Chapter 42 Incisions in Thyroid and Parathyroid Surgery
 This chapter contains additional online-only content, available on expertconsult.com.
This chapter contains additional online-only content, available on expertconsult.com.
Introduction
With the transformation of thyroid and parathyroid surgery since the late 1990s, there are now a variety of methods for accessing the thyroid and central neck. A number of technological advances such as advanced energy devices for hemostasis,1 high-resolution endoscopes for improved visualization,2 and laryngeal nerve monitoring3 have increased the focus on cosmetic outcomes and the pursuit of smaller, well-camouflaged incisions.4 Also emerging are techniques for remote access thyroid and parathyroid surgery.5,6 Conventional surgery remains necessary in many circumstances, such as for large substernal goiters or advanced malignancy, and will remain in the endocrine surgeon’s armamentarium.
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
Historical Perspectives
 Please see the Expert Consult website for more discussion of this topic, including Figure 42-1.
Please see the Expert Consult website for more discussion of this topic, including Figure 42-1.
Historical Perspectives
Modern thyroid surgery found its origins in the late 19th century in the work of Billroth and Kocher.7 Although Billroth is credited with first systematically pursuing thyroidectomy in a deliberate fashion, it was Kocher who developed a safe and reproducible technique for accomplishing a therapeutic thyroidectomy. He was able to demonstrate efficacy and efficiency through a low cervical collar incision that bears his name. Kocher himself, however, recognized the logic behind utilizing as small an incision as possible and is quoted as saying thyroidectomy incisions should be “as small as possible, as big as necessary,” therefore perhaps qualifying him as the first minimally invasive surgeon.
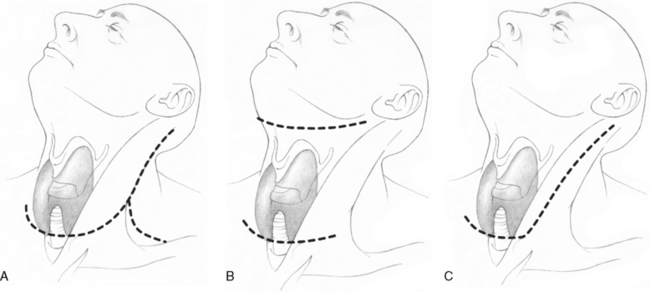
Because much of the earlier thyroid surgery was done for malignancy, descriptions emerged regarding the appropriate way to accomplish a thyroidectomy combined with a neck dissection. Popular incisions included the Lahey incision (Figure 42-1, A), the MacFee incision (Figure 42-1, B), and eventually a hockey stick type of incision (Figure 42-1, C).8 This last approach developed with recognition of the dangers of a trifurcated incision in which the tips of the trifurcation were prone to ischemia and devitalization, sometimes putting the great vessels of the neck at risk. As the “radical” operations of the 1960s and 1970s gave way to the more “selective” operations of the 1980s and 1990s, neck incisions for thyroid and neck dissection evolved.
General Principles
Individualizing Incisions
A concept that has gained traction in recent years is the customization of both the incision and the surgery to the patient and the disease characteristics, rather than a “one size fits all” approach.9 Historically, surgeons proposing to accomplish a thyroidectomy would make a standard length incision in a routine location and accomplish an identical operation for each patient. More recently, partly driven by public demand, ever smaller incisions have been utilized (when it can be done safely) in order to improve patient satisfaction, and the procedure is now tailored to the individual condition.
 Please see the Expert Consult website for more discussion of this topic, including Figures 42-2, 42-3, 42-4, and 42-5.
Please see the Expert Consult website for more discussion of this topic, including Figures 42-2, 42-3, 42-4, and 42-5.
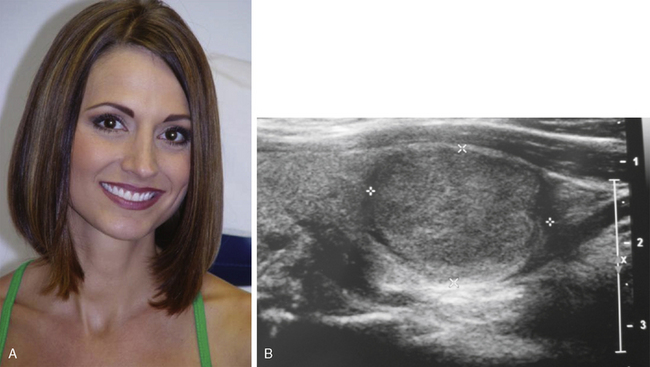
For example, a gentleman with a 26-inch neck (Figure 42-2, A) and a large goiter (Figure 42-2, B) is not a good candidate for any type of minimally invasive approach. By contrast, a television commentator with an 11-inch neck (Figure 42-3, A) and a 2-cm follicular neoplasm (Figure 42-3, B) is an ideal candidate for an endoscopic thyroidectomy. It is no longer sufficient to remove a thyroid, preserve the laryngeal nerves, and preserve the parathyroid glands (Figure 42-4). Patients now expect a more measured approach to their care, which sometimes includes quite small incisions (Figure 42-5).


Location
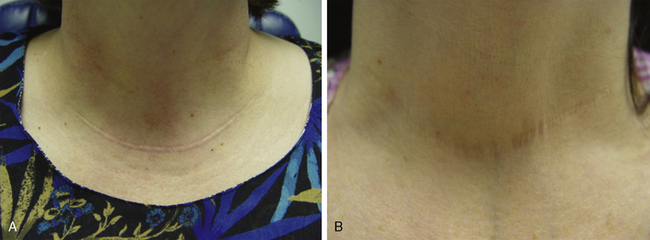
Perhaps the most important element in optimizing access while maintaining good cosmesis is choosing the proper location for an incision. It is nearly always preferable to identify and utilize a preexisting skin crease (if present), as this will result in the most optimally camouflaged scar. One must be cautious that normal creases may (especially in the more lateral portion of the neck) become asymmetrical and even “V” like in nature, rather than the more symmetrical rounded creases of the lower central neck. For standard-length incisions, a good alternate choice, if a normal symmetrical crease is not available, is a line parallel to a normal skin crease. All existing creases can be mapped out in order to configure an incisional line that is parallel to a regional crease. The best way to identify the proper crease and overall location is with the patient sitting upright in the preoperative holding area rather than waiting until the patient is lying supine on an operating table (Figure 42-6). It is in this position that patients will be in public situations such as dinner parties and cocktail receptions, and it is in this position the suprasternal notch (the depression created by the medial heads of the sternocleidomastoid muscle) can best be seen. In this way, the incision can be planned with the patient’s input and awareness. The standard incision is best placed above this suprasternal notch. Standard incisions that are placed too low, spanning this indented suprasternal notch region, may appear asymmetrical and tend to be hypertrophic in their midsegment as opposed to incisions higher, in a more uniform, cylindrical region of the neck. Minimally invasive incisions might be placed in the hollow between the medial heads of the sternocleidomastoid muscle. Consideration should be given to breast size, especially in younger women, as over time the incision will be pulled downward if the breasts are large and pendulous.

 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
The length of the incision will vary depending on the thickness of the neck and the size of the gland or nodule, although it should be noted that virtually always the benign gland or nodule can be bigger than the incision itself, as these structures are compressible and can be manipulated through an incision smaller than the gland. In any case, the incision should be parallel to relaxed skin tension lines, following classic cosmetic principles.10
Skin Management
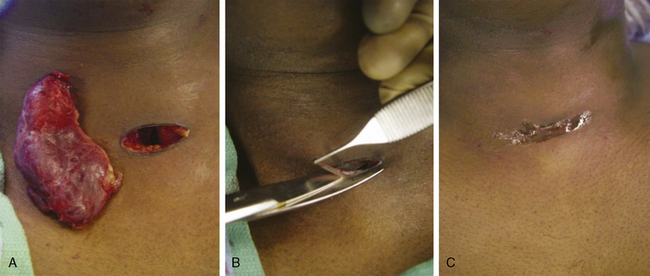
The contribution of the incision to the cosmetic outcome does not end with the making of the incision itself. It is important to minimize the amount of trauma to the skin edge, either from retraction or from inadvertent instrument trauma (for example, electrocautery and ultrasonic energy burns or gauze abrasion). We make every effort to eliminate the use of 4 × 4 gauze sponges during the operation, as the material is abrasive and behaves like sandpaper when it is placed into and retrieved from small incisions. However, despite careful technique, it is not uncommon to observe skin edges at the end of a procedure (particularly minimally invasive surgery) that are ischemic and traumatized. Because of the risk of hypertrophic scarring, we recommend resecting a sliver of skin edge whenever and wherever this is recognized (Figure 42-7). This helps to ensure proper wound healing in the postoperative period.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


