50
Idiopathic Central Serous Retinopathy
Carlos A. Moreira Jr.  Juan Ignacio Verdaguer
Juan Ignacio Verdaguer  Juan V. Espinoza
Juan V. Espinoza  J. Fernando Arevalo
J. Fernando Arevalo
Idiopathic central serous retinopathy (ICSR), also called central serous chorioretinopathy or choroidopathy, is considered to be an accumulation of serous fluid underneath the sensory retina, commonly affecting the posterior pole. Associated with serous detachment of the neurosensory retina, one or more areas of retinal pigment epithelium (RPE) detachment may be found.
PREVALENCE
This disease typically affects young and middle-aged adults in their third to fifth decades of life. Males are affected more commonly than females by a ratio of 8:1 or 9:1 (1, 2). ICSR often occurs in white, Asian, and Hispanic men, and is rare in Blacks (2). It has been speculated that psychological factors such as stress might play a role in determining the disease (3).
CLINICAL FINDINGS AND NATURAL HISTORY
Before the onset of symptoms, patients develop a serous detachment of the RPE, and they become symptomatic only if the central macula is affected. Serous detachment outside the posterior pole may not be detectable by the patient.
Patients who are symptomatic complain of a sudden decrease of central vision in many ways, such as blurred or dim vision, micropsia, metamorphopsia, or decreased color vision. A relative central scotoma and metamorphopsia usually can be demonstrated in the Amsler grid. In some patients, the onset of symptoms is preceded or accompanied by migraine-like headaches (3). There are no other diseases associated with ICSR. Patients’ medical history, physical examination, and family history are usually unremarkable.
Visual acuity in the acute stage is often decreased moderately, averaging 20/30, although a wide range of acuities can be observed ranging from normal to 20/200, depending on the amount of the serous detachment affecting the macula. Small hyperopic corrections may improve vision to 20/20 in some cases.
The diagnosis can be made with ophthalmoscopy and biomicroscopy by identifying a round or oval area of retinal elevation in the posterior pole, slightly darker than normal, which may be surrounded by a halo of light reflex. The foveal reflex is usually absent. Because this disease is not of inflammatory origin, there are no inflammatory cells in the vitreous cavity.
The slit-lamp examination of the posterior pole using a fundus lens with the light beam directed a few degrees off the visual axis provides an adequate stereoscopic view of the macula, allowing for correct diagnosis. The serous detachment is usually transparent, although a diffuse gray to white subretinal deposit may be present. There is evidence that this white appearance is caused by the presence of fibrin, especially in longstanding cases (2). If the detachment is relatively shallow, a shadow from the retinal vessels over the RPE may be present. A yellow spot may be seen at the center of the fovea, or multiple small yellow precipitates may be detected under the detached retina.
One or multiple RPE detachments may occur. Usually the RPE detachment appears as a small, yellowish, round lesion, located beneath the superior half of the area of retinal detachment (2). Owning to gravity, the accumulation of subretinal fluid tends to be inferior to the area of RPE detachment. Sometimes it is possible to have RPE detachments outside the area of the retinal serous detachment.
Patients with recurrent ICSR may show areas of mottled depigmentation of the RPE underneath the serous detachment. It is common to find many areas of altered pigmentation of the RPE without active leakage in the affected or fellow eye.
Most of the patients with ICSR (80%–90%) experience spontaneous resolution of the serous detachment in 8 to 12 weeks after the onset of symptoms (4). Visual acuity often returns to normal in 1 to 6 months, although mild color defects and relative scotomas may persist indefinitely (5). Although most patients recover normal vision, approximately 5% do not reach 20/30 acuity. Fewer than 20% develop a serous detachment in the opposite eye (2).
Recurrences are relatively frequent and occur 40% to 50% of cases (2, 6). In such cases, progressive deterioration of the RPE in the macular area may account for the persistent decrease in visual acuity. In rare instances, ICSR can cause the formation of subretinal neovascular membranes, especially in recurrent and prolonged detachments.
FLUORESCEIN ANGIOGRAPHY
Fluorescein angiography is the diagnostic method tool that is most useful in determining the pathophysiology and the correct diagnosis of ICSR. The classic appearance of a hyperfluorescent spot at the level of the RPE allows for a better understanding of the disease.
Characteristically, a small hyperfluorescent leak appears during the choroidal or arterial phase of the angiogram increasing in size and intensity as the angiogram progresses (Fig. 50-1). The leak, resembling an ink spot, is commonly observed. A “smokestack” appearance of the leak, although pathognomonic of the disease, occurs only in about 10% of the cases (7). Such a smokestack pattern occurs because of convection streams of the heated and lighter dye (8), which spreads vertically in a configuration evocative of a plume of smoke (Fig. 50-2).
Fluorescein angiography identifies the areas of detached RPE in which the serous fluid from the choriocapillaris is entering the subretinal space. Although the initial diffusion of dye is quite fast, it may take 20 minutes after injection for the dye to reach the borders of the serous detachment of the retina. Usually, there are only one or two leaking points, although many areas of focal leakage may be found (Fig. 50-3). The foci of leakage are located at the fovea in only 10% of cases (3). Most commonly, focal leaks are found in the macular area 1 mm adjacent to the fovea. The superonasal and inferonasal quadrants are the most frequently affected (9).
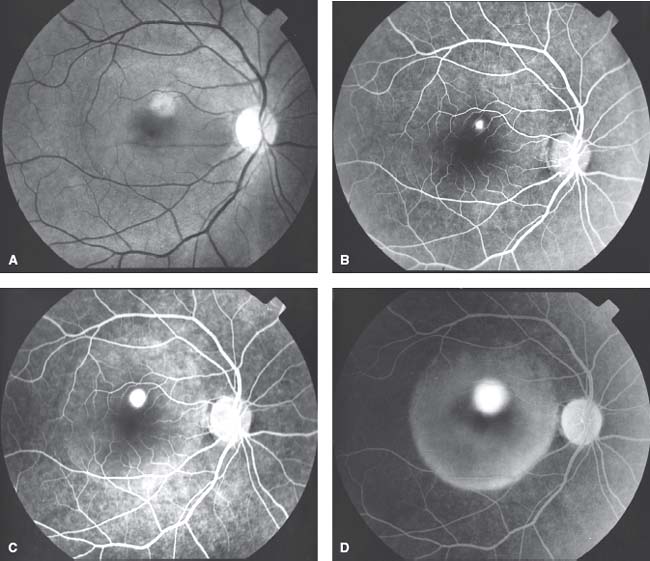
Figure 50-1. Idiopathic central serous retinopathy, acute form. A: Red-free retinography of a patient. Note a white dot in the superior area of the macula. B: Fluorescein angiography from an early arteriovenous phase of the same patient showing a small hyperfluorescent spot superior to the macula. C: Later phase of the angiogram showing enlargement of the hyperfluorescent spot and the initial hyperfluorescence in the subretinal space. D: Late phase of the angiogram showing hyperfluorescence of the retinal pigment epithelium detachment in the subretinal space.
In recurrent cases, approximately 80% of new leaks are located adjacent to the previous site (Fig. 50-4). Therefore, it is often difficult to determine if the leakage is new or just a reactivation of the primary pathology (10).
If the leak cannot be found one should consider two possibilities: the leak has already healed and the subretinal fluid will be absorbed in the next few days, or the leak is outside of the detached area. Therefore, one should always take angiographic images outside of the affected area, especially in the regions superior to the macula and the optic disc. It is important to realize that the serous detachment tends to extend to the foveal region even though the leak may be located eccentrically, because in this area the adhesion of the neurosensory retina to the RPE is weaker due to the absence of rods (3).
Once the tissue has healed, the angiographic findings may return to normal, although evidence of RPE detachment may persist. In recurrent cases, focal areas of depigmentation are present.
Research with indocyanine green angiography (ICG-A) has contributed novel information. Such studies have demonstrated presumed hyperpermeability of the choroidal vasculature surrounding the leaking sites seen on the fluorescein angiogram. Additional areas of choroidal hyperfluorescence not related to active leaking sites and multiple occult serous detachments of the RPE have been elucidated in some cases (11–16).
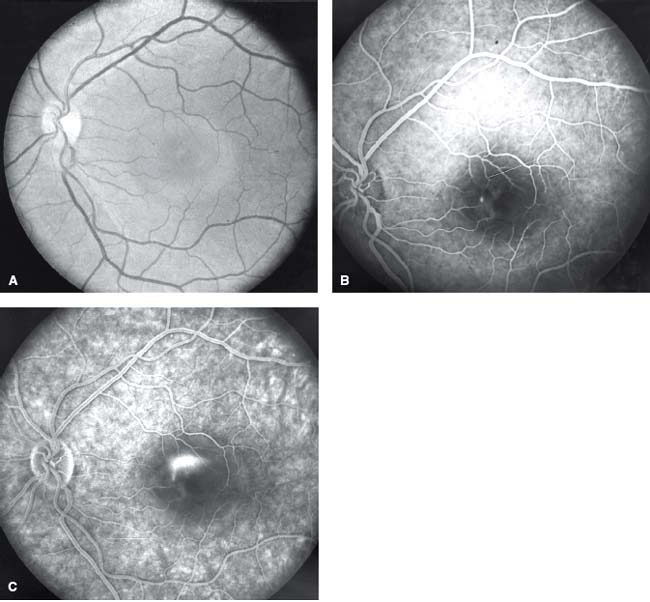
Figure 50-2. Idiopathic central serous retinopathy, acute form. A: Central serous detachment of the retina. B: Small retinal pigment epithelium leak in the angiogram. C: Diffusion of the dye into the subretinal space in a “smoke-stack” pattern.
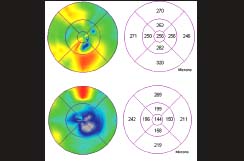
FUNDUS AUTOFLUORESCENCE
Recently fundus autofluorescence (FAF) has emerged as a noninvasive technique to study ICSR in different stages of the disorder. As previously stated, ICSR is a condition characterized by idiopathic leaks from the level of the RPE leading to serous retinal detachment. Patients with acute leaks imaged within the first month have minimal abnormalities seen in their FAF other than a slight increase in autofluorescence of the serous detachment.
When serous detachment persists for some time, the area of detachment becomes increasingly hyperautofluorescent. This autofluorescence is diffuse but contains discrete granules. After resolution of subretinal fluid, the accumulation of fluid on the outer retina is resorbed as well, and the hyperautofluorescence abates (17). Patients with chronic ICSR, having varying degrees of atrophy, show a mixed pattern of autofluorescence (Fig. 50-5). Additional deposition of material such as subretinal lipid and fibrin has been described in patients with ICSR. Lipid deposits and subretinal fibrin are not autofluorescent (17).
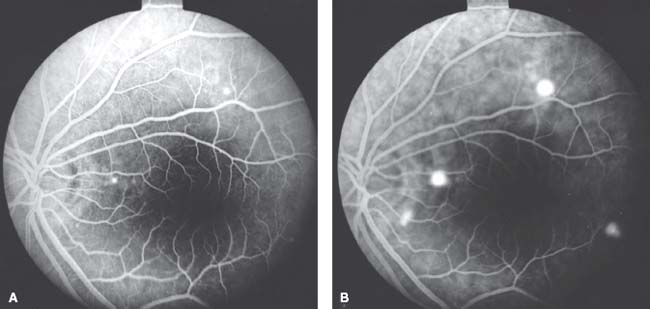
Figure 50-3. A: Patient with idiopathic central serous retinopathy and multiple retinal pigment epithelium detachments. Note two small hyperfluorescent spots. B: Same patient in a later phase of the angiogram showing four hyperfluorescent areas of detachment.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


