6 Indications for Surgery on Pituitary Tumors: An Endocrinologist’s Perspective
Until 1970, only surgery or radiation therapy was available for the treatment of pituitary tumors. But four findings led to considering medical therapy as a further option: (1) prolactin existed in humans as a molecule separate from growth hormone1; (2) hyperprolactinemia caused sexual dysfunction, infertility, and galactorrhea; (3) many pituitary adenomas hypersecreted prolactin2; and (4) bromocriptine was effective in lowering serum prolactin and improving sexual function.3 Only later was it discovered that shrinkage of prolactin-secreting pituitary tumors could be expected in response to bromocriptine and that withdrawal of medication was associated with tumor enlargement.4,5 The concept that medical therapy might be an alternative to surgery and radiotherapy was subsequently extended to other functioning pituitary adenomas, including growth hormone (GH)-secreting6 and thyroid-stimulating hormone (TSH)-secreting tumors.7Althoughprogressregardingmedicaltreatment of Cushing’s disease is being made, this disorder and nonfunctioning pituitary adenomas are still the purview of neurosurgeons in most situations.
 Expertise of Pituitary Surgeons
Expertise of Pituitary Surgeons
The best results of surgery for pituitary tumors are achieved when surgeons are highly experienced and focused in resection of pituitary lesions. In a study by Gittoes et al,8 the outcome of surgical removal of pituitary adenomas by the transsphenoidal approach was better when a specific dedicated neurosurgeon performed the surgery, in contrast to when it was performed by one of eight otherwise excellent colleagues who had less experience in pituitary disease. The dedicated surgeon accomplished a cure rate of 86% for microadenomas and 52% for macroadenomas. In contrast, the success rates for the other eight neurosurgeons were 54% and 30%, respectively. That this was the experience in a single surgery unit indicates that the cure rates of a particular surgeon, in contrast to those of a specific medical center, should be quoted. This book discusses success rates of surgery by the endoscopic route, which may further help in the optimal choice of the neurosurgeon. It is not clear whether a direct comparison of the different surgical approaches will help identify one as being better than the others.9
 What Constitutes a Pituitary Tumor?
What Constitutes a Pituitary Tumor?
Pituitary tumors are found in 11% of autopsies,10 and they stain for prolactin in 46% of cases. They may also come to attention during imaging of the head for unrelated reasons. In one study, 10% of 100 normal volunteers had magnetic resonance imaging (MRI) findings indicative of microadenomas, ranging from 3 to 6 mm in diameter.11 When a tumor is incidentally found, it requires a full endocrine evaluation and at minimum periodic radiologic follow-up.12 In a survey of 248 patients with pituitary incidentalomas followed for a mean period of 26.9 months, 46.4% of the pituitary masses were nonfunctioning adenomas and only 20% of them were found to increase in size.13 Thus, incidentalomas infrequently require therapy.
Pituitary adenomas are also brought to attention because of endocrine dysfunction or tumor mass effect. These frequently require treatment. When considering whether a patient with a pituitary adenoma should be treated medically, surgically, or not at all, it is important to evaluate its size, invasiveness, effects on adjacent structures, and secretory activity, as well as the function of the remaining normal pituitary tissue (Table 6.1).
 Specific Types of Pituitary Tumors
Specific Types of Pituitary Tumors
Functioning Pituitary Tumors
Prolactin-Secreting Tumors
The great majority of prolactin-secreting tumors are responsive to dopamine agonists, whether they are micro-or macroadenomas. Dopamine agonists not only normalize serum prolactin values, which can reverse the associated sexual dysfunction, galactorrhea, and osteopenia, but also reduce adenoma size. Tumor shrinkage is due to a reduction in cell cytoplasm, nucleus, and nucleolus.14–16 Even with large invasive adenomas, medication should be the first-line therapy, as it often improves vision and other mass effects. It was initially shown that tumors that shrank in response to bromocriptine would regrow with discontinuation of the drug.5 They often do, but many, especially microadenomas, do not recur after withdrawal of dopamine agonist therapy.17 Taken together, these authors and most pituitary endocrinologists consider dopamine agonists the therapy of choice for prolactinomas.18
Table 6.1 Characteristics of Pituitary Tumors that May Require Therapeutic Intervention
| Effects of Pituitary Tumors | Related Clinical Features |
|---|---|
| Hypersecretion of prolactin | Sexual dysfunction, galactorrhea, |
| Hypersecretion of GH | reduced bone mineral density |
| Hypersecretion of ACTH | Features of acromegaly |
| Hypersecretion of TSH | Features of Cushing’s syndrome |
| Features of hyperthyroidism (with measurable TSH) | |
| Increase in intrasellar pressure | Headache |
| Compression of surrounding | Hypopituitarism |
| normal pituitary tissue | Hyperprolactinemia |
| Compression of pituitary stalk | |
| Acute hemorrhagic infarction | Pituitary apoplexy, hypopituitarism |
| Pressure on optic chiasm | Visual field defects |
| Invasion of cavernous sinus | Rare cranial nerve deficit (most often no clinical sequelae) |
| Invasion of temporal or frontal lobe | Seizures, changes in personality, anosmia, hydrocephalus |
| Download invasion | CSF leakage, pharyngeal obstruction, meningitis |
| Pituitary infection | Meningitis, pituitary abscess |
Abbreviations: ACTH, adrenocorticotropic hormone; CSF, cerebrospinal fluid; GH, growth hormone; TSH, thyroid-stimulating hormone. Note: Features in bold are most frequently observed.
Bromocriptine has been employed since the early 1970s and is very effective in reducing serum prolactin, normalizing gonadal function, and shrinking tumors. Its use is somewhat limited by side effects including postural hypotension, gastrointestinal disturbances, and poor tolerability in some. Moreover, it must be administered up to three times a day. In contrast, cabergoline can be given weekly, is better tolerated, and can be used in higher doses for tumors that are relatively resistant. In recent years it has been associated with cardiac valve thickening and regurgitation when used in much higher doses, as in Parkinson’s disease.19 The bulk of evidence, however, suggests that doses necessary to treat prolactinomas do not cause cardiac problems.
We believe that surgery should be considered in patients who are completely resistant to or intolerant of dopamine agonists, personally choose surgery, or have macroadenomas and want to prevent the development of visual problems during pregnancy.
Resistance to Dopamine Agonists
Dopamine agonists act by binding to dopamine receptors in prolactin-producing adenoma cells. Therefore, these drugs need available dopamine receptors to be effective. In general, patients resistant or relatively resistant to therapy with dopamine agonist have some reduction in the number of receptors available (Fig. 6.1). However, “resistance” is a relative term. In the literature it generally refers to failure to normalize prolactin in response to 15 mg of bromocriptine daily. If this definition were applied to all patients with macroprolactinomas, many would be considered resistant. In practice, patients with very high levels of serum prolactin do not always achieve complete normalization of prolactin. Nevertheless, they experience considerable tumor shrinkage, reduction in tumor mass effects, and normalization of previous deficiencies in other pituitary hormones. They may even have some restoration of sexual function. Therefore, we would not consider these patients fully resistant to dopamine agonist therapy even though they may require steroid hormone replacement or fertility treatment if pregnancy is desired. In contrast, rare individuals may present tumor growth despite prolactin being suppressed,20 whereas others benefit through either tumor shrinkage or reduction in serum prolactin, but not both. Some prolactin-secreting tumors grow in spite of treatment with dopamine agonists. These include nonmalignant and rare malignant prolactinomas. Under these circumstances, therapeutic considerations should include surgery, radiation therapy, chemotherapy, or a combination.
Prolactinomas and Pregnancy
The normal pituitary gland enlarges during pregnancy as a result of proliferation of pituitary lactotroph cells. Pituitary adenomas can also grow in response to pregnancy-related hormones. An enlarged pituitary tumor or gland can impair vision if it impinges on the optic chiasm. Fortunately, microadenomas rarely damage visual tract during pregnancy.21 Only 1.4% of patients with microadenomas develop visual abnormalities during pregnancy, whereas 16% of patients with macroadenomas do.10 Therefore, when a woman has a pituitary tumor in close proximity to the optic chiasm or a macroadenoma, the risk of experiencing visual disturbances in pregnancy should be considered. Even with a microadenoma we recommend visual field tests before and during pregnancy. Some patients with macroadenomas select prophylactic surgery prior to pregnancy, whereas others prefer undergoing treatment with dopamine agonist if it becomes necessary during the course of pregnancy. If the latter choice is taken, responsiveness to dopamine agonists should be determined before proceeding with a pregnancy.
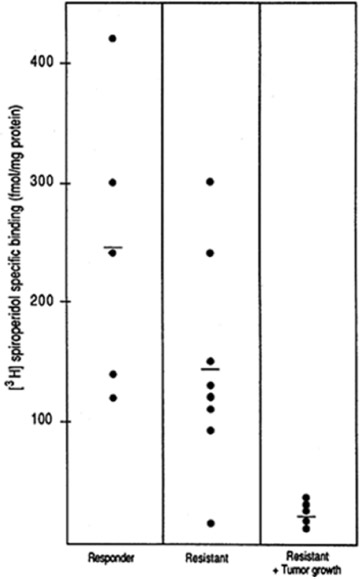
Fig. 6.1 Binding of dopamine agonist to dopamine receptors according to the sensitivity of prolactinomas to the drug. (From Pellegrini I, Rasolonjanahary R, Gunz G, et al. Resistance to bromocriptine in prolactinomas. J Clin Endocrinol Metab 1989;69:500–509)
Malignant Prolactinomas
Only 40 cases of malignant prolactinomas have been described. The diagnosis is made when there is evidence of metastasis outside the pituitary region. These tumors rarely respond to dopamine agonists and usually require combination therapy including debulking surgery, radiation therapy, and chemotherapy with temozolomide22 or other agents.
Growth Hormone–Secreting Tumors
Acromegaly leads to severe comorbidities and increased mortality, especially in patients who develop diabetes or heart disease.10
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


