Immunotherapy is an excellent treatment option for a selected subset of patients with inhalant allergies. It consists of intentional serial exposures to allergens, which modulate the immune system and induce immune tolerance through down-regulating the allergic response, resulting in an overall decrease in symptoms. Immunotherapy has been shown to have long-term efficacy in the management of inhalant allergies, as reflected by diminished frequency and duration of symptoms and improved quality of life. The therapy is considered safe, with side effects limited mostly to minor local reactions, and only occasional cases of systemic adverse reactions.
- •
Allergy immunotherapy involves the sequential administration of antigen to patients with symptomatic, atopic conditions to induce tolerance to the offending antigens.
- •
Numerous well-controlled studies have documented the efficacy of immunotherapy in the treatment of both allergic rhinitis and asthma.
- •
Although subcutaneous immunotherapy can be rarely associated with serious adverse systemic reactions, it is generally safe and well tolerated.
- •
Immunotherapy is associated with decreased health care costs.
Between 30 and 60 million Americans are diagnosed with allergic rhinitis (AR) annually. AR affects between 10% and 30% of adults, and as many as 40% children. The current management options include environmental control; pharmacologic therapy including oral and intranasal antihistamines, steroids, and decongestants, and antileukotriene receptor antagonists and mast cell stabilizers; and allergen immunotherapy. Immunotherapy is a fascinating area of research and an attractive choice of therapy because it is the only option with the potential to change the natural course of allergy.
The first documented description of clinical application of allergy immunotherapy dates back to the early 20th century. In 1911, Noon and Freeman reported the successful treatment of patients with hay fever using pollen injections. Since then, protocols and techniques have evolved, although core concepts have remained the same. Specific immunotherapy (SIT) involves a series of controlled exposures to escalating doses of allergen, which alter immune system pathways and down-regulate the allergic response, thereby decreasing the allergic symptoms associated with exposure to environmental allergens.
Mechanism
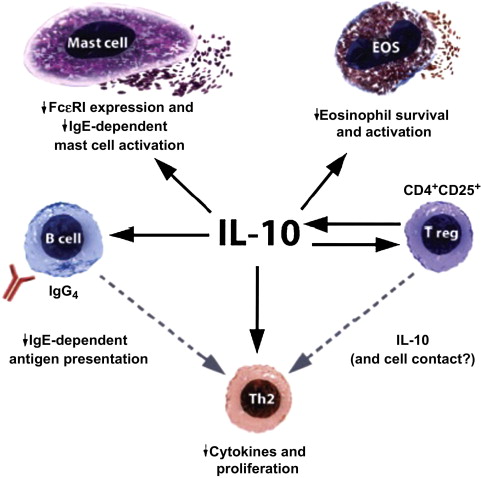
Despite intense research in the areas of immunology and allergy, a precise and detailed mechanism of immunotherapy remains to be elucidated. It is known, however, that immunotherapy induces several in vitro changes at molecular and cellular levels. The first immunologic difference can be detected as early as 7 days after initiation of immunotherapy, as manifested by a rise in cytokine interleukin (IL)-10. IL-10 has been shown to play a central role in tolerance induction and immunologic change with immunotherapy ( Fig. 1 ).
Shortly after beginning SIT, a slight increase in IgE is noted. Levels of IgE subsequently decrease, and a rise in IgG and IgA levels occurs, particularly IgG4 and IgA2. The rise in IgG can be seen at as early as 5 weeks, and is predictive of response to immunotherapy at 1 year. The simultaneous decline in IgE levels and increase in IgG levels have been described as a “scissors effect” and have led to development and popularization of a blocking antibody concept. IgG antibodies were once believed to prevent binding of allergen to mast cell and basophil-bound IgE, thereby blocking degranulation of these modulators of allergic response. Recent evidence, however, suggests that the shift in antibody levels is a mere effect of immunotherapy, not the driving mechanism.
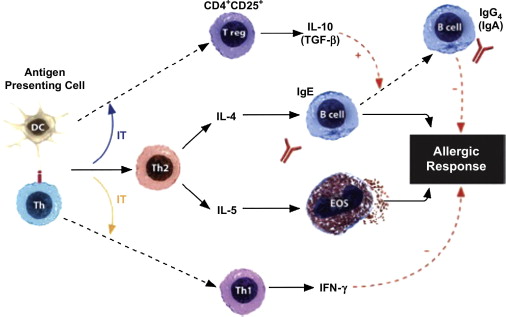
In the early 1980s thymus-derived effector and helper lymphocytes were identified as the key components of hypersensitivity. T-helper 1 (Th1) cells are primarily involved in Gell and Coombs type 4 delayed reactions, and T-helper 2 (Th2) cells are predominant in Gell and Coombs type 1 immediate hypersensitivity reactions. Th2 cells produce IL-4, IL-5, and IL-13, which direct B lymphocytes to switch to IgE production. IL-5 also promotes eosinophil activity in the peripheral tissues. Th1 cytokines, such as interferon gamma, transforming growth factor β, and IL-10, inhibit IgE production and are involved in Th2 regulation. In atopic conditions, such as allergic rhinoconjunctivitis and asthma, the T-cell balance is shifted toward proallergic Th2, with subsequent increase in proinflammatory agents. Early observations of decreased expression of the Th2 cytokines IL-4 and IL-5 and increased levels of the Th1 cytokines IL-2 and IL-12 led to the belief that immunotherapy works through restoring the normal Th1/Th2 balance ( Fig. 2 ).
How this balance is restored remains unclear; although it is probably an end result of a complex interaction of different modulators at both cellular and molecular levels. Currently, thymic lymphocytes known as T-regulatory cells (T-reg) are known to play a key role ( Fig. 3 ). T-reg cells constitute 10% of circulating lymphocytes and have been shown to regulate tolerance to both self (internal) and non-self (external) antigens. The increase in T-reg cell levels can be detected as early as 6 hours after administration of SIT and is directly correlated with the Th2 to Th1 shift.
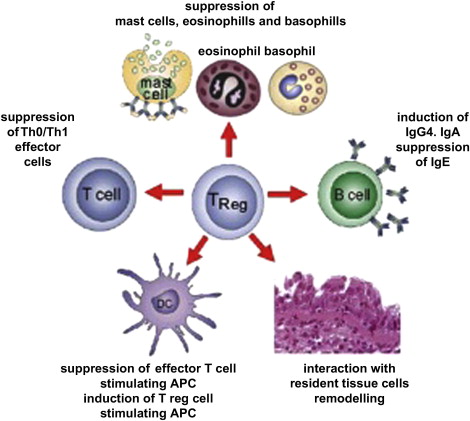
On repetitive presentation with an allergen, T-reg cells are able to differentiate into T-reg 1 subtype, capable of producing IL-10 or transforming growth factor β. Both are known to modulate T-cell activity, favoring Th1 proliferation. B-cell phenotype is also affected as isotype switching toward IgG4 and IgA is promoted, resulting in suppression of IgE. Finally, activation and migration of eosinophils and mast cells to target tissues are diminished.
Patient selection
Immunotherapy targets a particular patient population, in whom symptoms of allergy are induced through exposure to identifiable allergens. The degree of response to prior environmental modulation and maximal pharmacologic treatment, duration and severity of symptoms, and patient compliance must be reviewed. SIT should be considered in patients who do not experience response to or are unable to tolerate the side effects of conventional therapy. Alternatively, allergic immunotherapy should be offered to patients who wish to avoid long-term dependence on pharmacologic agents or are seeking a potential cure for their disease.
According to the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines, indications for immunotherapy in adults and children older than 5 years of age include :
- 1.
Patients with symptoms induced predominantly by allergen exposure.
- 2.
Patients with a prolonged season or with symptoms induced by succeeding pollen season.
- 3.
Patients with rhinitis and symptoms from the lower airways during peak allergen exposure.
- 4.
Patients in whom antihistamines and moderate-dose topical glucocorticoids insufficiently control symptoms.
- 5.
Patients who do not want to be on constant or long-term pharmacotherapy.
- 6.
Patients in whom pharmacotherapy induces undesirable side effects.
In addition to clinical symptoms, objective evidence of the presence of IgE antibodies specific to those allergens must be identified and documented in the form of either in vitro testing, such as radioallergosorbent test (RAST) or enzyme-linked immunosorbent assay (ELISA), or in vivo testing, such as intradermal, prick, or combined skin testing. Alternatively, the testing can be classified as qualitative and quantitative. The goal of qualitative testing is to identify the offending allergen. Quantitative testing attempts to detect both presence and degree of sensitivity. Intradermal skin end point titration (SET) and modified quantitative testing (MQT) are considered the standard quantitative methods. SET involves intradermal injections of serial fivefold dilutions of antigen into the skin, until the end point, or the extent of sensitivity, is determined. MQT is a more efficient form of intradermal testing. It uses percutaneous technique at the initial stage to estimate the level of sensitivity, followed by selected intradermal tests to assess a more precise level of response. Because of this blended method, MQT results in shorter testing time with less expense.
To maximize patient safety, immunotherapy based on qualitative testing must be initiated at very dilute concentrations, because the degree of sensitivity is not determined, and significant adverse events can occur with treatment. Immunotherapy based on quantitative methods, however, has an excellent index of safety. Experts have also suggested that patients managed with SIT based on quantitative testing experience clinical improvement sooner. The hypothesis behind this observation is that higher concentrations of allergen can be delivered at the initial stages of immunotherapy.
As stated by Haydon and Gordon, “the only absolute contraindication to immunotherapy is failure to prove that a relevant allergy exists.” However, immunotherapy is strongly discouraged in patients whose medical status would preclude them from surviving a systemic adverse reaction or its treatment . Several relative contraindications also exist, the most serious being poorly controlled asthma, because the risk of anaphylaxis is greater in patients with reduced pulmonary function. Patients on β-blocker drugs are considered high risk because the systemic reaction may be more severe and more resistant to management with adrenergic agents, such as epinephrine.
Pregnant patients also deserve special consideration. Although initiating or escalating the schedule in a pregnant patient is not recommended, continuing the maintenance dosing is considered safe. Other patients who requiring careful management are those with established autoimmune abnormalities, because development of autoimmune disease has been reported in patients being treated with SIT.
Patient selection
Immunotherapy targets a particular patient population, in whom symptoms of allergy are induced through exposure to identifiable allergens. The degree of response to prior environmental modulation and maximal pharmacologic treatment, duration and severity of symptoms, and patient compliance must be reviewed. SIT should be considered in patients who do not experience response to or are unable to tolerate the side effects of conventional therapy. Alternatively, allergic immunotherapy should be offered to patients who wish to avoid long-term dependence on pharmacologic agents or are seeking a potential cure for their disease.
According to the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines, indications for immunotherapy in adults and children older than 5 years of age include :
- 1.
Patients with symptoms induced predominantly by allergen exposure.
- 2.
Patients with a prolonged season or with symptoms induced by succeeding pollen season.
- 3.
Patients with rhinitis and symptoms from the lower airways during peak allergen exposure.
- 4.
Patients in whom antihistamines and moderate-dose topical glucocorticoids insufficiently control symptoms.
- 5.
Patients who do not want to be on constant or long-term pharmacotherapy.
- 6.
Patients in whom pharmacotherapy induces undesirable side effects.
In addition to clinical symptoms, objective evidence of the presence of IgE antibodies specific to those allergens must be identified and documented in the form of either in vitro testing, such as radioallergosorbent test (RAST) or enzyme-linked immunosorbent assay (ELISA), or in vivo testing, such as intradermal, prick, or combined skin testing. Alternatively, the testing can be classified as qualitative and quantitative. The goal of qualitative testing is to identify the offending allergen. Quantitative testing attempts to detect both presence and degree of sensitivity. Intradermal skin end point titration (SET) and modified quantitative testing (MQT) are considered the standard quantitative methods. SET involves intradermal injections of serial fivefold dilutions of antigen into the skin, until the end point, or the extent of sensitivity, is determined. MQT is a more efficient form of intradermal testing. It uses percutaneous technique at the initial stage to estimate the level of sensitivity, followed by selected intradermal tests to assess a more precise level of response. Because of this blended method, MQT results in shorter testing time with less expense.
To maximize patient safety, immunotherapy based on qualitative testing must be initiated at very dilute concentrations, because the degree of sensitivity is not determined, and significant adverse events can occur with treatment. Immunotherapy based on quantitative methods, however, has an excellent index of safety. Experts have also suggested that patients managed with SIT based on quantitative testing experience clinical improvement sooner. The hypothesis behind this observation is that higher concentrations of allergen can be delivered at the initial stages of immunotherapy.
As stated by Haydon and Gordon, “the only absolute contraindication to immunotherapy is failure to prove that a relevant allergy exists.” However, immunotherapy is strongly discouraged in patients whose medical status would preclude them from surviving a systemic adverse reaction or its treatment . Several relative contraindications also exist, the most serious being poorly controlled asthma, because the risk of anaphylaxis is greater in patients with reduced pulmonary function. Patients on β-blocker drugs are considered high risk because the systemic reaction may be more severe and more resistant to management with adrenergic agents, such as epinephrine.
Pregnant patients also deserve special consideration. Although initiating or escalating the schedule in a pregnant patient is not recommended, continuing the maintenance dosing is considered safe. Other patients who requiring careful management are those with established autoimmune abnormalities, because development of autoimmune disease has been reported in patients being treated with SIT.
Allergen selection
The most commonly used allergen extracts are derived from dust mites, cat and dog dander, cockroach, molds, and pollens of trees, grasses, and weeds. Extracts are prepared in aqueous, alum-precipitated, or lyophilized solutions. Standardized extracts are supplied in concentrations expressed in allergen units (AU) or bioequivalent allergy units (BAU). In the process of standardization, the biologic activity of the allergen is calibrated to the concentration units through the use of intradermal skin testing in selected reference populations. The U.S. Food and Drug Administration currently endorses 19 standardized allergen preparations.
One challenging decision for clinicians is how many allergens to treat. Proponents of the blocking antibody theory argue for using all offending allergens, so that a specific antibody is formed for each one of them. However, the effectiveness of immunotherapy can be compromised through the use of too many antigens, because each individual component can become too dilute to exert effect. Furthermore, in accordance with the currently accepted theory that immunotherapy normalizes immune system mechanisms, treating for the few prominent offenders should be sufficient to induce overall immune tolerance. Treatment patterns therefore vary among allergists practicing in the United States, and between domestic and international allergists.
A literature review by Nelson concluded that concurrent delivery of multiple properly identified antigen extracts in adequate quantities is clinically effective. In the author’s opinion, several prominent allergens should be selected for treatment based on the patient’s past medical history with respect to exposure to the suspected allergens, results of allergy testing, and patterns of allergens’ seasonal and geographic distribution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


