on the brain receiving clear and focused images from each of the two eyes (9).
The earliest evidence for active accommodation in human infants comes from studies that have observed differences in refractive error when measured both with and without the use of pharmaceutical cycloplegic agents to paralyze active accommodation. For example, analysis by Howland (8) of the data presented by Santonastaso (10) indicated that for 19 infants under 15 days of age, the mean spherical refractive error measured with and without cycloplegia was +0.98 D and -7.03 D, respectively. Earlier, Jaeger (11) used the direct ophthalmoscope to determine the refractive error of 100 infants between 9 and 16 days of age without cycloplegia, and reported that 78% were myopic. It should be noted that the direct ophthalmoscope is generally regarded as an inaccurate instrument for assessing refractive error (12,13). Nevertheless, most studies that have measured refractive error under cycloplegia have observed a much lower prevalence of myopia. For example, Cook and Glasscock (4) using cycloplegic retinoscopy on 1000 eyes of children during “postdelivery care” found that approximately 25% were myopic. Similar levels of myopia prevalence in infants (N = 356) using atropine cycloplegia were reported by Goldschmidt (5). Furthermore, a significant difference was observed in the refractive error of 2-day old infants when assessed with and without cycloplegia (14). It was concluded that these differences provided evidence of active accommodation in the newborn infant.
Having demonstrated that newborns do indeed possess the ability to accommodate, subsequent studies have examined the accommodative response to a range of stimulus demands in young infants. This assessment of the accommodative stimulus-response profile is commonly carried out in adults, and a typical adult accommodative stimulus-response function is illustrated in Fig. 6.1 (1,15,16).
One of the first studies to examine this function in infants was carried out by Haynes et al. (14). Here, dynamic retinoscopy was used to measure the accommodative response of
22 normal infants ranging from 6 days to 4 months of age. The fixation target was composed of a white card, which was mounted on the retinoscope, and contained a red annulus with an outside diameter of 3.8 cm. Black marks and dots were printed randomly within the red area.
22 normal infants ranging from 6 days to 4 months of age. The fixation target was composed of a white card, which was mounted on the retinoscope, and contained a red annulus with an outside diameter of 3.8 cm. Black marks and dots were printed randomly within the red area.
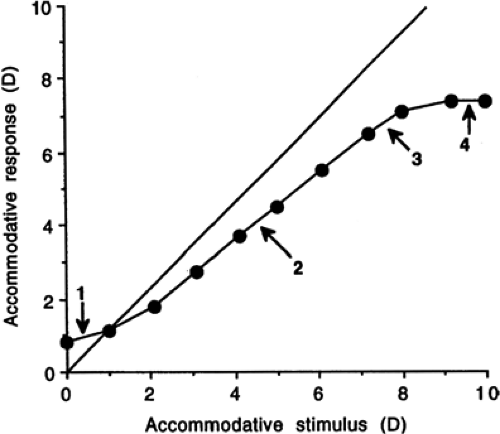 Figure 6.1 Static accommodative stimulus-response curve for a normal adult subject. 1, initial nonlinear region; 2, linear region; 3, transitional soft saturation region; 4, hard saturation region. The diagonal line represents the unit ratio (or 1:1) line. (Redrawn from Ciuffreda KJ, Kenyon RV. Accommodative vergence and accommodation in normals, amblyopes and strabismics. In: Schor CM, Ciuffreda KJ, eds. Vergence Eye Movements: Basic and Clinical Aspects. Boston, Butterworths, 1983;101–173. ) |
Haynes et al. (14) reported that before 1 month of age, accommodation appeared to be locked at a single focal distance having a median value of 19 cm (5.3 D). The flexibility of the response improved with increasing age, however, so that adult-like responses were achieved by 4 months of age. Further, to demonstrate that the infants were indeed capable of accommodating, the refractive state was measured in 11 infants when they were sleeping, and compared with the findings for the same children when they were awake and alert. The authors reported that the refractive state varied by an average of 5 D under these two conditions.
In reevaluating the data presented by Haynes et al. for the nine infants who were less than 1 month of age, it is apparent that almost all of these subjects showed poor responsivity to the changing stimulus (i.e., maintained a relatively stable response). A wide range of accommodative response levels was observed, ranging from approximately 3.5 D to 8.75 D. Accordingly, the often-quoted statement based on this study that the accommodation of newborn infants is fixed at a value around 5 D is unjustified. Rather, it would be more accurate to state that a very wide range of accommodative responses was observed, but little change in accommodation resulted from alteration of the target distance.
An extensive series of investigations by Banks (17) also used dynamic retinoscopy to examine accommodative stimulus-response profiles in infants between 1 and 3 months of age. In the first experiment, accommodation was measured in 20 infants longitudinally at weekly intervals from 1 week up to at least 2 months of age. Three stimulus values were tested, namely 1.00, 2.00, and 4.00 D. Summary data are shown in Fig. 6.2, and longitudinal data for a single subject is illustrated in Fig. 6.3. Banks noted three changes with increasing age, namely (a) an increase in the gradient of the stimulus-response function, (b) a decrease in variability within each age group, and (c) a decline in the mean accommodative error (i.e., the difference between the accommodative stimulus and response). In comparing his findings with those of Haynes et al., Banks noted that the mean gradients of the stimulus-response function observed in his study for infants 1, 2, and 3 months old were 0.51, 0.75, and 0.83 D/D, respectively. In comparison, for similar aged children, Haynes et al. observed mean gradients of 0.06, 0.50, and 0.76 D/D, respectively.
To explain the discrepancy between his findings and those of Haynes et al., particularly in the children under 1 month of age, Banks suggested that the form and size of the target adopted by Haynes et al. might have represented a poor accommodative stimulus in such young children. The angular subtense of the annulus would have varied from 23° at a viewing distance of 10 cm to 2° at a viewing distance of 100 cm. Thus, the “black marks and dots,” which were printed randomly on the target, probably subtended less than 15 minutes of arc at the furthest viewing distance. Although
estimates of unaided visual acuity in newborn infants vary widely depending on the method of assessment (18), a value between 20/400 and 20/800 (19,20) would correspond to a minimum angle of resolution between 20 and 40 minutes of arc. Accordingly, much of the detail present in the target used by Haynes et al. is likely to have been too small for the subjects to be able to resolve, thereby explaining why little change in accommodation was observed in the youngest subjects, with the accommodative response appearing to be “locked” at a single response value.
estimates of unaided visual acuity in newborn infants vary widely depending on the method of assessment (18), a value between 20/400 and 20/800 (19,20) would correspond to a minimum angle of resolution between 20 and 40 minutes of arc. Accordingly, much of the detail present in the target used by Haynes et al. is likely to have been too small for the subjects to be able to resolve, thereby explaining why little change in accommodation was observed in the youngest subjects, with the accommodative response appearing to be “locked” at a single response value.
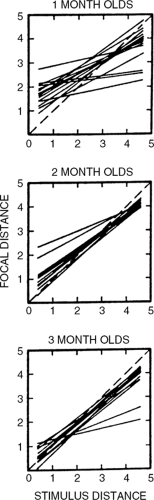 Figure 6.2 Accommodation stimulus-response function for 14 infants at 1, 2, and 3 months of age. Focal distance (plotted in diopters) refers to the distance at which the eye is focused, and reflects the accommodative response. Best-fitting lines were calculated from the responses of each infant. The diagonal dashed line represents the unit ratio (or 1:1) line. (From: Banks MS. The development of visual accommodation during early infancy. Child Dev 1980;51:646–666 , with permission.) |
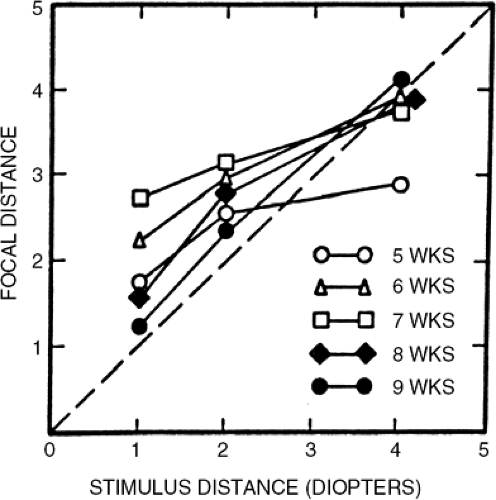 Figure 6.3 Accommodation stimulus-response function measured on a longitudinal basis for a single infant between 5 and 9 weeks of age. Focal distance (plotted in diopters) refers to the distance at which the eye is focused, and reflects the accommodative response. The diagonal dashed line represents the unit ratio (or 1:1) line. (From Banks MS. The development of visual accommodation during early infancy. Child Dev 1980;51:646–666 , with permission.) |
Additionally, results from the measurement of visual resolution at different viewing distances in infants may also support the proposal that these individuals have the ability to vary their accommodative response. For example, Salapatek et al. (21) used a preferential looking procedure to determine the visual acuity threshold to square wave gratings in 33 full-term infants varying from 24 to 63 days of age. Gratings were presented at distances of 30 cm and 150 cm for all subjects, and some subjects were also tested at 60 cm and 90 cm viewing distances. The authors reported that acuity thresholds were “relatively constant” regardless of the viewing distance. Similar findings were observed by Atkinson et al. (22), who compared visual acuity at distances of 30 cm and 60 cm in infants as young as 5 weeks of age, and found
equivalent results at the two viewing distances. If the infants lacked the ability to alter their accommodative response, then one would have predicted a significant decline in visual acuity when the position of the target was altered, provided the change in stimulus exceeded the depth-of-field of the eye. As will be noted in a later section of this chapter, the depth-of-field [which can be defined as the range of object distances within which the visual acuity does not deteriorate (23), and is dioptrically equivalent to the depth-of-focus] tends to be large in young infants. These findings, therefore, do not conclusively demonstrate a change in accommodation.
equivalent results at the two viewing distances. If the infants lacked the ability to alter their accommodative response, then one would have predicted a significant decline in visual acuity when the position of the target was altered, provided the change in stimulus exceeded the depth-of-field of the eye. As will be noted in a later section of this chapter, the depth-of-field [which can be defined as the range of object distances within which the visual acuity does not deteriorate (23), and is dioptrically equivalent to the depth-of-focus] tends to be large in young infants. These findings, therefore, do not conclusively demonstrate a change in accommodation.
In an alternative procedure to dynamic retinoscopy, other investigators have used objective photorefraction to assess the refractive state of an accommodating subject. Early studies (24,25) used orthogonal photorefraction to assess accommodation in infants. Here, a fiber-optic bundle delivers a point of light to the center of a 35 mm camera lens, and a photograph is obtained after refraction at the eye through an array of four 1.50 D cylindrical lenses that surround the fiber-optic bundle. The cylindrical lenses produce a star pattern, with the length of the cross arms being proportional to the refractive power of the respective meridian. Although this technique measures the magnitude of defocus, it does not indicate its sign (i.e., whether it is myopic or hyperopic). An alternative procedure, eccentric photorefraction, where the light source is not centered in the camera aperture, can be used to determine both the magnitude and sign of the refractive error.
Braddick et al. (25) used orthogonal photorefraction to examine accommodative responsivity in infants as young as 1 day old. Targets were presented at viewing distances of 1.5 m and 0.75 m. For an emmetropic observer, these correspond to accommodative stimuli of 0.67 and 1.33 D, respectively. The camera operator, serving as the visual target, attracted the infant’s attention by shaking colored rattles or playing an attention-seeking game such as peek-a-boo. For the 0.75-m viewing distance, the eye was considered “in-focus” if the point conjugate with the retina lay within a range of 1.2 D in front of the camera (i.e., was focused between 1.3 and 2.5 D). At the 1.5-m viewing distance, the in-focus range was considered to fall between 0.37 and 1.27 D. The size of these in-focus zones was determined by the region within which the observed reflexes were vignetted by the fiber-optic head. For the 0.75-m target, Braddick et al. reported that approximately 50% of the infants 1 to 9 days of age were consistently in-focus at the distance, rising to a level of greater than 80% at 2 to 3 months of age. Even in the infants 1 to 9 days of age, approximately 85% were considered in-focus for this relatively distant target on at least one of the three or four occasions when accommodation was measured. For the more distant 1.5-m target, however, none of the infants 1 to 9 days of age was found to be in-focus consistently, although between 10% and 40% were “inconsistently” focused at this distance. By 2 to 3 months of age, approximately 85% and 60% of the subjects were consistently in focus at the 0.75- and 1.5-m distances, respectively, which rose to 100% for both distances at 6 to 8 months of age.
A subsequent study by Dobson et al. (26) also used photorefraction to measure the accommodative response of infants 3 month of age. Here, the target was composed of either a horizontally or vertically oriented square-wave grating [1.6 cycles per degree (cpd)] or orthogonal 19-min stripes positioned at target distances of 1.5 m and 0.55 m. This corresponds to a change in accommodative stimulus of 1.15 D. The mean change in accommodation for both astigmatic and nonastigmatic subjects was approximately 0.8 D, which indicated that the subjects exhibited a change in accommodative response that was somewhat less than the stimulus, but no significant difference was found between the three types of stimuli tested.
Recent investigations have used video photorefraction to measure the refractive state of the eye in infants and children (27). The advantage of a video-based system is that it allows the captured images to be viewed almost immediately, thereby avoiding the risk of discovering that defective images have been obtained only after the child has left the laboratory or clinic.
Static digital recording devices would also have the same advantage. Video photorefraction has also been used to examine the dynamics of the accommodative response, and Howland et al. (27) used this technique to
demonstrate that the speed of accommodation in infants between 4- and 9-months of age was up to 4.6D per second. This is very similar to findings in adult subjects presented by Campbell and Westheimer (28) and Charman and Heron (29).
demonstrate that the speed of accommodation in infants between 4- and 9-months of age was up to 4.6D per second. This is very similar to findings in adult subjects presented by Campbell and Westheimer (28) and Charman and Heron (29).
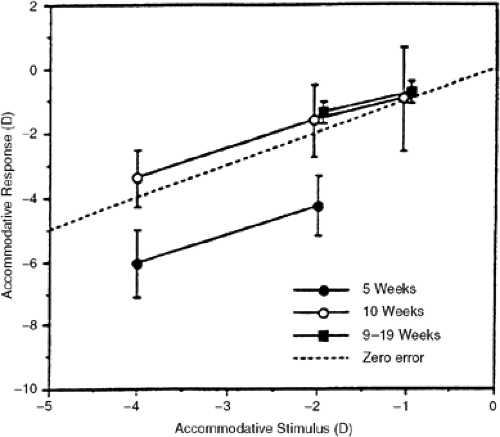 Figure 6.4 Mean accommodation stimulus-response function for infants 9 to 19 weeks of age (N = 15); 10 weeks of age (N = 4); and 5 weeks of age (N = 4). Accommodation was measured using an objective, open-field, infrared optometer. Error bars indicate ±1 SEM. (From Aslin RN, Shea SL, Metz HS. Use of the Canon R-1 autorefractor to measure refractive errors and accommodative responses in infants. Clin Vis Sci 1990;5:61–70 , with permission.) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


