Fig. 1
Frontal view (a) from a contrast esophagogram shows a smooth round impression on the right side of the upper esophagus due to a right aortic arch (arrow). On the lateral view (b) there is a posterior impression on the esophagus due to an aberrant left subclavian artery (arrow). These findings constitute a vascular ring
Due to the complexity of its mechanism, swallowing is not thoroughly evaluated on a routine esophagogram or upper GI series. Swallowing dysfunction is better assessed with a modified barium swallow (MBS), during which the infant is fed in a semiupright position using barium-impregnated materials of various textures. These exams are recorded in real-time for later playback and detailed review. The MBS is useful for detecting laryngeal penetration and aspiration, and to aid in formulation of feeding plans.
Computed Tomography
Advantages
Recent technologic advances have allowed multidetector CT to become a powerful tool for imaging of the airways in small patients. Unlike bronchoscopy, CT is noninvasive, and can evaluate both the airway wall and the surrounding structures, rather than just the mucosal surface. Also unlike bronchoscopy, CT can demonstrate synchronous airway lesions, as well as demonstrate the distal effects of airway obstruction such as air-trapping and atelectasis [10]. CT offers numerous advantages over other imaging modalities, including a rapid acquisition time, decreased need for sedation, large field of coverage, high spatial resolution, and the ability to generate two-dimensional (2D) and three-dimensional (3D) reformatted images [2]. In addition, paired inspiratory–expiratory imaging and cine imaging can be performed using CT [2].
Technique
Unlike the simple conventional radiographic techniques described earlier, patient preparation is important in CT for maximizing image quality. With the large number of CT detectors available in modern machines, scanning times are relatively fast (in the order of seconds), and the majority of neonates do not require general anesthesia with intubation. Light sedation is recommended for CT exams in older infants [2], which will minimize motion artifact, but still allow the patient to independently maintain an airway.
For patients with suspected tracheobronchomalacia who require both inspiratory and expiratory phase CT, controlled ventilation techniques should be used. In intubated patients, positive pressure is applied during inspiration, and pressure is withheld during expiration [2]. In this way, the patient can be scanned first in “end-inspiration” and then in “end-expiration.” In sedated non-intubated patients, hypocarbia can be induced by augmenting inspiration through a face-mask. This results in a short apneic period (via the “Hering-Breuer reflex”) during which the patient is scanned at the desired degree of airway distention [10]. In patients for whom a controlled ventilation technique is not feasible, cine CT can be performed by rapidly acquiring axial images at specified levels, with the scan being performed throughout a free breathing respiratory cycle.
Because of the inherent contrast between the airways and soft tissue structures, routine CT evaluation of the airways does not require intravenous (IV) contrast. However in the absence of a specific indication or a previously known airway diagnosis, IV contrast should be used to define the mediastinal structures, and to assess for vascular anomalies such as rings or slings [2]. Note that prior to contrast-enhanced CT, patients must be thoroughly screened for risk factors for adverse reactions to contrast media, including contrast nephropathy and anaphylaxis. The recommended type of contrast material is a nonionic low-osmolar formulation, and the volume administered is calculated based on patient weight (typically 2 cm3/kg) [2]. The preferred method of contrast administration is through a mechanical power injector. For infants with smaller caliber catheters or central venous lines, contrast can be administered manually (“hand injection”) [2].
Technical parameters for performing neonatal chest CT vary by scanner type. In general, the machine with greatest number of CT detectors is best, and the minimum suggested number is 16 detectors. In accordance with the ALARA principle (As Low As Reasonably Achievable), radiation exposure to the patient should be minimized by adjusting CT parameters (milliamperage, kilovoltage) appropriately for the patient’s age and weight. Ultra-low radiation dose techniques can still provide high quality, diagnostic CT images of the airways [1, 2, 11]. In patients requiring paired inspiratory–expiratory CT, the second (expiratory) series can be performed using even further dose reduction, without affecting diagnostic confidence [11].
Image Analysis
The first step in interpretation of airway CT is review of the source (axial plane) images. Following this, the radiologist performs several post-processing steps using a specialized workstation, in order to fully understand the nature and extent of the airway lesion, and to define complex anatomy.
2D reconstruction techniques include curved planar reformatting (CPR), in which images can be created as reformations of the curve along the axis of the airway. This allows accurate airway length measurements, which can be used for treatment planning. Another 2D reconstruction technique is minimum intensity projection (MinIP) reformatting, in which images are formed by projecting the voxels with lowest attenuation (e.g., those in air-filled structures such as the airways and lungs). This enhances visibility of the tracheobronchial tree and lung parenchyma [2].
The key 3D reconstruction method used for airway evaluation is volume rendering. In this method, a computer algorithm detects the edges of the airway wall and creates a surface rendering. An external rendering (“virtual bronchography”) allows one to view the outer surface of the airway wall, and its relationship to surrounding structures. An internal rendering (“virtual bronchoscopy”) allows one to view the inner lumen of the airway, which mimics conventional/direct bronchoscopy. These methods are extremely useful for depicting complex anatomic relationships in three dimensions. Volume rendering provides life-like images, which may preclude the need for conventional bronchoscopy [2, 5] (Fig. 2a).
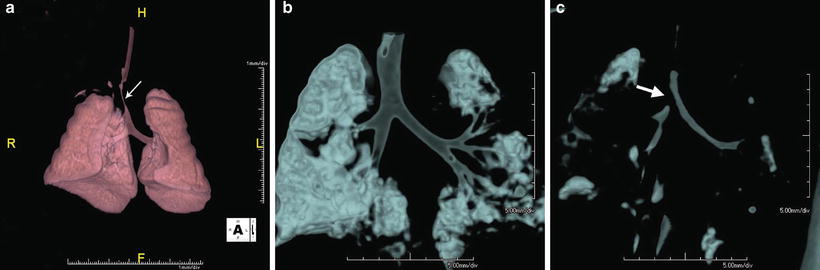
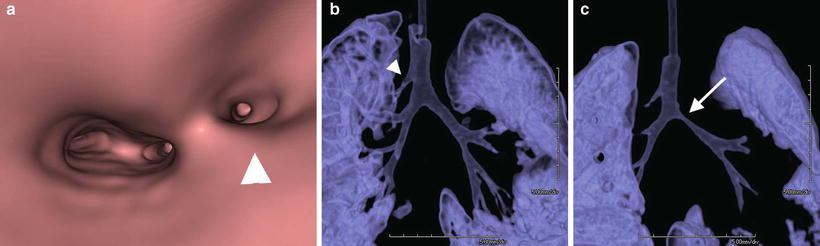
Fig. 2
(a) shows CT 3D colorful reconstruction of an infant with long-segment tracheal stenosis previously unrecognized on conventional radiologic modalities. Volume renderings of the airways in a different infant in both inspiratory (b) and expiratory (c) phases demonstrate diffuse decrease in caliber of the tracheobronchial tree during expiration. There is complete expiratory collapse at the origin of the right mainstem bronchus (arrow)
Magnetic Resonance Imaging
Like CT, MRI is a cross-sectional imaging modality which can provide information about the airway and mediastinal vessels. The major advantages of MRI are its lack of ionizing radiation, high soft tissue contrast, and the ability to image in multiple planes without changing the position of the patient. Cardiovascular MRI has excellent accuracy in diagnosis of vascular anomalies that cause airway compromise [12]. These exams are targeted to evaluation of the heart and major vessels using ECG-gated sequences, as well gadolinium contrast-enhanced angiographic sequences. MRI also has the capability for dynamic (“cine”) image acquisition. In current practice, cine MRI is primarily used to evaluate airway motion during sleep studies in older children with suspected obstructive sleep apnea, as well as patients with glossoptosis and hypopharyngeal collapse [5]. Cine imaging is also used in some centers for assessing lung, chest wall, and diaphragm motion in patients with thoracic insufficiency syndrome [1].
There are some disadvantages of MRI which limit its utility in the neonatal age group. Depending on the clinical indication, current MRI protocols may require scan time of up to 30–60 min, and the majority of infants will require sedation or cardiac anesthesia [3]. In young infants (usually less than 6 months old), a “feed and swaddle” method can be attempted, and may obviate the need for anesthesia or deep sedation [12]. Evaluation of the lung parenchyma on MRI is limited due to artifacts from air-tissue interface susceptibility, as well as respiratory and cardiac motion. However, newer techniques such as respiratory triggering, respiratory gating, and motion-insensitive sequences have enhanced the pulmonary imaging capability of MRI. MRI technology is a rapidly evolving field, and future improvement of scan time and image quality will make this a valuable modality for assessment of the neonatal airway.
Fetal Imaging
Although this text is focused on postnatal imaging of the neonatal airway, awareness of fetal imaging is also important for all clinicians involved with management of prenatally diagnosed airway lesions. Airway lesions for which fetal imaging is critical include neck masses (e.g., vascular malformations, teratomas) and congenital high airway obstruction syndrome (CHAOS) [10, 13]. Fetal ultrasound (US) and MRI are used in complement to assess these obstructive airway lesions prior to delivery, and to help determine the need for an ex utero intrapartum therapy (EXIT) procedure.
Fetal US is a real-time examination which allows direct observation of swallowing and respiration, and Doppler US is used for evaluation of vascular structures. Fetal MRI has the added ability to examine the fetus in a large field of view and in multiple planes. MRI is superior to US for soft tissue contrast, characterization of masses and their effect on the airway, and for evaluation of cartilaginous structures such as the oropharynx and nasopharynx [13]. Both modalities are necessary for complete assessment of fetal airway compromise, and for guiding management decisions.
Imaging Features of Specific Neonatal Airway Disorders
Tracheobronchomalacia
TBM of the trachea and mainstem bronchi can be visualized on airway fluoroscopy, but at times the diagnosis is difficult, or the underlying cause cannot be determined. In these patients CT is helpful for more complete evaluation, and is especially useful for evaluating caliber of airways distal to the mainstem bronchi. Since TBM can be missed on static CT images, an additional expiratory series is typically performed to assess for change in size of the tracheobronchial tree (Fig. 2b, c). The criteria for diagnosis of TBM on CT is the reduction of airway cross-sectional area by 50 % or more, and this criteria has been shown to be concordant with bronchoscopy results [14]. Cine (4D) CT can depict airway collapsibility in real-time, and is best performed on CT machines with 64 or more detectors [15].
In addition to identifying the presence, location, and severity of airway malacia, CT provides information about predisposing conditions, and offers quantitative measures for preoperative planning. CT also depicts the distribution of expiratory air-trapping and inspiratory alveolar recruitment [16].
Congenital Malformations
Branching Anomalies
There are multiple variant branching patterns of the tracheobronchial tree. Some of the most common are ectopic bronchi, supernumerary bronchi, and tracheal diverticulum [2, 17]. These variants are uncommon and usually found incidentally, but rarely they are responsible for air-trapping, recurrent atelectasis, repeated infections, and aspiration [18]. The most well-known ectopic bronchus is the tracheal bronchus (“bronchial suis” or pig bronchus), which is a small upper lobe bronchus that arises from the lateral wall of the trachea above the carina (Fig. 3a–c). A tracheal diverticulum is a congenital outpouching which arises from the posterolateral wall of the trachea near the thoracic inlet, and has a narrow neck [5]. Acquired tracheal diverticulum may be posttraumatic or due to increased transluminal pressure, and usually have a wide neck [5, 19].