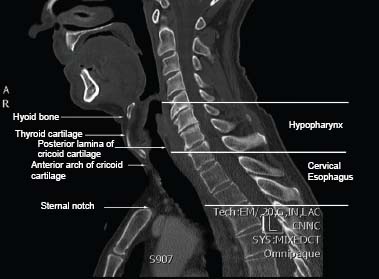
18 Core Messages • Work-up should include direct laryngoscopy and biopsy for hypopharyngeal tumors and endoscopic ultrasound for tumors of the cervical esophagus. • The primary management for locally advanced cancers of the cervical esophagus and hypopharynx is chemoradiotherapy with surgical salvage for those with persistent local disease after treatment. • Cancers of the cervical esophagus and lower hypopharynx have a high incidence of nodal metastasis, and careful attention must be paid to management of the neck. • Superficial cancers of the hypopharynx and cervical esophagus may be managed with endoscopic surgery or other larynx-preserving surgeries in centers with experience with these techniques. Cancers of the hypopharynx and cervical esophagus are relatively uncommon, together accounting for less than 10% of cancers of the upper aerodigestive tract and less than 5% of cancers of the head and neck.1–3 Cancers of the cervical esophagus account for only approximately 5% of all esophageal cancers. The incidence of cancers of the hypopharynx and cervical esophagus is currently 1:100,000 in North America and has been steadily decreasing, with a drop of more than 30% in each site between 1975 and 2001.2 No significant improvements in survival have been seen in population-based registries in either carcinoma of the hypopharynx or cervical esophagus.2,3 Squamous cell carcinoma (SCC) is the predominant histology, comprising more than 95% of cancers of the hypopharynx and 85% of cancers of the cervical esophagus. Adenocarcinoma is the second most common histology in the cervical esophagus, comprising 9% of the cases. Other less common histologies include lymphoma, adenoid cystic carcinoma, and small cell carcinoma.2 The most common age range at presentation for cancers of the hypopharynx and cervical esophagus is 50 to 80 years. Men are two to three times more likely to be diagnosed than women. Smoking and alcohol are the two largest risk factors for the development of SCC of the hypopharynx and cervical esophagus. Cigarette smoking increases the risk, with an odds ratio (OR) of 3 to 5, and this risk is modified by the age at which started smoking, total number of years smoked, number of packs smoked in a day, and current smoking status.4,5 The risk of SCC of the head and neck and esophagus remains elevated up to at least 10 years after smoking cessation. Cigar and pipe smoking also increases the risk of cancers of the upper aerodigestive tract but not to the same degree as cigarette smoking. Those who abuse alcohol also have an increased risk of cancers of the upper aerodigestive tract, and this effect is multiplicative in those who smoke as well, with an increased OR of up to 35. There is also evidence that the use of alcohol in individuals with polymorphisms in alcohol dehydrogenase and aldehyde dehydrogenase increases the risk for cancers of the upper aerodigestive tract.6 Infection with the human papillomavirus (HPV) has been implicated in the pathogenesis of cancers of the upper aerodigestive tract, and HPV16 is the predominant genotype. The oropharynx is the site with the highest incidence of HPV-related SCC, with up to 50% of the cases in North America associated with HPV. HPV association is not as common in other cancers of the aerodigestive tract, with one review revealing an incidence of 13.8% in cancers of the larynx and hypopharynx in North America with higher incidence in other parts of the world.7 A meta-analysis of patients with head and neck cancer demonstrated an improved prognosis in HPV-related oropharyngeal cancer but not HPV-related cancers of the oral cavity, larynx, and hypopharynx.8 The hypopharynx and cervical esophagus are adjacent structures in the head and neck. The hypopharynx begins inferior to the oropharynx, and the superior border is the vallecula. This begins at a plane at the superior border of the hyoid bone. The inferior border of the hypopharynx is the cervical esophagus, which begins at a plane at the inferior border of the cricoid cartilage. The inferior border of the cervical esophagus is at the thoracic inlet, which begins at a plane at the sternal notch (Fig. 18.1 and Table 18.1). The length of the cervical esophagus can vary on the basis of age, gender, and body habitus, but measurements on endoscopy are generally 15 to 20 cm from the incisors. Figure 18.1 Sagittal computed tomography of the neck revealing the anatomic boundaries of the hypopharynx and cervical esophagus. The hypopharynx consists of three subsites: the postcricoid region, pyriform sinuses, and lateral and posterior hypopharyngeal walls. The postcricoid region is posterior to the arytenoid and cricoid cartilages and forms the anterior border of the hypopharynx, connecting the two pyriform sinuses. The right and left pyriform sinuses begin at the pharyngoepiglottic fold and extend down to the cervical esophagus and are bound laterally by the lateral hypopharyngeal wall. Both the hypopharynx and the cervical esophagus have a rich lymphatic drainage that is commonly bilateral. The upper hypopharynx drains through an anterior collecting system with lymphatics from the supraglottic larynx that exit the thyrohyoid membrane to drain to levels II and III. The posterior collecting system drains the inferior hypopharynx and exits the superior constrictor muscle to drain to lateral retropharyngeal, paratracheal, and internal jugular chain lymph nodes. Locally advanced SCCs of the hypopharynx can also involve levels IV and V. Contralateral lymph-node metastases are common as bilateral lymphatic drainage occurs along superficial lymphatics of the posterior pharyngeal wall.9 The lymphatic drainage of the esophagus is concentrated in the submucosal layer, but lymphatic channels also exist in the lamina propria. Lymphatics penetrate the muscularis propria to drain to regional lymph nodes. Even superficial tumors have access to this rich lymphatic drainage system and have a propensity for lymph-node metastasis.10 SCC of the cervical esophagus can result in metastases to cervical, upper mediastinal as well as recurrent nerve lymph nodes.11 The number of lymph nodes involved, and not the location, is related to prognosis, and this is reflected in the current edition of the American Joint Committee on Cancer (AJCC) staging manual. Cancers of the hypopharynx and cervical esophagus often present with advanced disease. The most common presenting symptom is dysphagia. Dysphagia can present with “sticking” of certain solid foods such as meats and can progress to complete dysphagia to solid foods and then liquids. Weight loss can occur because of dysphagia, dietary changes, and tumor anorexia. Patients can also have hoarseness due to recurrent laryngeal nerve involvement or involvement of the cricoarytenoid joint or the cricoarytenoid muscle. Unilateral or bilateral otalgia can also be present in cancer of the hypopharynx due to referred pain from cranial nerves IX and X. Other symptoms can include hemoptysis, cough, and anemia. Complete obstruction of the cervical esophagus can result in an inability to clear secretions, and erosion into the trachea can result in tracheoesophageal fistula. Work-up of cancers of the hypopharynx and cervical esophagus should start with a thorough physical examination. Lesions in the superior hypopharynx may be seen with mirror examination or fiberoptic laryngoscopy (Fig. 18.2). However, lesions in the lower hypopharynx and cervical esophagus may not be seen with either mirror examination or laryngoscopy and requires rigid endoscopy. Palpation of the neck can reveal the presence of suspicious cervical nodes. Diagnosis should be made by biopsy performed during endoscopy. Fine-needle aspiration for cytology may be performed on suspicious cervical lymph nodes with a sensitivity of 89.5% and a specificity of 96.5 to 98.5%.12 Table 18.1 Anatomic Boundaries of the Hypopharynx and Cervical Esophagus
Hypopharynx and Cervical Esophagus Cancer
Epidemiology
Anatomy
Lymphatic Drainage
Patient Evaluation and Staging
Hypopharynx | Cervical Esophagus | |
Superior border | Vallecula | Plane at inferior border of the cricoid cartilage |
Inferior border | Plane at inferior border of the cricoid cartilage | Plane at sternal notch |
Anterior border | Arytenoid and cricoid cartilage | Trachea |
Posterior border | Prevertebral cervical fascia | Prevertebral cervical fascia |
Lateral border | Carotid sheath | Carotid sheath |
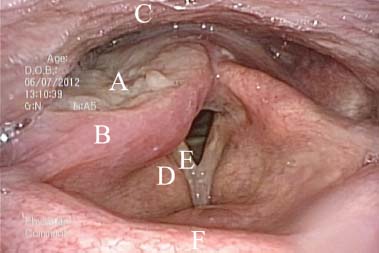
Figure 18.2 A right pyriform sinus tumor. Structures as follows: (A) right pyriform sinus tumor, (B) right aryepiglottic fold, (C) posterior pharyngeal wall, (D) right false cord, (E) right true cord, and (F) epiglottis.
Imaging studies play an important role in the work-up of SCC of the hypopharynx and cervical esophagus as physical examination, laryngoscopy, and endoscopy often cannot determine the extent of local invasion or regional and distant dissemination to accurately stage the patient (Tables 18.2 and 18.3). Computed tomography (CT) imaging can identify the invasion of adjacent structures and cortical bone as well as retropharyngeal, paratracheal, and upper mediastinal lymph-node metastases (Fig. 18.3). A study found that CT imaging upstaged the primary tumor (T) or regional lymph node (N) stage in 90% of hypopharynx cancers, with two-thirds of these upstaged in the T stage and one-third upstaged in the N stage.13 In head and neck cancers, CT imaging increases the sensitivity for detecting cervical node metastases compared with physical examination from 74 to 83%, with the specificity increasing from 81 to 83%.14 The sensitivity of CT imaging for regional nodal metastasis is lower for esophageal carcinoma at 50%, with a specificity of 83%.15
Positron emission tomography (PET) has improved sensitivity compared with CT in detecting regional nodal metastasis as well as distant metastasis. One study showed an increase in sensitivity from 82 to 90% for detecting nodal metastasis in SCC of the head and neck with PET compared with CT imaging.16 In esophageal cancer, PET increased the sensitivity in detecting regional nodal metastasis from 50 to 57%. While providing modest increases in sensitivity for detecting regional nodal metastasis, in esophageal carcinoma PET improves the sensitivity in detecting distant metastasis from 52% to 71%, with the specificity increasing from 91% to 93%.15 Integrated PET-CT can improve the accuracy of PET alone by providing anatomic correlation to areas of increased 18F-flouro-2-deoxy-d-glucose uptake and decreasing the number of equivocal lesions.17 In detecting distant metastases, PET-CT has a sensitivity of 97.5%, a specificity of 92.6%, a positive predictive value of 62.9%, and a negative predictive value of 99.7%.18 While PET-CT is very good at ruling out distant metastasis, positive findings should be interpreted with caution and confirmed histologically when possible.
To properly assess T and N stages in SCC of the cervical esophagus, endoscopic ultrasound (EUS) should be performed. EUS can visualize the different layers of the esophageal wall and determine the depth of invasion into these layers to assess the T stage (Fig. 18.4). Superficial esophageal carcinomas can be further subclassified into M 1-3 on the basis of the depth of mucosal invasion and SM 1-3 on the basis of the depth of submucosal invasion (Table 18.4). The accuracy of EUS for T stage depends on operator experience, depth of the tumor invasion, or the presence of a malignant stricture but is generally between 80 and 90%.19 The sensitivity and specificity for detecting regional nodal metastasis with EUS are 80 and 70%, respectively.15
Treatment
The management of SCC of the cervical esophagus and hypopharynx is complex and should be managed in a multidisciplinary setting including otolaryngology, thoracic surgery, medical oncology, radiation oncology, diagnostic radiology, pathology, gastroenterology, dentistry, speech and language pathology, and nutrition. The optimal management of SCC of the cervical esophagus is controversial, and there is considerable regional variation in treatment. Most patients with carcinoma of the hypopharynx or cervical esophagus present with locally advanced disease, and some institutions prefer surgical resection with either adjuvant or neoadjuvant chemotherapy or chemoradiotherapy, and other institutions prefer definitive chemoradiotherapy with surgical salvage for local failure. In the case of early stage disease, less invasive options may be available.
Endoscopy—Cervical Esophagus
Superficial SCC of the cervical esophagus was traditionally managed surgically with esophagectomy. However, endoscopic treatments are now being used for carefully selected superficial lesions. Tumor invasion into the submucosa is associated with a 38% risk of lymph-node metastasis, and endoscopic management alone should be avoided in these patients because of the increased risk of recurrence.20 Patients with M3 tumors that exhibit lymphovascular invasion also have an increased risk of lymph-node involvement (up to 18%) and may require further therapy.21 Endoscopic mucosal resection (EMR) has been in use for more than 20 years and can yield equivalent local control and survival and reduced morbidity compared with esophagectomy in esophageal carcinoma confined to the mucosa.20 EMR should not be used in patients with cirrhosis and esophageal varices and should be used with caution in patients with multifocal disease. Lesions greater than 2 cm often require piecemeal resection and are more likely to experience local recurrence after EMR. Endoscopic mucosal dissection (EMD) has been in use for more than 10 years and allows for en-bloc resection of larger lesions. A meta-analysis revealed that EMD produced higher rates of en-bloc resection and complete resection and lower rates of local recurrence compared with EMR. However, EMD was associated with longer procedure times as well as increased rates of bleeding and perforation.22 There is limited experience with endoscopic therapies such as EMR plus photodynamic therapy, argon plasma coagulation, radiofrequency ablation, and laser ablation, and the use of these techniques in superficial esophageal carcinoma remains investigational.
Table 18.2 American Joint Committe on Cancer Staging for Hypopharynx
Primary tumor (T) | |
• T1 | Tumor limited to one subsite of the hypopharynx and/or 2 cm or less in greatest dimension |
• T2 | Tumor invades more than one subsite of the hypopharynx or an adjacent site, or measures more than 2 cm, but not more than 4 cm in greatest dimension without fixation of the hemilarynx |
• T3 | Tumor more than 4 cm in greatest dimension or with fixation of hemilarynx or extension into the esophagus |
• T4a | Moderately advanced local disease. Tumor invades thyroid/cricoid cartilage, hyoid bone, thyroid gland, or central compartment soft tissuea |
• T4b | Very advanced local disease. Tumor invades prevertebral fascia, encases carotid artery, or involves mediastinal structures |
Regional lymph nodes (N) | |
• Nx | Regional lymph nodes cannot be assessed |
• N0 | No regional lymph-node metastasis |
• N1 | Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension |
• N2 | Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension, or in multiple ipsilateral lymph nodes, not more than 6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, not more than 6 cm in greatest dimension |
• N2a | Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension |
• N2b | Metastasis in multiple ipsilateral lymph nodes, not more than 6 cm in greatest dimension |
• N2c | Metastasis in bilateral or contralateral lymph nodes, not more than 6 cm in greatest dimension |
• N3 | Metastasis in a lymph node, more than 6 cm in greatest dimensionb |
Distant metastasis (M) | |
• M0 | No distant metastasis |
• M1 | Distant metastasis |
Source: Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010.
aCentral compartment soft tissue includes prelaryngeal strap muscles and subcutaneous fat.
bMetastasis at level VII is considered regional lymph-node metastasis.
Table 18.3 American Joint Committe on Cancer Staging for Esophagus
Primary tumor (T)a | |
• Tx | Primary tumor cannot be assessed |
• T0 | No evidence of primary tumor |
• Tis | High-grade dysplasiab |
• T1 | Tumor invades lamina propria, muscularis mucosae, or submucosa |
• T1a | Tumor invades lamina propria or muscularis mucosae |
• T1b | Tumor invades submucosa |
• T2 | Tumor invades muscularis propria |
• T3 | Tumor invades adventitia |
• T4 | Tumor invades adjacent structures |
• T4a | Resectable tumor invading pleura, pericardium, or diaphragm |
• T4b | Unresectable tumor invading other adjacent structures, such as aorta, vertebral body, and trachea |
Regional lymph nodes (N)c | |
• Nx | Regional lymph nodes cannot be assessed |
• N0 | No regional lymph-node metastasis |
• N1 | Metastasis in one to two regional lymph nodes |
• N2 | Metastasis in three to six regional lymph nodes |
• N3 | Metastasis in seven or more regional lymph nodes |
Distant metastasis (M) | |
• M0 | No distant metastasis |
• M1 | Distant metastasis |
Source: Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010.
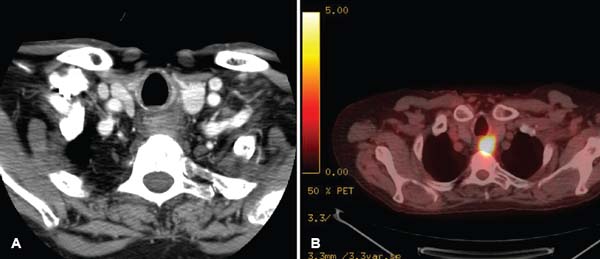
Figure 18.3 Cervical esophagus primary seen on axial (A) contrasted computed tomography (CT) of the neck and (B) positron emission tomography (PET)-CT.



