Purpose
To describe a case series of enlarged extraocular muscles in young patients.
Design
Retrospective interventional case series.
Methods
Study involves 6 young patients who presented with atypical restrictive strabismus and reduced eye movements. Examination, neuroimaging, biochemistry results, and biopsy results are presented. The surgeries are described, and the follow-up over 1-20 years is presented.
Results
All 6 patients had enlarged extraocular muscles that caused restrictive strabismus. The patients had no significant medical history. There was no identifiable underlying pathology on biochemistry tests or muscle biopsy. Three of the patients required multiple surgeries.
Conclusion
Atypical presentations of strabismus should be investigated for systemic conditions. Neuroimaging of the orbit and brain and a biopsy of the affected muscles should be considered. The patients should be counseled that multiple surgeries may be necessary to improve the strabismus, and it is unlikely that orthotropia will be attained.
Extraocular muscle (EOM) enlargement in adults is commonly due to thyroid eye disease, inflammatory myositis, or sarcoidosis, or is secondary to neoplastic infiltrate. In adults there is often a constellation of symptoms and signs that aid in diagnosis. Pediatric EOM enlargement is much rarer than in adults and, consequently, it is more difficult to determine etiology.
In children, the restrictive strabismus may be misdiagnosed as a congenital cranial nerve palsy before imaging is obtained. There have been case reports of inflammatory, neoplastic, and vascular lesions causing enlarged EOM, and rare cases of thyroid eye disease. There have also been case reports of congenital idiopathic enlargement.
We present a case series of 5 cases of pediatric enlarged EOM for which no underlying pathology could be identified. We also provide an update on 1 case that was previously reported, but now with a 20-year follow-up.
Methods
This is a retrospective interventional case series of 6 patients from 3 institutions (Department of Ophthalmology and Vision Sciences of The Hospital for Sick Children, Toronto, Canada; Department of Ophthalmology of Stanford University, Stanford, California; and Department of Ophthalmology and Visual Science at the University of Nebraska Medical Center, Omaha, Nebraska). A review of patient charts, their clinical presentation and examination, imaging, operative details, surgical pathology results, and postoperative outcomes was performed.
The Research Ethics Board at The Hospital for Sick Children, Toronto, waived the need for Research Ethics Board approval. The study and data accumulation were in conformity with all country, federal, or state laws. Informed consent was obtained for presentation and publication of clinical history, photographs, and imaging, and the study was in adherence to the tenets of the Declaration of Helsinki.
Case Reports
Case 1
A 5-month-old male subject presented in 2006 with a deviation of the left eye from birth. On examination he was noted to have left hypotropia of 10 prism diopters (PD) and a 35 PD left exotropia ( Figure 1 , Top left). His upgaze was reduced by 50% ( Figure 1 , Middle left). Pupillary examination and the remainder of the ophthalmic examination was normal. Systemic examination by a pediatrician was normal. The patient had a fixation preference for the right eye and was diagnosed with left amblyopia. Patching of the right eye for 2 hours daily was started. His cycloplegic refraction was +0.50+2.50×100 in the right eye and +0.50+3.00×80 in the left.
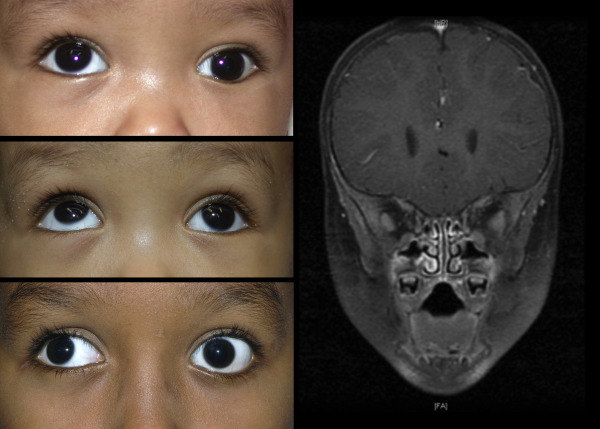
He underwent a magnetic resonance imaging (MRI) scan of the brain and orbits that showed thickening and enhancement of the muscle bellies of the left lateral rectus and inferior rectus, both near the orbital apex, with no tendon enlargement ( Figure 1 , Right). There was no change to the MRI 6 months later, and thyroid function tests, antithyroid autoantibody, and inflammatory markers were all normal.
At age 18 months, surgery was performed. Forced duction testing at surgery confirmed a tight left inferior rectus and lateral rectus. Intraoperatively both of the muscles appeared normal in thickness and consistency distally. No muscle biopsy was obtained. The left lateral rectus was recessed 8 mm and the inferior rectus was recessed 3 mm.
Three months postoperatively, the patient developed a right hypertropia of 30 PD, and at age 3 he underwent a second operation. The left inferior rectus was found 10 mm from the limbus and was further recessed 3 mm, and the right superior rectus was recessed 6 mm. A 1 mm × 3 mm muscle biopsy was obtained from the left inferior rectus muscle belly posterior to the muscle insertion. The biopsy revealed dense connective tissue and fibrosis, a reduced number of skeletal muscle fibers, and marked fiber size variability. There was no evidence of inflammation or tumor.
Over the 6 years after the second operation, the patient developed an alternating A-pattern exotropia of 30 PD, with mild right hypertropia and superior oblique over-action ( Figure 1 , Bottom left) A third strabismus operation was performed at age 9. The right lateral rectus was recessed 7.5 mm and both superior oblique tendons were lengthened by 5.0 mm with 5-0 polyester suture (Mersilene; Ethicon, Cincinnati, Ohio). Six months after surgery, the patient remained orthotropic in primary gaze, with mild superior oblique over-action. His vision was 20/20 in the right eye and 20/30 in the left.
Case 2
A 5-year-old male subject presented in 2011, with a 1-year history of right-sided strabismus. He was in good general health. On examination he had right upgaze deficit of 25% in adduction and 75% in abduction. There was a right hypotropia of 30 PD, with a chin-up head position ( Figure 2 , Left). Vision was 20/80 in the right eye and 20/30 in the left eye. Cycloplegic refraction was +1.00 diopters in both eyes. The remaining ophthalmic examination was normal.
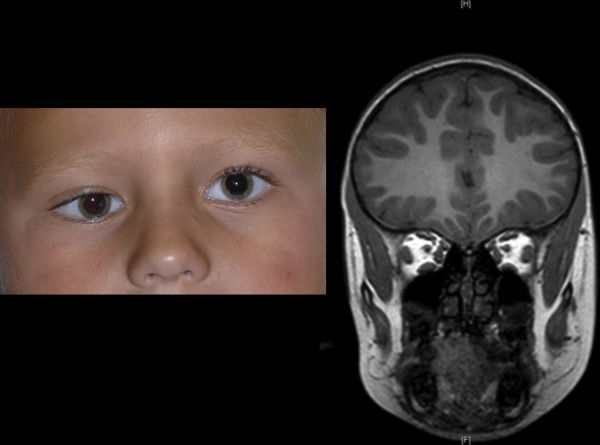
An MRI revealed that the patient had enlarged diameter of all 4 rectus muscles in both eyes, with a normal orbital floor and tendon-sparing enlargement ( Figure 2 , Right). A repeat MRI at age 6 exhibited the same features with no interval changes. Thyroid function tests, antithyroid autoantibody tests, and inflammatory markers were normal.
Surgery was performed at age 7 to correct his abnormal head position. On forced duction testing at surgery, the right inferior rectus was tight, and the superior oblique was normal. Right inferior rectus recession of 5.5 mm with a partial hangback technique was performed.
Follow-up over 14 months revealed that the right eye had 3 PD of hypertropia and had 25% reduction in both upward and downward movement. Patching for amblyopia has improved the right visual acuity to 20/30.
Case 3
This case was previously reported in 1994. The patient was an 8-month-old infant who presented in 1990 with a 5-month history of left strabismus, left-sided ptosis, and a chin-up head posture. On examination, she had signs of left-sided amblyopia, and patching of the right eye was commenced. She had a left hypotropia of 30 PD and a left esotropia of 10 PD. She had 100% left upgaze limitation from her primary position and 50% limitation of left eye abduction.
Her thyroid function tests were normal. Computed tomography (CT) scan at age 1 showed enlargement of the left medial and inferior rectus muscles and, to a lesser degree, the left lateral rectus muscle. The tendons were spared. Follow-up imaging at 18 months and an MRI at age 2 showed no changes in findings.
Surgery was performed for the strabismus at the age of 2. Forced duction testing at surgery was positive in the left eye on abduction and supraduction. The left medial and inferior rectus muscles had normal appearance and insertion location. The left medial rectus and the left inferior rectus were both recessed 10 mm to balance the forced duction test results. Postoperatively, the patient gradually developed an exotropia. She underwent a second surgery with biopsy and recession of the left lateral rectus muscle. Biopsy of the belly of the lateral rectus showed some variability of muscle fiber diameter and some scattered atrophic fibers, but no inflammatory infiltrate. Electron microscopy did not reveal any structural abnormality.
Two years following the second operation, there was a small left hypertropia in primary gaze, with limitation of left upgaze by 75%, downgaze by 25%, and abduction by 25%. The patient was happy with the cosmesis.
On follow-up at age 18, she still had the mild left upper lid ptosis, which was worse when she was tired. There was equal vision in both eyes. She had a left exotropia of 10 PD. She had 100% limitation of left upgaze and 50% limitation of left downgaze. She had 75% limitation of abduction and adduction from primary gaze in the left eye.
Over the next 3 years, there was gradual increase in left hypotropia in primary gaze to 35 PD. There was no improvement in left eye movements, and the right eye had corresponding 50% over-action on upgaze. A repeat MRI had similar findings as noted previously, with left medial, lateral, and inferior rectus enlargement in the mid and posterior portions and the remaining muscles having a normal appearance.
Owing to the significant left hypotropia in primary gaze, a third strabismus operation was performed at age 21. Forced duction testing at surgery was positive on supraduction, and the left inferior rectus and inferior oblique had significant scarring around it on exploration. The scar tissue was freed and there was noticeable improvement on forced duction. No further recession or myectomy was performed. In the early postoperative phase, there was a residual left hypotropia of 15 PD.
Case 4
A 6-month-old female subject presented in 2013 with a right-sided head tilt ( Figure 3 , Top left), right ptosis, and right strabismus. On examination, there was a minimal right upper lid ptosis of 0.5 mm. The patient had a right exotropia of 30 PD and a right hypotropia of 20 PD, and an associated 50% reduction in right-sided upgaze and a 25% limitation in right-sided adduction ( Figure 3 , Bottom left). There was mild right amblyopia, so 2 hours daily patching of the left eye was started. Cycloplegic refraction of the right eye was +3.50−1.00×90 and left eye was +1.50 diopters. The remainder of the ophthalmic examination was normal, and the patient was otherwise healthy systemically.
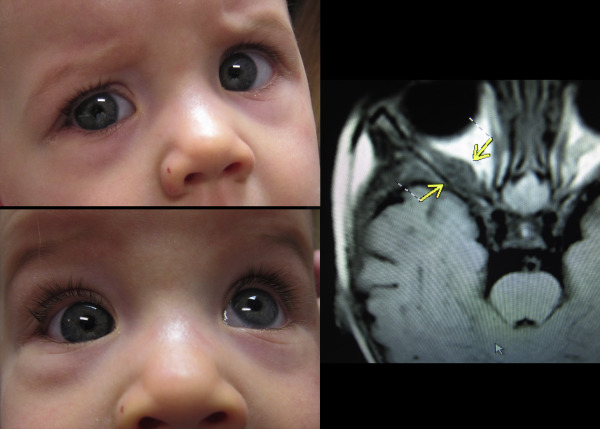
An MRI demonstrated a soft tissue mass in the right orbit, centered in the posterior aspect of the right lateral rectus muscle and extending toward the orbital apex ( Figure 3 , Right). The mass was homogenous with minimal enhancement. It measured 14 mm in the anteroposterior plane, with a 5.2 mm transverse diameter. There were no signs of optic nerve compression or extension toward the cavernous sinus.
A trial of oral prednisolone at 1 mg/kg for 7 days did not result in any improvement. Based on the above findings, and to exclude a neoplastic cause, a muscle biopsy through an orbitotomy approach was performed. The biopsy revealed fragments of skeletal muscle that had mild inflammation and some degenerating fibers. The CD45 immunohistochemistry demonstrated presence of rare inflammatory cells.
Strabismus surgery was performed at age 12 months. The scar around the right lateral rectus was dissected, and the right inferior rectus was recessed 5.5 mm. Six months after surgery the patient had a slight head tilt. There remained limited right eye supraduction, but the right exotropia and hypotropia was reduced to 5 PD and 8 PD, respectively.
Case 5
A 9-month-old male subject presented with a history of intermittent exotropia from birth. Initial examination in 2006 confirmed a left intermittent exotropia for distance fixation, with no deviation at near. The pupils were equal, and there was no ptosis. The patient was otherwise systemically healthy. He was brought back for an atropine refraction and fundus examination. On the second visit, a right head turn with a chin-up position was noted. On examination, there was a 100% limitation in left eye adduction and 100% reduction in left eye infraduction. There was a left exotropia of 20 PD and there were some signs of left amblyopia, for which patching was commenced. His cycloplegic refraction was +2.00 diopters in the right eye and +3.00+0.50×90 in the left eye.
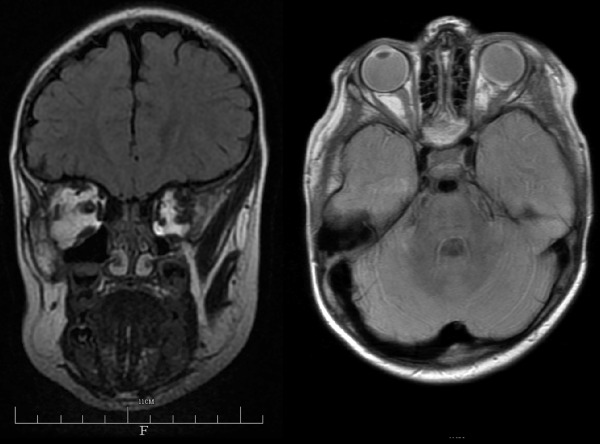
MRI scan at age 10 months revealed a thickened left lateral rectus that was partially confluent with a partially displaced and thickened superior rectus ( Figure 4 ). There was no other orbital mass or pathology visible.
During the course of a year, the left exotropia gradually increased to 50 PD for distance and 20 PD for near. There was increased upgaze limitation in the left eye. A follow-up MRI was organized, but the family was lost to further follow-up.
Case 6
A 25-year-old male subject had a history from birth of right esotropia. He was otherwise healthy and on no medications. There was no other significant medical history, and no previous ocular surgery or trauma.
On examination, the vision was counting fingers in the right eye and 20/25 in the left eye. He had greater than 100 PD right esotropia and greater than 10 PD hypotropia ( Figure 5 , Top left). The eye did not abduct from this position, and there was a 100% limitation of elevation. Force generation testing in clinic revealed no elevating force in the right eye and a 50% reduced abducting force.



