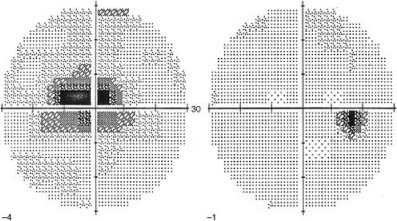
Chapter 20 Idiopathic inflammation of the optic nerve occurs in isolation or in the context of more widespread demyelinating disease. Initial evaluation is directed at confirming acute optic nerve dysfunction, differentiation from other acute optic neuropathies, and may later include extensive ancillary testing to assess both for current evidence and future risk of multiple sclerosis (MS). The patient referred with suspected optic neuritis should be evaluated by an ophthalmologist within 24 hours. Optic neuritis occurs most frequently in young women age 20 to 40. Acute onset of central visual loss, described as “dim” or “foggy” vision, or a gray central blur with color washout, developing over several days. Periorbital aching pain, particularly with eye movement, occurs in roughly 90% of patients; the globe itself may be tender as well. Visual acuity is usually reduced, as the majority of cases involve the papillomacular bundle of retinal nerve fibers subserving the central fixation region of vision. The classic pattern of visual field loss is a central or cecocentral scotoma (Fig. 20–1). However, generalized depression of the central 30-degree field is actually more common, and altitudinal or arcuate field defects are also frequently seen. A relative afferent pupillary defect is invariably present, unless bilateral involvement produces symmetrically impaired pupillary light responses. The optic disc may appear normal (65%) or edematous (35%) (Fig. 20–2). With recurrent episodes, the disc may become atrophic. Peripheral retinal venous sheathing may be present in 10 to 15% of cases, more often in those with MS. The following features should raise the question of alternate diagnoses: FIGURE 20–1 Visual fields in optic neuritis. Left eye (on left) demonstrates a central scotoma. Right eye shows normal field with physiologic blind spot.
IDIOPATHIC OPTIC NEURITIS
URGENCY OF EVALUATION
DIAGNOSIS
SYMPTOMS
Demographics
Visual Loss
Pain
SIGNS
Visual Acuity
Visual Field
Pupils
Optic Disc
Other Abnormalities
Red Flags
 Evidence of intraocular inflammation (suggests uveitis with secondary optic nerve involvement)
Evidence of intraocular inflammation (suggests uveitis with secondary optic nerve involvement)
 Visual field pattern suggesting chiasmal involvement (superotemporal field loss in the fellow eye) suggests anterior chiasmal compressive lesion
Visual field pattern suggesting chiasmal involvement (superotemporal field loss in the fellow eye) suggests anterior chiasmal compressive lesion
 Orbital signs such as proptosis, extraocular muscle dysfunction, lid ptosis or retraction (suggests orbital mass or inflammation)
Orbital signs such as proptosis, extraocular muscle dysfunction, lid ptosis or retraction (suggests orbital mass or inflammation)
 Pain continuing more than 2 to 3 weeks (suggests orbital inflammation, posterior scleritis)
Pain continuing more than 2 to 3 weeks (suggests orbital inflammation, posterior scleritis)
 Sequential involvement of the fellow eye (suggests Leber’s hereditary optic neuropathy)
Sequential involvement of the fellow eye (suggests Leber’s hereditary optic neuropathy)
 Lack of visual recovery (suggests atypical inflammation, ischemia, infiltration, or compressive optic neuropathy)
Lack of visual recovery (suggests atypical inflammation, ischemia, infiltration, or compressive optic neuropathy)
DIFFERENTIAL DIAGNOSIS
Inflammatory and Infectious Optic Neuropathies (see Chapter 21)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


