OSA SURGICAL EVALUATION
A thorough history and physical examination are the foundation of any surgical examination, but there are specific components and possible additional studies that have particular relevance to hypopharyngeal and skeletal surgery. As is true for nasal and palatal surgery, the examination must evaluate the anatomical factors that can contribute substantially to upper airway obstruction. Hypopharyngeal procedures are ultimately directed at one or more of the structures that can produce hypopharyngeal obstruction: the oropharyngeal lateral walls, tongue, and epiglottis. In contrast, skeletal surgery enlarges airway dimensions along the entire length of the pharynx without a specific focus on individual structures.
The role of the history in detection of hypopharyngeal obstruction is limited, as no studies have indicated that any of the common OSA signs and symptoms are unique to hypopharyngeal obstruction. The same is true for sleep study results, as the apnea-hypopnea index (AHI) has not shown a consistent or strong association with patterns of obstruction or specific involved structures. However, these evaluations help determine the severity of OSA and its burden and, therefore, the aggressiveness of treatment.
In contrast, physical examination can identify factors that can be highly suggestive of hypopharyngeal obstruction.
Table 138.1 lists some evaluation techniques that have been used for pharyngeal examination, with the goal of characterizing the pattern of airway obstruction. Because obesity and weight gain are well-established risk factors for OSA (
1), measurement of the height and weight (with calculation of body mass index (BMI), a commonly used but crude measure of obesity) is an essential component of physical examination, as is questioning about changes in body weight and an association with signs or symptoms in the patient history. There are multiple mechanisms that may explain the association between increased body weight and OSA, including an increase in soft tissue mass surrounding the pharyngeal airway and decreased lung volumes that develop with increases in body weight. Magnetic resonance imaging (MRI) studies have demonstrated that weight loss results in a decrease in lateral pharyngeal wall volume (
3). Increases in body weight may also result in fat deposition within the tongue base, based on a higher fat content of that tissue, relative to other portions of the tongue, shown with computed tomography (CT) (
4) and a correlation between BMI and fat content of the tongue base that was notably stronger than for other parts of the tongue (
5). BMI and changes in body weight are major
factors in treatment outcomes, and these are discussed later in this chapter.
In addition to measurement of body weight and BMI, visual examination of the oral cavity, including the tongue, tonsils, mandible, and lateral pharyngeal walls, can prove invaluable. The modified Mallampati position reflects absolute tongue size, soft palate length, and the dimensions and position of the mandible (which define the space for the tongue) (
6,
7). The combination of modified Mallampati position, tonsil size (according to the Brodsky classification), and BMI enables classification according to Friedman stage, which has demonstrated a stronger association with outcomes after uvulopalatopharyngoplasty (UPPP) with tonsillectomy than the AHI has (
6,
8). The improvement in outcomes for a combination of hypopharyngeal surgery (submucosal tongue radiofrequency) and UPPP with tonsillectomy, compared to UPPP with tonsillectomy alone, in Friedman stage II and III patients (
9) suggests that these groups have at least some component of hypopharyngeal obstruction and that the Friedman stage can play an important role in considering hypopharyngeal procedures.
The position and dimensions of the mandible and dentition can contribute to OSA and affect treatment outcomes. The mandible is an important component of the bony framework housing the soft tissues surrounding the upper airway, and both retrognathia and mandibular deficiency/insufficiency compromise the airway, particularly the hypopharyngeal airway. Examination of the mandible can occur with direct inspection, indirect evaluation based on the dental occlusion, or imaging studies. Direct inspection is the simplest technique. Dental occlusion is commonly defined by the Angle classification comparing the position of the mesiobuccal cusp of the maxillary first molar to the buccal groove of the mandibular first molar. This can reflect the mandible position and size relative to the maxilla, but two limitations are that the Angle classification can be affected substantially by dental and orthodontic treatment, including dental extractions, and that relative position and size of the mandible may not be as important as absolute measures (also true for the maxilla). Multiple imaging modalities can assist in evaluation of the mandible, and of these, lateral cephalometry has been studied most extensively in OSA. Although somewhat limited as a two-dimensional assessment of the airway, lateral cephalometry can image multiple aspects of bony and soft tissue anatomy. Individuals with OSA and normal BMI have demonstrated retrognathia (decreased sellanasion-mandible B point angle, or SNB angle), a narrowed space between the tongue base and posterior pharyngeal wall (posterior airway space), and an increased distance between the mandible and hyoid bone (mandibular plane-hyoid distance) (
10). Findings of lateral cephalometry have also demonstrated an association with outcomes after certain hypopharyngeal procedures, and these findings are discussed later in this chapter.
There is no standardized or objective assessment of the lateral pharyngeal walls during physical examination. Subjectively, certain factors may suggest a greater contribution of the lateral walls to airway obstruction: their thickness (determined indirectly by visual inspection of the pharyngeal aspect), folds or redundancy in the mucosa covering the underlying musculature (suggesting increased thickness and/or tissue laxity), and any narrowing of the transverse dimensions of the pharyngeal airway that can occur with thickened walls. MRI offers the most detailed assessment of the lateral pharyngeal walls, but currently it is used solely for research purposes. Improved methods for examination of the lateral pharyngeal walls will likely contribute substantially to understanding OSA and treatment outcomes.
Awake fiberoptic endoscopy is an invaluable tool for evaluating not only the nasal and retropalatal regions but also the hypopharyngeal region. Indirect laryngoscopy can inspect the larynx and tongue base, but its use in OSA is limited for three reasons. First, many individuals with OSA have a large tongue that impairs visualization of the hypopharynx due to physical blockage of the line of sight and/or increased likelihood of triggering a gag reflex. Second, indirect laryngoscopy requires mouth opening and tongue retraction, both of which disturb the natural anatomy of the hypopharyngeal airway. Third, it does not allow visualization of the hypopharyngeal airway under varying clinical states. Fiberoptic laryngopharyngoscopy enables a more-detailed evaluation of the hypopharyngeal airway and the individual structures surrounding it under various conditions, making it a mainstay of hypopharyngeal evaluation. The airway caliber, site of narrowing, and surrounding structures (tongue base, lateral walls, and epiglottis) can be seen under conditions such as mouth open versus closed, during snoring versus restful breathing, inspiration versus end-expiration, upright versus supine, mandible advanced forward versus neutral position, and with increased negative intrathoracic pressure (Muller maneuver). The Muller maneuver can be performed during awake endoscopy, but there are no reported studies related
to hypopharyngeal procedure selection or outcomes. Subjective evaluation of airway dimensions and structures using endoscopy can provide important and useful information (
11), but there are currently no commonly used, standardized, and objective measurements.
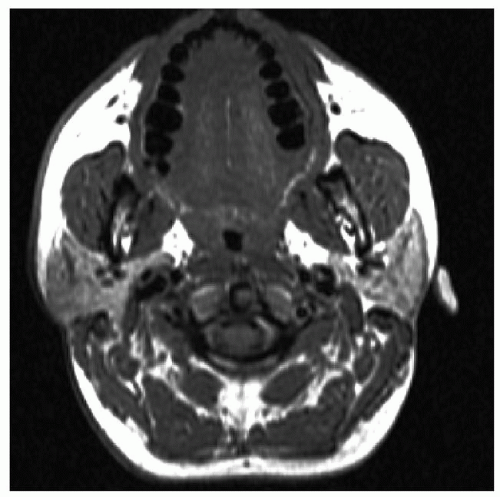
Studies based on MRI (
Fig. 138.1) (
12) and CT (
4), in addition to a number of other modalities such as acoustic methods, airway pressure sensing, optical coherence tomography (
13), and computational fluid dynamics (
14), have provided a greater understanding of anatomical abnormalities among individuals with OSA and, to some extent, outcomes after palate procedures. Thus far, they have largely been limited to research purposes or surgical planning. However, these studies have important limitations for this discussion, for three reasons: most of these studies have been performed during wakefulness, they have generally characterized all hypopharyngeal region obstruction as similar without differentiation among possible subtypes, and, other than the lateral cephalogram, they have not been examined for a possible association between imaging findings and outcomes after hypopharyngeal procedures or skeletal surgery. The first two limitations are discussed here.
Airway examination during wakefulness—whether physical examination, endoscopy, or imaging—has important limitations related to the physiologic changes that occur during sleep, such as the marked decrease in genioglossus muscle tone that occurs at sleep onset (
15) and the further decrease in rapid eye movement (REM) sleep (
16). Of course, individuals with OSA demonstrate airway obstruction only during sleep, often with increased frequency during REM sleep. The implications for evaluation of hypopharyngeal airway obstruction (especially that related to the tongue) may be substantial. Although awake evaluation, especially office examination, generally has relatively low cost, there are likely important differences between examinations performed during wakefulness and sleep, and further investigation will elucidate how important those differences are.
Multiple investigators have studied the airway under conditions of anesthesia, including drug-induced sleep endoscopy (DISE) (
17), originally described as sleep nasendoscopy in 1991 (
18). The continuum of sedation ranges from wakefulness to conscious sedation to unconscious sedation to general anesthesia, and DISE involves endoscopic examination of the pharyngeal airway during unconscious sedation. While unconscious sedation under propofol may not be a perfect simulation of natural sleep, with identical effects on upper airway collapsibility, pharyngeal dilator muscle activity during DISE appears to lie somewhere between natural non-REM and REM sleep (
15,
16,
19,
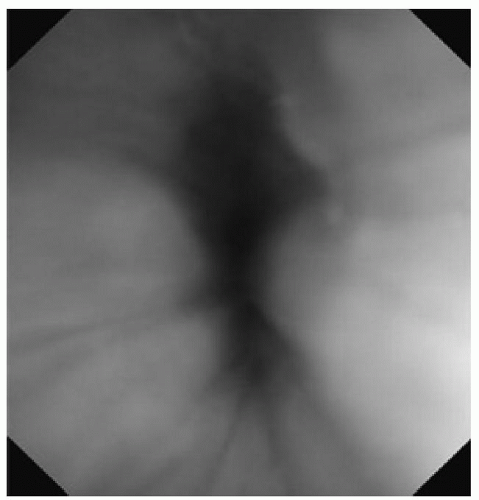
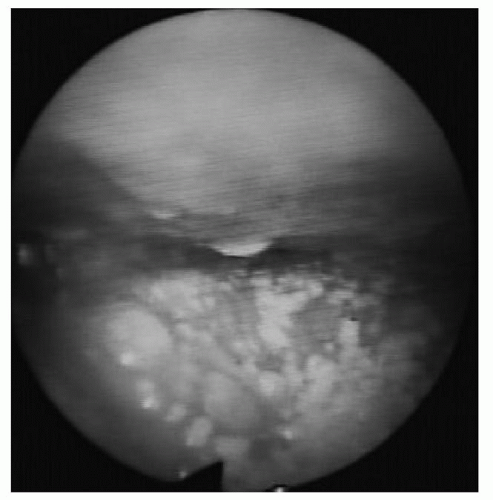
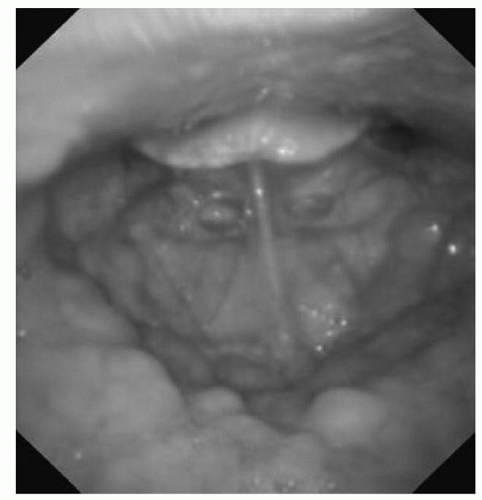
20). DISE findings have suggested that there may be multiple subtypes of hypopharyngeal region obstruction; during unconscious sedation, individuals with OSA generally have one or more of the following structures contributing to hypopharyngeal obstruction: the oropharyngeal lateral walls, tongue, and/or epiglottis (
Figs. 138.2,
138.3,
138.4, respectively) (
17,
21). Although hypopharyngeal procedures are ultimately directed at specific structures (including these three), it remains unclear whether this diversity of patterns within the broader category of hypopharyngeal obstruction has implications for outcomes of surgical and nonsurgical treatment (i.e., whether tongue-directed procedures work better in individuals with tongue-related hypopharyngeal obstruction than in those with obstruction more related to the oropharyngeal lateral walls or epiglottis). It is possible that alleviation of one source of airway narrowing/obstruction
may alleviate that from others, for example, by reducing resistive Bernoulli forces. Thus, the interaction of anatomy, physiology (e.g., depth of sleep, collapsibility, and ventilatory control), airflow dynamics, and conditions (e.g., body position) is complex. At a minimum, the grouping of all hypopharyngeal region obstruction together, as has occurred with most evaluation techniques, does not capture this diversity. Although DISE findings have demonstrated an association with outcomes for palate surgery (
22,
23), similar evaluations have not occurred for hypopharyngeal procedures.
The importance of preoperative evaluation—and the association between findings of the preoperative evaluation and surgical outcomes—cannot be overemphasized.
The next section discusses outcome assessment, followed by the available hypopharyngeal procedures and skeletal surgery and their reported outcomes, highlighting the factors that may be apparent during preoperative evaluation that have shown an association with outcomes, as well as their risks.